Article Text

Abstract
Objectives Life-long adherence to health-enhancing physical activity (PA) is a major challenge for people with rheumatoid arthritis (RA). Our aim was to evaluate the utilisation of and experiences with a RA-specific, mobile internet PA support service, ‘tRAppen’, developed through a co-design process.
Methods 28 participants with RA formed 3 web communities and tested tRAppen for 6 weeks. A mixed-method design was used to combine different types of data. Log data and questionnaire data were analysed quantitatively, while data from telephone interviews were analysed with a directed content analysis.
Results 25 of the 28 participants used tRAppen. Log data indicated that a majority of them registered their PA, sent likes and posted comments to peers, set personal goals and made exercise plans. tRAppen was rated as easy and fun to use, and fairly informative and supportive for PA, and was highly recommended for people with RA. The interview analysis resulted in the following 6 categories describing the utilisation of and experiences with tRAppen: (1) experiences in general, (2) feasibility of features, (3) value as support for PA, (4) enjoyment, (5) ideas for improvements and (6) additional factors.
Conclusions tRAppen is the first co-designed mobile internet service developed specifically for the self-management of PA in people with RA. The results are promising and indicate that tRAppen may be useful for supporting a physically active lifestyle in a subpopulation at certain risk of poor health. It will now be revised, launched and continuously updated in an iterative process involving its future users.
- Rheumatoid Arthritis
- Physcial therapy
- Health services research
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Life-long adherence to health-enhancing physical activity (PA) is a major challenge for most people with rheumatoid arthritis (RA).
To date, there is no evidence-based mobile internet service available focusing on self-management of PA adapted to the specific needs of people with RA.
What does this study add?
People with RA reported the co-designed RA-specific mobile internet service, tRAppen, to be feasible and to provide support for PA in a subpopulation at certain risk of poor health.
Variations in disease activity, PA level and personal preferences were perceived as affecting the utilisation of, and experiences with, the service and, hence, highlights the importance of customising tRAppen according to individual preferences.
How might this impact on clinical practice?
tRAppen could complement supervised exercise provided in rheumatology care and make an evidence-based healthcare service available to more patients for use in everyday life, thus contributing to their long-term health.
Introduction
Life-long adherence to health-enhancing physical activity (PA)1–3 is recommended to prevent disability and co-morbidity in people with rheumatoid arthritis (RA). A physically active lifestyle demands self-management, which is influenced by personal, environmental and behavioural factors, and self-regulation skills.4–6
The internet has the potential to reach large populations, bring self-management interventions into people's everyday lives and be cost-effective.7 ,8 A large number of commercial PA mobile applications are available, but they are seldom evidence-based and are not tailored to the specific needs of people with RA.9 ,10 Among six identified, evidence-based, internet-accessible programmes targeting medication and disease management,11 only one, the Arthritis Self-Management Programme,12–16 includes PA tracking. Nine RA-specific recently identified mobile applications17 were primarily classified as educational, including information on the disease and the medications used to treat it. To date, there is no evidence-based mobile internet service available for people with RA to self-manage PA.
User involvement is a truism in health informatics18 ,19 when producing viable, effective and usable internet services. Co-design is one strategy to involve users in the production of services and includes the active involvement of users of the future service throughout the development process in collaboration with researchers, clinicians and service designers.20 Co-design has been used successfully to improve healthcare services.21 ,22
The present project employed a co-design process to develop a mobile internet service, called tRAppen, for the self-management of PA in people with RA. The first step of the co-design process, the needs inventory phase, involved people with RA who generated and prioritised ideas on core features to include in the future service.23 Second, in a series of workshops, people with RA, researchers, a clinical physiotherapist, an e-health strategist and a representative from the patient organisation specified two essential components of the future service: peer support and self-monitoring, including goal setting, activity planning and feedback.24 The present paper aimed at reporting the results from the third step, which included the users' utilisation of and experiences with the first test version of the new service.
Methods
Design
A mixed-methods design was used25 to explore the utilisation of and experiences with tRAppen during a 6-week test period during December 2014 to January 2015. Data collection included system-generated and manually compiled log data from the test period, as well as answers to a web questionnaire and data from semistructured telephone interviews obtained after the test period. The Regional Ethical Review Board in Stockholm approved the study (D.nr. 2014/1522-31/2).
