Article Text

Abstract
Objectives To identify whether children with antenatal prednisone exposure have chronically elevated cortisol and cortisone concentrations, an altered body composition or higher blood pressure. In addition, to identify whether maternal rheumatoid arthritis disease (RA) activity is associated with these alterations.
Methods In this prospective study, 56 children (mean age=10.0 years) with and 61 children (mean age=9.6 years) without antenatal prednisone exposure, born to women with RA, were included. Hair cortisol and cortisone were analysed using liquid chromatography–tandem mass spectrometry. Linear regression models were built to analyse differences between the two groups, corrected for relevant covariates. Hair cortisol concentrations were also compared between the study population and an age-matched healthy reference group(n=150 children, mean age=9.8 years).
Results Hair cortisol and cortisone concentrations were similar in children with and without antenatal prednisone exposure (median cortisol 1.14 pg/mg (IQR 0.67–1.75) and 1.15 pg/mg (IQR 0.65–2.21) and median cortisone 6.76 pg/mg (IQR 5.42–8.86) and 7.40 pg/mg (IQR 5.39–10.73), respectively). Antenatal prednisone exposure and maternal RA disease activity were also not associated with body composition or blood pressure. Hair cortisol concentrations were not different in children born to mothers with RA compared with children from the reference group.
Conclusion This, in its kind, large and unique long-term prospective study demonstrates that low-dose antenatal prednisone exposure and maternal RA disease activity are not associated with negative consequences in prepubertal childhood. The findings of this study are reassuring and support the assumption that low-dose maternal prednisone use during pregnancy is safe for the offspring, at least until the age of approximately 10 years.
- pregnancy
- prednisone
- cortisol
- rheumatoid arthritis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Research on the long-term consequences of antenatal prednisone exposure has been limited.
What does this study add?
In this unique nationwide study, the majority of the participants were followed prospectively during and after pregnancy.
Scalp hair measurement of cortisol and cortisone is considered the most optimal method for long-term concentrations.
Low-dose antenatal prednisone exposure and maternal disease activity are not associated with long-term negative consequences in prepubertal childhood.
How might this impact on clinical practice?
The findings of this study are reassuring for women with an autoimmune disease who use low-dose prednisone during pregnancy.
Ideally during pregnancy, women would not use any medication; however, sometimes it is inevitable, like the use of corticosteroids in autoimmune disorders. In animal studies, it has been shown that an excess of maternal glucocorticoids during pregnancy, for example, administration of synthetic glucocorticoids, is associated with altered hypothalamic-pituitary-adrenal (HPA) axis activity with higher plasma cortisol levels of the offspring, higher blood pressure, hyperglycaemia and visceral obesity in later life.1–7
There are also several human studies demonstrating that adverse circumstances during pregnancy, that are related with cortisol concentrations in the mother (eg, maternal stress,8 maternal depression9–11 and maternal anxiety during pregnancy12–14), result in elevated cortisol concentrations and an altered cortisol response in the offspring. Chronically elevated cortisol levels are associated with an increased risk of abdominal obesity, hypertension, non-insulin dependent diabetes mellitus and cardiovascular disease.15–20
Maternal cortisol rises throughout pregnancy, but normally only 10%–20% reaches the fetus due to the oxidation of cortisol to cortisone by 11beta-hydroxysteriod dehydrogenase type II (11βHSD2) enzyme in the placenta.21–23 Cortisone can be reverse metabolised into cortisol.24 The 11βHSD2 enzyme also converts the active prednisolone into its inactive metabolite prednisone.25 Despite the presence of this enzyme, children born to mothers who use prednisone during pregnancy could be exposed to higher concentrations of corticosteroids in utero in at least three different ways.
First, since the placenta is not fully developed before 12 weeks of gestation, in that period passive diffusion of prednisolone to the fetus takes place.26 Second, the capacity of the 11βHSD2 enzyme may be exceeded by the external administration of corticosteroids,26 27 resulting in increased placental availability of prednisolone. Finally, the activity of 11βHSD2 is downregulated by the proinflammatory cytokines tumour necrosis factor (TNF), interleukin (IL)-1 and IL-6, which are elevated in autoimmune disorders like rheumatoid arthritis (RA),26 28 resulting in decreased inactivation and increased availability of prednisolone.
