Article Text

Abstract
Objectives Autoimmune rheumatic diseases (ARDs) affect women of childbearing age and have been associated with adverse birth outcomes. The impact of diseases like ankylosing spondylitis and psoriatic arthritis (PsA) on birth outcomes remains less studied to date. Our objective was to evaluate the impact of ARDs on preterm birth (PTB), congenital anomalies, low birth weight (LBW) and small for gestational age (SGA), in a large cohort of women.
Methods We conducted a propensity score-matched analysis to predict ARD from a retrospective birth cohort of all live, singleton births in California occurring between 2007 and 2012. Data were derived from birth certificate records linked to hospital discharge International Classification of Diseases, ninth revision codes.
Results We matched 10 244 women with a recorded ARD diagnosis (rheumatoid arthritis (RA), systemic lupus erythematosus (SLE), antiphospholipid syndrome, PsA); ankylosing spondylitis and juvenile idiopathic arthritis (JIA) to those without an ARD diagnosis. The adjusted OR (aOR) of PTB was increased for women with any ARD (aOR 1.93, 95% CI 1.78 to 2.10) and remained significant for those with RA, SLE, PsA and JIA. The odds of LBW and SGA were also significantly increased among women with an ARD diagnosis. ARDs were not associated with increased odds of congenital anomalies.
Conclusion Consistent with prior literature, we found that women with ARDs are more likely to have PTB or deliver an SGA infant. Some reassurance is provided that an increase in congenital anomalies was not found even in this large cohort.
- autoimmune rheumatic diseases
- preterm birth
- small for gestational age
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
It has been shown that, in general, autoimmune rheumatic diseases (ARDs) are associated with worse pregnancy outcomes.
What does this study add?
Less common ARDs like psoriatic arthritis were also shown to have this association in our study.
Given these results, women with ARDs should be counselled that there is an increased risk of adverse birth outcomes.
Some reassurance is provided that an increase in congenital anomalies was not found even in this large cohort.
How might this impact on clinical practice?
Future large studies using cohorts that could access linked mother–child records and assess the relative contributions of maternal disease severity and treatments used towards these adverse outcomes are needed.
Introduction
Autoimmune rheumatic diseases (ARDs) are painful, debilitating conditions characterised by abnormal immunological targeting of healthy muscle, joint, bone or organ tissue causing chronic inflammation and cell damage.1 2 There usually is a delay in diagnosing these diseases, especially in women.3 4 Women are disproportionally affected by ARDs, with disease onset often occurring during childbearing years.5 Female sex hormones, particularly oestrogens, have been shown to play an important role in disease development and progression.6 Pregnancy is uniquely challenged in women with ARDs as disease-modifying drug regimens, disease flares and the presence of autoantibodies may adversely affect maternal and neonatal outcomes.2 6
Previous studies indicate that women with ARDs are more likely to experience fetal loss, intrauterine growth restriction (IUGR), low birth weight (LBW) and preterm birth (PTB).7 8 As most of these studies were performed using small sample populations,9 they were only powered to assess the impact of more common ARDs, such as rheumatoid arthritis (RA) and systemic lupus erythematosus (SLE), on birth outcomes. Fewer studies have assessed birth outcomes of women with less common ARDs such as ankylosing spondylitis (AS), which has been reported to be much less frequent in females than males, and psoriatic arthritis (PsA).10 11
The objective of this study was to evaluate the impact of ARDs on PTB, congenital anomalies, LBW and small for gestational age (SGA), in a large, racially diverse and ethnically diverse cohort of women. Identification of women at highest risk of adverse birth outcomes will help facilitate coordinated medical and obstetric care for improvement of pregnancy outcomes.