Participants
Designated contact people, including physiotherapists, an occupational therapist and a physician, recruited participants from three rheumatology clinics and one primary care clinic in three cities in central Sweden. Individuals with diagnosed RA who were ≥18 years of age, had adequate Swedish communication skills, were comfortable using the internet and had access to a mobile phone, were eligible. A sample of approximately 30 participants was needed to form three sensibly sized communities. This was considered enough to evaluate the test version in term of the utilisation of and experiences with the service. Thirty-four interested individuals received verbal information on the study. Twenty-eight individuals, who either participated in a face-to-face introductory meeting (n=24) or received individual information (n=4) to acquaint them with tRAppen and the study set-up, provided written consent and constituted the study sample (table 1). The participants formed three communities (n=7–11), one in each city.
Baseline characteristics of the study participants (n=28*)
tRAppen overview
An existing, flexible online service with peer support for PA was identified as suitable for tRAppen, enabling lower costs and quicker development. To provide the features identified during previous workshops in the co-design process, the service was complemented with features for self-monitoring, including goal setting, PA planning and feedback. Thus, the tRAppen test version evaluated in the present study was a peer group self-management service to support everyday PA and consisted of two main components: (1) a small community with peers for inspiration and support, and (2) a self-monitoring component, including personal goal setting, PA planning and feedback. The aim of tRAppen is to provide support to each individual's PA behaviour and not to objectively monitor what they actually do by pedometers, accelerometers, etc. Thus, all data are self-reported.
Before the test period started, each community participant was invited to a meeting to get an introduction to tRAppen and to meet with peers. The meeting started with each participant introducing himself or herself to the other. The study set-up was presented (the test period and the assessments) and the features of tRAppen were shown on a screen. How to set goals, how to register PA and what PAs to register were discussed. All participants also logged on to tRAppen through a log-in link provided by email before the meeting. The website was bookmarked for easy access. The participants were told to use the tRAppen features as described below.
When accessing the tRAppen welcome screen (see online supplementary appendix 1a), photographs of every community member are shown in a dynamic order (left to right), determined by the time from past PA registration. A heart symbol for sending ‘peps’, that is, indicating encouragement that will be displayed along with the user's name, to the peer with the longest inactivity period, is provided. A speech bubble under each photograph enables easy, direct email communication. A display of the user's own long-term outcome goal, PA behavioural goal and weekly PA plan is provided. A guide with evidence-based information on the importance of PA for people with RA, recommendations for health-enhancing PA,31 ,32 instructions on SMART (Specific, Measurable, Acceptable, Realistic, Time set) goal setting and planning,33 ,34 and instructions on features is provided via a link.
Supplemental material
Another screen for registering PA, uploading images and talking to peers, that is, asking questions and sharing experiences and knowledge (see online supplementary appendix 1b), is also provided. Peers' postings of PA performances can be accessed, and comments can be provided as free text or as ‘likes’, that is, indicating support by clicking a thumbs-up icon that will be displayed along with the user's name (see online supplementary appendix 1c).
A statistics screen provides feedback on the user's own PA performance as well as information on peers' performances. A dashboard with statistics on the total number of PA occasions during the past month, mean number/week, mean minutes/occasion and mean minutes/week during the same period is provided for the user and for the peer community, along with a ranking of the members based on PA performance the previous month. A feature to facilitate competition between different peer communities is also provided. A detailed PA log, a circle diagram showing the PA types performed (see online supplementary appendix 1d), and monthly awards for such aspects as best performance/improvement and best support are provided. Different types of feedback are also provided by weekly emails, generated by the system or provided manually (ÅR). Feedback includes updates with system-generated statistics on personal and peer ranks, and manually generated personal feedback on goal achievement and standardised reminders to encourage PA planning. The feedback also includes encouragement to review goals that have not been achieved. Real-time email notifications on peers' performances are provided continuously.
Data collection
The system-generated log data consisted of the frequency of likes and peps sent, comments posted, images uploaded, and PA registered. Data on the frequency of goal setting, goal changing and PA planning were manually compiled after the study period by the first author.
A study-specific web questionnaire, based on the Unified Theory of Acceptance and Use of Technology,35 was used to assess the features for peer support, self-monitoring and feedback (see online supplementary appendix 2). It included participants' ratings of tRAppen in general, its feasibility and the value of its support for PA. Ratings were assigned using Likert-type items with five or six response options (‘totally agree’—‘do not agree’; or ‘to a very high extent’—‘not at all’), including the answer ‘not used/received’. The first draft of the questionnaire was reviewed by an expert group in behavioural medicine and physiotherapy. After subsequent editing, the questionnaire was tested by two of the authors (HA and PÅ), which resulted in minor refinements.