Exposure to higher corticosteroid concentrations in utero may influence the development of the fetal HPA-axis, with reduced negative feedback due to reduction in hippocampal glucocorticoid receptor expression.2 As a result, this may lead to an overactive HPA-axis and elevated circulating glucocorticoids in the offspring.2
De Steenwinkel et al 26 reported that children born to mothers with RA who used prednisone during pregnancy had higher salivary cortisol levels at the age of approximately 7 years, independent of RA disease activity of the mother during pregnancy.26 However, there was no association with physical signs of higher cortisol levels. The main limitation of that study is that the analysis of cortisol was from a single day saliva sample collection, which is a useful method to study acute HPA-axis reactivity, but is not a good reflection of long-term cortisol levels.29 30
Since then, a new method has become available to measure both long-term cortisol and cortisone concentrations in scalp hair.31 Several studies have shown that this is a reliable, non-invasive method to measure endogenous cortisol and cortisone, in adults32–35 and in children.30 36 37 Hair cortisol is a reflects long-term cortisol exposure.30 It has been shown that obese children have higher hair cortisol concentrations compared with non-obese children.24 30 Furthermore, in a large population-based cohort, hair cortisol concentrations were already associated with body mass index (BMI) and adverse body fat distribution in children at young age (mean age of 6 years).38 Also, children’s hair cortisol levels have been shown to be associated with stress at school entry.37
Hair cortisol and cortisone analysis could provide more information about the long-term consequences of antenatal prednisone exposure.
In the current study, we investigated whether children with antenatal prednisone exposure have signs of altered HPA-axis activity, reflected by chronically elevated hair cortisol and cortisone concentrations, an altered body composition (risk factors for future cardiovascular and metabolic disease) or higher blood pressure compared with children without antenatal prednisone exposure. In addition, since proinflammatory cytokines may cause downregulation of 11bHSD2 followed by increased transfer of prednisolone to the fetus, we analysed the associations between maternal RA disease activity during pregnancy and the earlier mentioned outcome measures in childhood.
Methods
Study population
In a previous study26 that showed that antenatal prednisone exposure is associated with elevated cortisol concentrations in saliva at the age of approximately 7 years, 42 children with and 63 children without prednisone exposure were included. Hair cortisol concentrations correlate with long-term salivary cortisol production measured over a 1-month period.32 Therefore, in order to acquire enough power in this prospective cohort study, we aimed to include comparable numbers of participants. In this study, a total of 56 children with (prednisone dose ≥5 mg/day, during at least 2 trimesters of pregnancy) and 61 children without antenatal prednisone exposure born to women with RA, aged 515 years, were included between 2014 and 2018.
First, children born to women who participated in the Pregnancy induced Amelioration of Rheumatoid Arthritis (PARA) study were included, a nationwide prospective cohort study on RA and pregnancy and onwards from the Netherlands.39 The PARA study has been described in detail elsewhere.39 In the PARA study, patients with RA who met the 1987 revised American College of Rheumatology criteria40 with a wish to conceive or already pregnant, were enrolled between 2002 and 2008 (last visit in 2010).
Second, siblings of the children born to PARA-participants were included (if their mother was already diagnosed with RA before pregnancy). Finally, after the inclusion was not sufficient, children born to women with RA who visited the outpatient clinic of the department of Rheumatology in the Erasmus MC Rotterdam, the Netherlands, were included to accomplish the intended number of inclusions. At this outpatient clinic, RA disease activity and medication use during pregnancy are properly recorded.
In total, 97 children born the PARA study participants, 14 siblings and 6 children born to women who visited the outpatient clinic were included. Exclusion criteria were: congenital abnormalities, chronic illness of the child, non-Caucasian ethnicity, scalp hair shorter than 2 cm.
Reference population
As a reference population, 252 healthy children born to women from the general population were used. These children had been recruited, as described in more detail elsewhere.41 Briefly, children were eligible for inclusion if they were between the age of 4 and 18 years, did not use glucocorticoids 3 months prior to or during the study and did not suffer a chronic disease. Healthy controls were recruited from primary and secondary schools in the Netherlands and among siblings of children attending the paediatric outpatient clinic.41 For comparison with the current study, only data on Caucasian children between the age of 5 and 15 years was used, resulting in 150 participants in the reference group.