Materials and methods
Study population and data collection
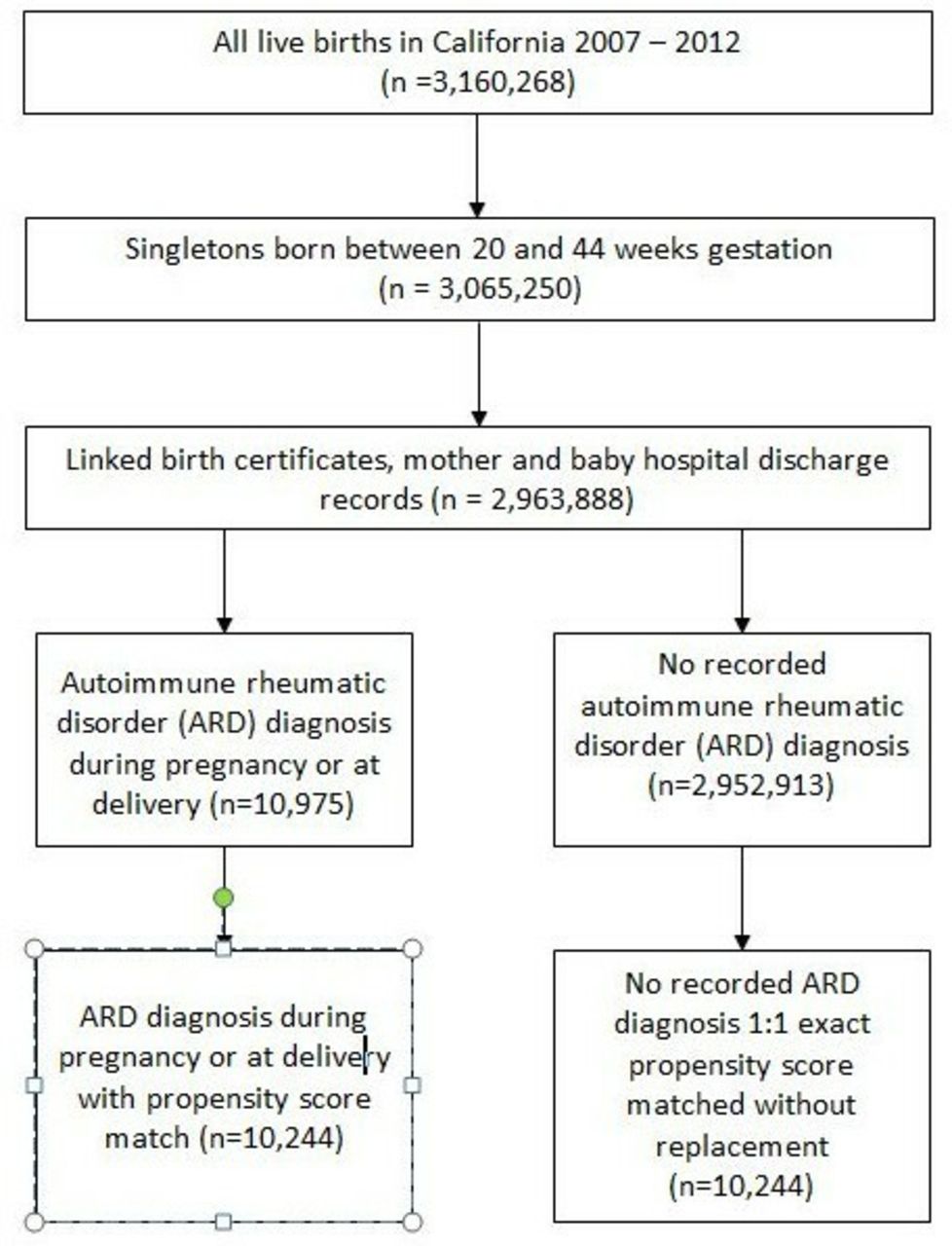
In this retrospective cohort study, the sample was drawn from all California live (20–44 weeks gestation), singleton births between 1 January 2007 and 31 December 2012 (n=3 160 268). The sample population was restricted to only include those with linked mother and child birth records and hospital discharge summaries maintained by the California Office of Statewide Health Planning and Development (n=2 963 888). The database contains linked infant birth and death certificates and information about maternal and infant characteristics, diagnoses and procedures from up to 1 year prior to delivery and 1 year after delivery.