The semistructured telephone interviews covered experiences with tRAppen in general and its specific features. The main questions were: What was your experience with tRAppen? What did you particularly like/dislike about tRAppen? Do you have any suggestions for improvements? Probes and follow-up questions were used to learn more about the experiences with respect to specific features. The interviews were recorded and saved electronically on an external hard drive.
Data analysis
Descriptive data are presented as frequencies (n, %) or medians (md) with ranges (minimum–maximum). The telephone interviews were transcribed and analysed with a deductive approach using directed content analysis.36 Three predefined categories based on the structure of the web questionnaire were used: (1) experiences with tRAppen in general, (2) feasibility of features and (3) value of features as support for PA. Two subcategories for each of these three categories were created to reflect positive experiences and those that were less satisfactory. Meaning units were initially identified and sorted into these two subcategories by Atlas.ti software. Operational definitions of categories, including additional categories that emerged during analysis and subcategories, were refined during the coding process. Meaning units were compared to assess similarities and differences in content, and similar meaning units were assigned a unifying code.
The first four interviews were analysed separately by two authors (ÅR and SP) to ensure credibility. Disagreements in coding and definition of the categories and subcategories were discussed until consensus was reached on how to interpret the meaning units, and define the categories and subcategories. The same procedure was repeated after coding half of the interviews. The remaining interviews were coded by ÅR alone. Next, tables were developed to present the link between the codes, subcategories and categories.
Results
Twenty-five of the 28 participants used tRAppen, 2 logged on but did not use it and 1 withdrew from the study for personal reasons.
Log data were available for 25 participants and indicated that the majority of participants registered their PA, sent likes and posted comments (table 2). Twenty-four participants set goals and 21 made exercise plans. Six participants changed their goals once or twice during the test period.
Use of tRAppen features among 25 participants during the 6-week test period
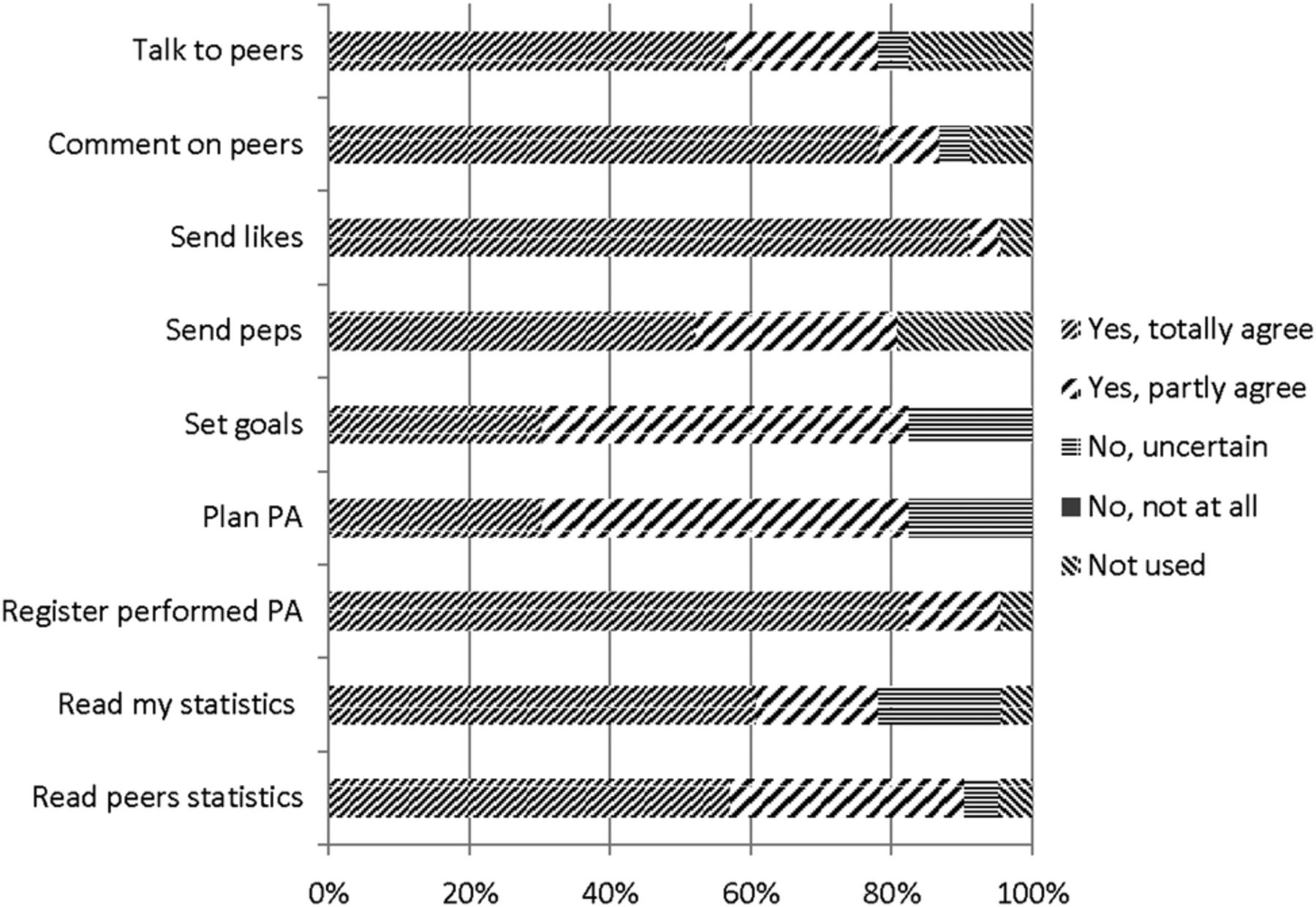