Data collection
Data collection during pregnancy
In the PARA-study, participants were visited at their home address before pregnancy (if possible), three times during pregnancy and three times after the birth of the child (at 6, 12 and 26 weeks). At all time-points, data on mother and child were collected. RA disease activity was measured using the Disease Activity Score based on 3 variables; swelling and tenderness by palpation in 28 joints and a C reactive protein (DAS28-CRP(3)). For participants whose mother did not participate in the PARA study, information on their disease activity and medication use during pregnancy, pregnancy course and pregnancy outcome (from 1 year before delivery until 1 year after delivery) was obtained from their rheumatologist and gynaecologist.
Hair collection
Participants were visited at their home address once during the study period. During this visit, a lock of 3 cm with approximately 100 hairs was cut from the posterior vertex of the child’s scalp, as close to the scalp as possible. There is a wide consensus that proximal parts of the hair reliably reflect chronic cortisol concentrations.42 Exogenous environmental factors, such as frequent hair washing and cosmetic treatments could decrease cortisol levels in the more distal (older) segments of the hair.31 42–44 Additionally, sampling of hair that is taken from the posterior vertex is the most optimal, because the intraindividual variation is smallest at that site.31 34 Hair growth patterns vary across different regions of the scalp and the posterior vertex region shows the most uniform growth rates.45 Because hair grows approximately 1 cm per month, a hair sample of 1 cm is thought to reflect the mean exposure of cortisol in 1 month.30 ,46
The hair samples were taped to a piece of paper, and the proximal side was marked. The hair samples were stored at room temperature in an envelope until analysis.
Parents were also asked to fill out a questionnaire on, for example, frequency of washing the hair, hair colour, cosmetic hair treatments and medication/illness of their children.
Anthropometry
During the visit, blood pressure, growth and body composition were also measured (height, weight, hip and waist circumference and skin folds using Holtain calliper). All measurements, except for weight, were performed three times. Blood pressure was measured three times in rest with an automatic device (Omron M6 AC; Omron Healthcare, Hoofddorp, the Netherlands), using a cuff appropriate to the size of the child’s upper arm. The mean of the three measurements were used in the analysis. Fat percentage was calculated using the skin folds (biceps, triceps, subscapular and suprailiacal) with the Durnin and Womersley formula.47
BMI was calculated using the formula weight (kg)/height2(m2). Systolic and diastolic blood pressure/height ratios were calculated, since those ratios have been shown to correlate with the corresponding blood pressure percentiles in both male and female children.48 All other child-related values were transformed into SD scores (SDS) for age and gender according to the 2010 Dutch reference values,49 using the Growth Analyser(version 4.0; Growth analyser BV, Rotterdam, the Netherlands, http://www.growthanalyser.org). Birth weight was expressed as birth weight SDS, corrected for gestational age and gender.50
Data collection reference population
Hair samples and data on anthropometrics were collected during school visitation. Demographic information, data on general health, the use of medication and hair care were collected through questionnaires.41 Hair collection was performed with a similar method as in the current study.
Cortisol and cortisone analysis in hair
The hair samples were processed and analysed, by liquid chromatography–tandem mass spectrometry as described previously,44 at the department of Clinical Chemistry, Erasmus University Medical Center, Rotterdam, The Netherlands.
Statistical analysis
For all subjects, descriptive statistics were calculated as numbers, percentages, means, medians, SDSs and IQRs. For comparing baseline characteristics, Student’s t tests were used for normally distributed continuous variables, Wilcoxon rank-sum tests for not normally distributed continuous variables and χ² and Fisher’s exact tests for categorical variables. Cortisol and cortisone were logarithmically (log10) transformed to achieve a normal distribution. Linear regression models were built to analyse associations between cortisol and cortisone, and antenatal prednisone exposure. Factors associated in other studies24 51 with hair cortisol and cortisone concentrations (age, sex, socioeconomic status (SES) based on the educational level of the mother, season of hair collection, hair colour, washing frequency) were used as independent covariables. Similarly, a regression model was built to analyse the association between maternal DAS28-CRP(3) during pregnancy and cortisol and cortisone concentrations. Furthermore, associations between cortisol, cortisone, DAS28-CRP(3) and the anthropometric measurements (BMI SDS, fat percentage SDS based on skinfolds, waist and hip circumference SDS, systolic and diastolic blood pressure SDS, ratio waist-hip circumference and ratio skinfolds trunk to skinfolds peripheral) were analysed using linear regression.