The data files contained International Classification of Diseases, ninth revision, Clinical Modification (ICD-9-CM) diagnoses codes.12 We identified women with ARDs, diagnosed prior to pregnancy and up to 1 year after delivery, using the following ICD-9-CM codes: RA (714.0, ‘rheumatoid arthritis’), SLE (710.0, ‘systemic lupus erythematosus’), PsA (696.0, ‘psoriatic arthropathy’), antiphospholipid syndrome (APS) (289.81, 646.80), juvenile idiopathic arthritis (JIA) (714.3, ‘juvenile chronic polyarthritis’) and AS (720.0, ‘ankylosing spondylitis’). Information on a number of potential confounders was collected from birth certificate records. These included race and ethnicity, maternal age at delivery, pre-pregnancy body mass index (BMI) (calculated as pre-pregnancy weight (kg)/(height (m))2), expected payer for delivery, maternal education, smoking during pregnancy, previous PTB, maternal diabetes and year of birth. Additional variables identified from hospital discharge ICD-9-CM codes included: drug or alcohol dependence (648.3, ‘drug dependence; 303, ‘alcohol dependence syndrome; 304, ‘drug dependence’; and 305, ‘non-dependent abuse of drugs’), thyroid disorder (246.0, ‘disorders of thyrocalcitonin secretion’; 246.9, ‘unspecified disorder of thyroid’ and 648.1, ‘thyroid dysfunction complicating pregnancy childbirth or the puerperium’), asthma (493, ‘asthma’) and hypertensive disorder (642, ‘hypertension complicating pregnancy, childbirth and the puerperium’).
Birth outcomes assessed included PTB, congenital anomalies, LBW and SGA. Gestational age was determined using best obstetric estimate and was obtained from birth certificate records. Gestational age at delivery <37 weeks was considered preterm.13 PTB was categorised as any, spontaneous, or medically indicated. Spontaneous PTB was further subdivided into either prelabour rupture of membranes (PROM) or labour with intact membranes (ie, no PROM). The preterm PROM group included all pregnancies with indication of preterm PROM on the infant’s birth certificate or maternal hospital discharge record.14 15 Women with birth certificate or hospital discharge indication of premature labour or tocolytic medication use, without recorded preterm PROM, were included in the spontaneous labour with intact membranes group. Medically indicated PTB was defined as induction or caesarean delivery <37 weeks gestation without PROM, premature labour or tocolytic administration.15
Both major structural birth defects and chromosomal abnormalities were included in the congenital anomalies outcome. Structural birth defects were considered to be ‘major’ if they were determined, on clinical review, to cause major morbidity or mortality and were likely to be identified in the hospital at birth or lead to hospitalisation during the first year of life.16 Chromosomal abnormalities were identified by the ICD-9-CM code 758 for ‘chromosomal anomalies’ (online supplementary table 1).
Supplemental material
Birth weight was obtained from birth certificate records. LBW was defined as weighing <2500 g at birth.17 SGA was defined as having a birth weight in the lowest 10th percentile for gestational age.18
Statistical analysis
To adjust for differences in baseline characteristics between women with an ARD diagnosis and those without, a propensity score matching analysis was performed. This analytical method is frequently used to approximate the experimental situation of randomisation in observational studies.19 Logistic regression was used to create a propensity score for each individual to predict ARD diagnosis. All maternal characteristics identified as potential confounders, with the exception of pre-pregnancy BMI, were included in the propensity score model. Pre-pregnancy BMI was removed from the model due to the large number of women with missing data (6.7%). While many women were also missing information on level of education (3.7%), level of education among women with and without an ARD diagnosis differed significantly on removal of this variable from the model, necessitating its inclusion in the model. Propensity scores for women with an ARD were exact matched, without replacement, in a 1:1 ratio to the propensity scores for women without an ARD.