The web questionnaire was completed by 24 participants, and 1 only answered the questions regarding the experiences of tRAppen in general. All the other 23 participants answered all the questions included in the questionnaire. Eighteen (78%) participants primarily accessed tRAppen via a mobile phone, 3 (13%) via a computer and 2 (9%) via a tablet. tRAppen was generally rated as easy and fun to use, and as providing sufficient PA support and information, and all participants reported that they would recommend it to other people with RA. More than 60% claimed that they would continue to use tRAppen (figure 1). tRAppen features were generally rated as easy to understand and use, but almost 20% of participants were uncertain regarding the feasibility of goal setting and PA planning (figure 2). The highest-ranked support feature was planning and registration of PA, while talking to peers was ranked as the least helpful support feature (figure 3).
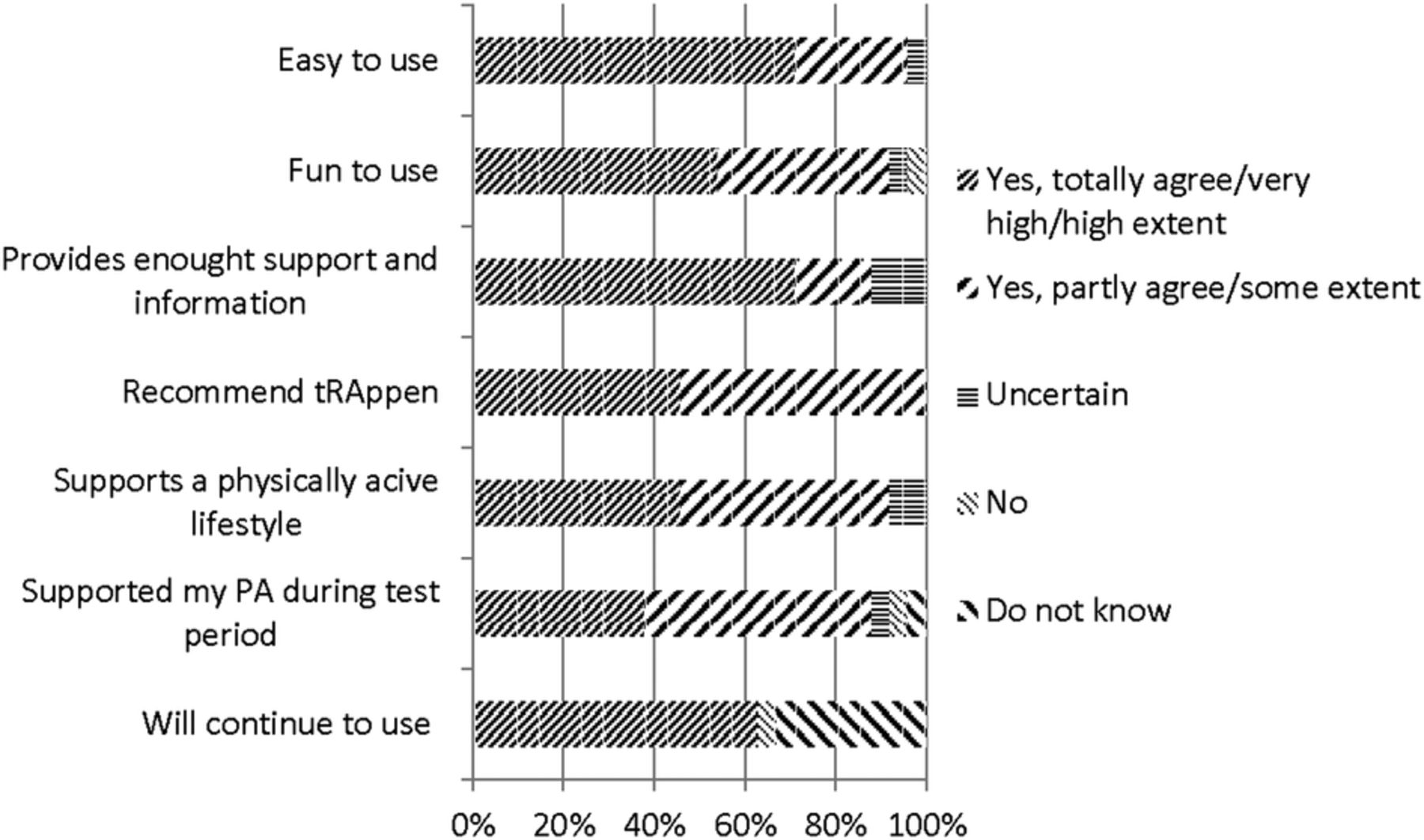
Participants’ (n=24) rating of tRAppen in general. PA, physical activity.

Participants’ (n=23) ratings of the feasibility of individual tRAppen features. PA, physical activity.

{kind=link}
{kind=link}
{kind=link}
Participants’ (n=23) ratings of individual tRAppen features with respect to PA support. PA, physical activity.
Twenty-six telephone interviews were conducted. The results of the analysis are presented in the following six categories, three of which were predefined, namely, (1) experiences with tRAppen in general, (2) feasibility of features and (3) value of features as support for PA, and three of which emerged during analysis, namely, (4) enjoyment, (5) ideas for improvements and (6) additional factors important for the utilisation and experience (table 3).
Overview of the results from the qualitative analysis of the telephone interviews on participants' experiences of tRAppen presented as categories, subcategories and codes
Discussion
The overall results demonstrated that the majority of the participants found tRAppen easy and fun to use, and believed it would support a physically active lifestyle. The outcome of the qualitative analysis, however, indicated a rather complex picture with a large variety of preferences for and against different tRAppen features, some of which were clearly RA-specific and related to variations in the physical as well as mental state.