In addition, a linear regression analysis was performed to compare the cortisol concentrations children born to mothers with RA, with the reference population using stepwise backwards selection of relevant covariates (age, sex, weight SDS, height SDS, BMI SDS, waist circumference SDS, height circumference SDS, SES, washing frequency and hair colour).
P≤0.05 were considered statistically significant. All statistical analysis were performed using STATA software V.15.1 for Windows.
Ethics
This study is in compliance with the Helsinki Declaration. The Medical Ethics Committee at the Erasmus MC University Medical Center Rotterdam, the Netherlands, approved the current study (MEC-2014–395) and the PARA-study (MEC-214.320/2002/117). Parents (and children) received oral and written information about the study. Informed consent was signed by both parents, and their children if they were aged ≥12 years.
Results
Participants
In total, 252 children born to mothers with RA and both of their parents were invited to participate in this study (figure 1). From these, 58 (23.0%) did not respond to the invitation and could not be reached by mail or phone. From the 72 invited subjects who refused participation, 35 (48.6%) did not provide a reason, 16 (22.2%) explained that they had participated in too many studies and 12 (16.7%) were not interested in participation due to the fact that this study had to be performed in their children. After exclusion of five children with antenatal prednisone exposure <5 mg/day and/or less than during two trimesters, in total 117 children were included in this study. From these, we included 56 children who had antenatally been exposed to prednisone (prednisone dose ≥5 mg/day, during at least 2 trimesters of pregnancy) and 61 children who had not been exposed.
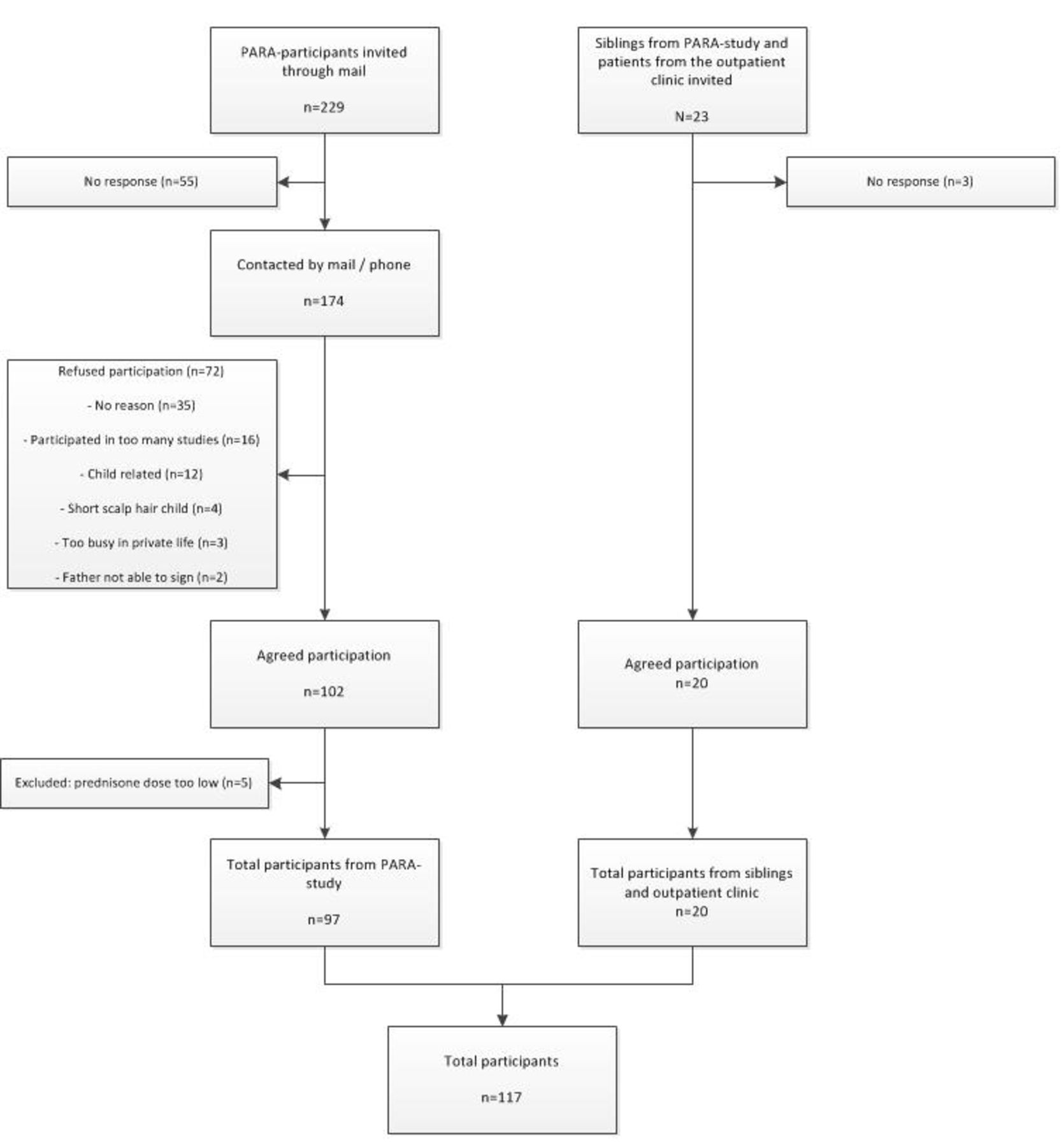
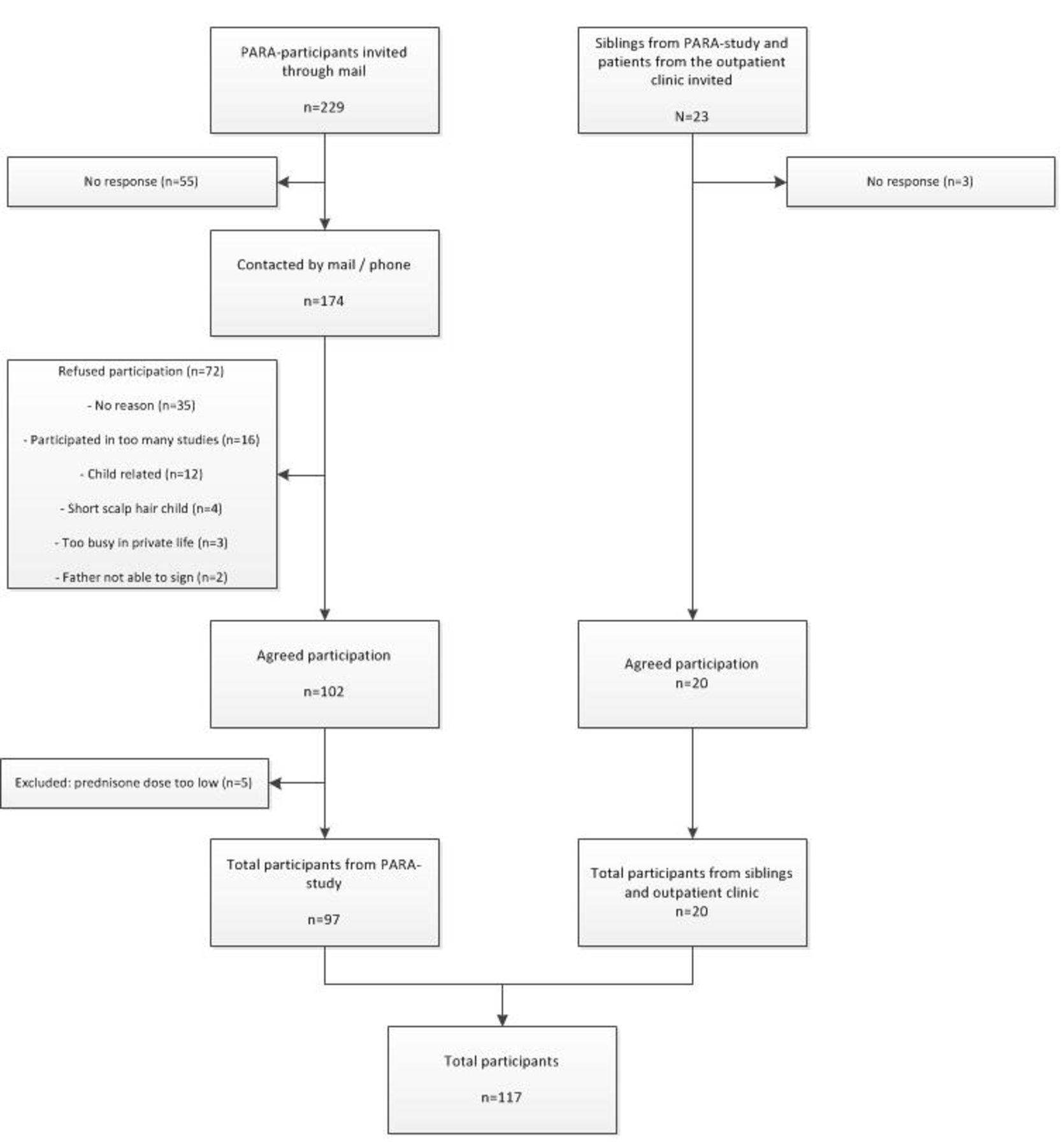{kind=link}
Flowchart of the study population and inclusion of study participants.