The observation of peers' performances may improve self-efficacy for engagement in PA, which is a powerful method of behavioural learning.4 The peer community provided by tRAppen thus constituted an important PA support group for people with RA, as demonstrated by our results. However, the qualitative statements also revealed that the need for sharing and reading about peers' performances may vary with PA levels and personal preferences. Some participants wanted to share more, whereas others wished to stay somewhat anonymous, and still others preferred to use tRAppen entirely without peer support. Previous research on people with cancer revealed similar views.37 The informants wished to share personal information, but actual sharing varied with personal characteristics and type of information shared (clinical or private). The benefits of actively sharing personal information with others must be perceived as higher than the risk of disclosing it. Thus, tRAppen may have an advantage over commercial PA mobile applications that provide social interaction38 ,39 because sharing information within a small community of people with RA is presumably valued more highly than sharing within a broader community. Nevertheless, the tRAppen peer support features may need to be redesigned to enable more flexible use, and criteria for peer community assignments could be further developed.
Both theory and evidence support the importance of personal goal setting for PA, planning, registration and feedback, on performance for the development of self-regulation skills to initiate and maintain PA.5 ,40 Most commercial PA mobile applications do not include PA planning and goal setting,38 ,39 ,41 and the need for self-monitoring features seemed to vary among participants in the present study. One reason for the varying needs was variations in disease activity and PA levels, and another reason was perceived obstacles to setting realistic goals and plans in general, and using the tRAppen features for this aim specifically. Furthermore, most participants did not revise goals according to variations in disease activity and well-being, although this feature was identified as important in the preceding requirement-specification phase of tRAppen development.24 Different obstacles to the registration and planning of PA have previously been described by people with RA participating in face-to-face PA support groups42 and do not seem to be specific to internet support of PA in general or to tRAppen in particular. Nevertheless, this is an area for further exploration and improvement when designing PA support interventions targeting people with RA.