Participants and non-participants were compared. There were no statistically significant differences in maternal DAS28-CRP(3) in third trimester, maternal age at delivery, presence of autoantibodies in mother, SES based on educational level of the mother, sex of the offspring and birth weight. Gestational age was borderline significant (p=0.05), with a median gestational age of 277.9 days (IQR 270.9–286.0) in participants and 275.0 days (IQR 268.0–282.5) in non-participants.
Descriptive statistics of the study population are shown in table 1. Overall, the baseline characteristics were comparable in the prednisone and the non-prednisone group. Birth weight and gestational age were both significantly lower in the group with prednisone exposure compared with children without prednisone exposure. Mean birth weight was 3167.5 g (SD=691.9) in the prednisone group vs 3435.4 g (SD=584.2) in the non-prednisone group, p value 0.01. The median gestational age was 273.0 days (IQR 258.0–281) in the prednisone vs 281.0 days (IQR 274.0–287.0) in the non-prednisone group, p<0.001. Birth weight corrected for gestational age and sex was not different between the two groups. Maternal characteristics were also comparable in both groups, except for the DAS28-CRP(3), which was higher in the prednisone group, 3.7 (SD=1.1) vs 2.8 (SD=0.9) in the non-prednisone group, p<0.001. Detailed information on descriptive statistics of the children is provided in online supplementary table 1.
Supplemental material
Descriptive statistics of study population
Associations between antenatal prednisone exposure and cortisol and cortisone concentrations in scalp hair
The median hair cortisol concentration was 1.14 pg/mg (IQR 0.67–1.75) in the children with antenatal prednisone exposure and 1.15 pg/mg (IQR 0.65–2.21) in the children without antenatal prednisone exposure. The median hair cortisone concentration was 6.76 pg/mg (IQR 5.42–8.86) in the prednisone group and 7.40 pg/mg (IQR 5.39–10.73) in the non-prednisone group. After log-transformation, cortisol and cortisone were normally distributed. Hair cortisol and cortisone concentrations were not significantly different between the two groups.
In our study population, 17 children were exposed to prednisone with a mean dose per day ≥10.0 mg. Repeating the analyses in these children compared with the children without antenatal prednisone exposure did not result in significant associations between prednisone exposure and hair cortisol and cortisone concentrations (p>0.30). The median cortisol and cortisone concentrations were 0.97 pg/mg (IQR 0.68–1.57) and 6.26 (IQR 4.80–8.49) in the prednisone group (≥10.0 mg daily) and 1.15 (IQR 0.65–2.21) and 7.40 (IQR 5.39–10.73) in the non-prednisone group, respectively.
In univariable analysis, a higher SES (based on the educational level of the mother) was associated with higher hair cortisol and cortisone concentrations, and a washing frequency ≥3 times with lower cortisol concentrations. Children born to mothers with a higher SES had a lower washing frequency of their hair. The association between SES and levels of cortisol and cortisone was not present in the multivariable model.
In the multivariable linear regression models, prednisone exposure was not associated with hair cortisol and cortisone concentrations. The median of the mean prednisone dose per day during pregnancy was 7.5 mg/day (IQR 5.0–10.0). The mean prednisone dose and prednisone exposure in the first trimester were also not associated with these concentrations. In the multivariable models, only washing frequency was significantly associated with the levels of cortisone in hair. A washing frequency ≥3 times per week was associated with lower cortisone concentrations (p<0.05). Age, sex, season of hair collection and hair colour were not associated with hair cortisol and cortisone in the univariable and multivariable models.
Associations between antenatal prednisone exposure and anthropometric values
Antenatal prednisone exposure was not associated with the anthropometric measurements (BMI SDS, fat percentage SDS, waist circumference SDS, hip circumference SDS, ratio waist-hip, ratio systolic blood pressure/height, ratio diastolic blood pressure/height, and the ratio skinfolds trunk/peripheral), corrected for age, sex and SES (based on the educational level of the mother). The anthropometric values were also not associated with the hair cortisol and cortisone concentrations.
Associations with maternal RA disease activity
Maternal RA disease activity in the third trimester was not associated with hair cortisol and cortisone concentrations in the children. Maternal DAS28-CRP(3) in the third trimester was also not associated with the anthropometric measurements.
Comparison with reference population
The median hair cortisol concentration in the reference population was 1.93 pg/mg (IQR 1.18–3.11). After log-transformation, cortisol was normally distributed.
Hair cortisol concentrations were not different between children born to mothers with RA and the reference population, corrected for the relevant variables mentioned previously, in a multivariate linear regression model. In this model, an older age of the child and higher weight SDS were significantly associated with higher cortisol levels (p<0.05).
Discussion
Prednisone is an anti-inflammatory drug that is prescribed to patients with an autoimmune disease, for example, RA, also during pregnancy. Research into the long-term side effects of prednisone use during pregnancy on the offspring has been limited. In this relatively large and unique nationwide study, we followed the majority of the mothers and their children prospectively during and after pregnancy. The results of our study show that children with low-dose antenatal prednisone exposure do not have chronically elevated cortisol and cortisone concentrations in hair, compared with children without antenatal prednisone exposure. This is the first study to show these results prospectively from the antenatal period onwards in a (for this design) large cohort using scalp hair, reflecting chronic cortisol and cortisone concentrations. Adjustment for confounders allowed an independent analysis of the effects of antenatal prednisone exposure in childhood.
Prednisone exposure was also not associated with anthropometric measurements like BMI SDS, fat percentage SDS, waist circumference SDS, hip circumference SDS, ratio waist-hip and the ratio skinfolds trunk/peripheral or with ratio systolic blood pressure/height and ratio diastolic blood pressure/height. Furthermore, maternal RA disease activity during pregnancy was not associated with cortisol and cortisone concentrations and anthropometric measurements. Children born to mothers with RA had a similar cortisol concentration compared with the reference population.
In general, antenatal exposure to glucocorticoids might result in chronically elevated cortisol and cortisone concentrations in the offspring.1–4 46 Previous studies, mostly animal but also in humans, demonstrated long-term effects of maternal stress,8 maternal depression9 10 and maternal anxiety during pregnancy12–14 on cortisol concentrations or cortisol responses in offsprings. As mentioned before, adverse events during pregnancy have been shown to influence the development of the fetal HPA-axis. The systemic inflammation in patients with RA, and medication use during pregnancy are also considered as an adverse event during pregnancy. This is one of the few prospective studies in humans studying offspring antenatally exposed to synthetic glucocorticoids with the most reliable method to measure chronic cortisol and cortisone concentrations (in scalp hair).33 In our current study, we did not find any association between antenatal exposure to low-dose prednisone, maternal RA disease activity during pregnancy and long-term cortisol and cortisone concentrations or with an altered body composition or higher blood pressure in childhood.