Another area to explore further is the methods of encouraging feedback. Our results indicated that the participants reacted differently depending on disease activity, PA levels and personal preferences. Because theory and evidence suggest that features supporting self-regulation skills should be included in tRAppen,5 ,40 it is a challenge to make them adjustable to guide goal setting and PA planning according to individual preferences, and to provide optimal feedback to each user.
Some methodological issues should be taken into consideration when interpreting the present results. The mixed-methods design that provided detailed and complementary data is a true strength that enabled full understanding of the utilisation of and experiences with the tRAppen test version and will also be valuable in the process of further improving it. There are clearly some limitations with respect to the generalisability of our results because our participants had been regularly physically active before disease onset, and most of them were well educated, worked and scored low on the Health Assessment Questionnaire Disability Index (HAQ). Thus, our results may be generalised to this subpopulation only, but they may also be transferable to similar populations with other chronic diseases. Future studies of tRAppen should include people with lower education, to evaluate whether it is feasible and useful for them too. The limited sample and fairly short test period may also be considered limitations of our study. However, as this was the first evaluation of tRAppen, which aimed to identify necessary improvements of its features according to participants' utilisation and experiences in a real-life setting, the sample and the test period could be considered sufficient. Systems are in place to monitor and report on long-term use once tRAppen is launched.
One limitation of the tRAppen test version evaluated in the present study may be that the specific features developed to satisfy requests from the requirement-specification phase,24 that is, for goal setting and PA planning, were less developed and tested than the peer support feature already included in the existing generic PA support service used as the basis of tRAppen. Furthermore, it may be considered a limitation that tRAppen contains self-reported PA only. However, while self-report is adequate to support individual PA behaviour change, future research on tRAppen could, depending on the research questions, be complemented with objective measures of PA and/or health outcome data.
The most important and unique strength in the development of tRAppen is the co-design process.23 ,24 ,43 To our knowledge, such a thorough process has not previously been applied nor scientifically evaluated in the development of any e-health service within the field of rheumatology. Thus, our co-design process may serve as a model for the development of future e-health services in this field at a time when many such services are in development.17 The involvement of people with RA throughout the development process improve the credibility of tRAppen and the likelihood that it will support a physically active lifestyle in this subpopulation. The next step in the development will be to revise some of the features based on the current results, which provide clear descriptions of preferences but also highlight the complexity of providing a self-management service for a heterogeneous group, such as the RA population. The revised version will then be launched and continuously improved in an iterative process involving future tRAppen users.
In conclusion, the present results are promising and indicate that tRAppen may be useful for supporting a physically active lifestyle in a subpopulation at certain risk of poor health. tRAppen could complement supervised exercise provided in rheumatology care and make an evidence-based healthcare service available to more patients for use in everyday life, thus contributing to their long-term health. Because variations in disease activity, PA level and personal preferences seemed to affect the utilisation of and experiences with the features, the ability to customise tRAppen to individual preferences would be helpful and should be considered in future versions. Further research is needed to evaluate the best target users for tRAppen and its effects on PA behaviour and health.
Acknowledgments
The authors would like to thank the study participants; the physiotherapists at Västerås Hospital; the occupational therapist, physiotherapists and physician at Karolinska University Hospital at Solna and Huddinge; the physiotherapists at Uppsala University Hospital; and the physiotherapist at Nacka Rehabilitation Center.
References
Footnotes
Contributors The study was performed at Karolinska Institutet and Uppsala University in collaboration with the Stockholm County Council 4D-project, the Swedish Rheumatism Association and the We+ Company. ÅR was involved in the design and planning of the study, data collection, data analysis, and manuscript writing. PÅ was involved in the design and planning of the study, analysis, and manuscript writing; CHO participated in the planning of the study, data analysis and manuscript writing; SP participated in the data analysis and manuscript review; HA and MB participated in the planning of the study and manuscript review. All the authors read and approved the final manuscript.
Funding The study was funded by the Karolinska Institutet part-time financing of doctoral students (KID), the Vinnvård Foundation, the Combine Sweden, the Swedish Rheumatism Foundation, the Stockholm County Council 4D and the Strategic Research Program in Health Care Research at Karolinska Institutet.
Disclaimer The sponsors had no involvement in the study design, data collection, and analysis, the writing of the report, or the decision to submit the report for publication.
Competing interests None declared.
Ethics approval The Regional Ethical Review Board in Stockholm approved the study (D nr 2014/1522-31/2).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.