In a previous study by de Steenwinkel et al,26 children born to mothers with RA with antenatal prednisone exposure had higher daytime cortisol levels (measured in saliva) compared with children without prednisone exposure. However, measuring cortisol in saliva is not a reliable method for long-term concentrations due to the circadian rhythm, pulsatile secretion, daily variation and reactivity to acute (transient) stress.21 29 30 Measuring cortisol in hair reliably reflects chronic concentrations. The elevated salivary cortisol levels in children with antenatal prednisone exposure born to mothers with RA from the study by de Steenwinkel et al 26 could be a result of increased HPA-axis reactivity. However, for studying HPA-axis reactivity, cortisol concentrations should preferably be measured before and after administrating a stressor. In another study by de Steenwinkel et al,52 maternal RA disease activity during pregnancy and antenatal prednisone exposure had no influence on the body composition or on the risk for the metabolic syndrome of approximately 7-years-old offspring.52 In concordance with this study, we did not find either any associations between maternal RA disease activity during pregnancy, antenatal prednisone exposure and body composition in offspring aged approximately 10 years, which is reassuring. It is still possible that the consequences for these offsprings will emerge later in their life, therefore following these children until postpubertal age is interesting for future research. The chronic use of prednisone and high RA disease activity are associated with reduced bone mineral density (BMD).53 54 In our study, we did not explore the effect of antenatal prednisone exposure on the BMD of the offspring. However, in a previous study by de Steenwinkel et al,55 they investigated the influence of medication use and disease activity of the mother during pregnancy on the offspring at the age of approximately 7 years. In that study, a dual x-ray absorptiometry scan was performed in 108 children born to women with RA. They did not find any association between BMD and prednisone use or RA disease activity during pregnancy, even after correcting for all known associated variables, which is reassuring.
Currently, the treatment options for RA during pregnancy are prednisone, sulfasalazine, hydroxychloroquine and TNF-inhibitors.56 Most patients start with sulfasalazine or hydroxychloroquine, and when they do not respond to this therapy, prednisone or TNF-inhibitors are added. Compared with prednisone, TNF-inhibitors are expensive and worldwide not easily available for all patients with RA. Therefore, it is important that this study showed the long-term safety of maternal prednisone use during pregnancy.
Certain limitations should be taken into account when interpreting the results of this study. First, from the 252 invited children (and their parents), 122 (48.4%) were willing to participate in this study. In total, 72 (28.6%) refused participation. Baseline characteristics were comparable between participants and non-participants. These findings decrease the likelihood that selection bias influenced the results of this study.
Second, in this study, the median of the mean prednisone dose per day during pregnancy was 7.5 mg (IQR 5.0–10.0). The use of prednisone concentrations above 7.5 mg/day or even 10 mg/day might be more likely to influence the long-term cortisol and cortisone concentrations in the offspring. However, repeating the analyses in the children who were antenatally exposed to higher prednisone dosages (mean dose per day ≥10.0 mg), did not lead to different results. In addition, lower concentrations of prednisone are often sufficient for the treatment of RA during pregnancy. Unfortunately, we did not have information on maternal weight during pregnancy for the majority of the participants. Maternal weight during the visit when the children’s hair was collected (child age approximately 10 years) was measured. However, since that would not be completely representative of the weight during pregnancy, prednisone dosages could not be corrected for maternal weight.
In conclusion, our study demonstrates that low-dose antenatal prednisone exposure and maternal RA disease activity during pregnancy are not associated with long-term elevated cortisol and cortisone concentrations, an altered body composition or higher blood pressure in prepubertal childhood. Prednisone is an effective, low-priced antirheumatic drug that is considered safe to use during pregnancy. The findings of this study support the assumption that maternal prednisone use during pregnancy is safe for the offspring, at least until the age of approximately 10 years, which is reassuring for mothers who use prednisone and their physicians.
Acknowledgments
We are grateful to all patients participating in this study. We thank all research assistants and laboratory workers for their help with data collection and processing.
References
Footnotes
Contributors JMWH, RJEMD, ELTvdA, YBdR, EFCvR and HI-A: study design and analysis plan; JMWH and RJEMD: data acquisition; HI-A: cleaning of data; HI-A and RJEMD: analysis; HI-A and RJEMD: draft paper; JMWH, RJEMD, ELTvdA, YBdR, EFCvR and HI-A: revision of paper and final approval for publication.
Funding This study was funded by the Dutch Arthritis Society (ReumaNederland, previously known as Reumafonds), a non-commercial fund raising organisation.
Competing interests RJEMD received an unrestricted grant from UCB Pharma B.V.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data may be obtained from a third party and are not publicly available. Department of Rheumatology, Erasmus MC.