Maternal demographic and clinical characteristics were compared between women with a recorded ARD diagnosis and women without a recorded ARD diagnosis, both before and after propensity score matching, using χ2 testing. Logistic regression was used to estimate the odds of PTB, congenital anomalies, LBW and SGA among women with a recorded ARD compared with women without an ARD. P values were adjusted for using the Bonferroni correction. Statistical analyses were conducted using SAS V.9.4 software.
Results
In our study population, a total of 10 975 women had an ARD diagnosis during pregnancy or 1 year after delivery (figure 1). Of these women, 10 244 (93.3%) were exact propensity score matched to women without a recorded ARD diagnosis. The majority of recorded ARD diagnoses among women with a propensity score match included APS (35%, n=3908), SLE (33%, n=3595) and RA (26%, n=2921). A smaller proportion of women were diagnosed with JIA (3%, n=337), PsA (2%, n=161) and AS (1%, n=128).

Sample selection.
Before propensity score matching, women with an ARD diagnosis were demographically and clinically different than women without an ARD diagnosis (table 1). Women with an ARD diagnosis were more likely to be white, not Hispanic, >34 years of age at delivery, have a pre-pregnancy BMI ≥30.0 kg/m2, delivery through caesarean section, be privately insured and have >12 years of education than women without an ARD diagnosis. Additionally, a greater proportion of women with an ARD diagnosis smoked or used drugs/alcohol during pregnancy, had a previous PTB and were diagnosed with a thyroid or hypertensive disorder, asthma or diabetes than women without an ARD diagnosis. After propensity score matching, all variables were balanced among the cases and controls (p>0.05), including BMI which was not included in the propensity score.
Maternal characteristics among women with and without an ARD diagnosis in the whole population and the propensity-matched sample.
Majority of ARDs associated with an increased risk of adverse pregnancy outcomes
Women with an ARD diagnosis had nearly a twofold increase in odds of having a PTB compared with women without an ARD diagnosis (OR 1.93, 95% CI 1.78 to 2.10) (table 2). This finding was consistent across all subtypes of PTB: spontaneous labour, PROM (OR 1.94, 95% CI 1.62 to 2.31); spontaneous labour, no PROM (OR 1.83, 95% CI 1.63 to 2.04) and medically indicated (OR 1.85, 95% CI 1.56 to 2.21). The odds of LBW and SGA were also significantly increased among women with an ARD diagnosis compared with women without an ARD diagnosis (OR 1.70, 95% CI 1.43 to 2.02; OR 1.49, 95% CI 1.36 to 1.63, respectively). Women with an ARD diagnosis were not found to be at increased odds of congenital anomalies compared with women without an ARD diagnosis.
Odds of adverse birth outcomes among women with an ARD compared with women without a recorded ARD
When assessing each ARD individually, the odds of PTB were the highest among women with SLE (OR 2.84, 95% CI 2.57 to 3.15) (figure 2 and table 2). While the odds were significantly increased for all PTB subtypes among women with SLE, after Bonferroni correction, the odds of medically indicated PTB were the highest, with women with SLE experiencing a nearly threefold increase in odds compared with women without an ARD diagnosis (OR 2.82, 95% CI 2.30 to 3.45). Women with RA, APS and more than one ARD diagnosis were also at increased odds of delivering preterm compared with women without an ARD diagnosis (OR 1.55, 95% CI 1.37 to 1.75; OR 1.65, 95% CI 1.48 to 1.85; OR 1.82, 95% CI 1.52 to 2.17). The odds of LBW and SGA also varied by the type of ARD diagnosis. Similar to what was observed for PTB, women with SLE were at the highest odds of LBW and SGA (OR 2.35, 95% CI 1.91 to 2.89; OR 2.08, 95% CI 1.86 to 2.32, respectively) (table 2). The odds of LBW and SGA were also significantly increased, after Bonferroni correction, for women with RA (OR 1.57, 95% CI 1.22 to 2.01; OR 1.42, 95% CI 1.25 to 1.62). Women with more than one ARD were at increased odds of SGA, but not LBW.

{kind=link}
{kind=link}
Odds of PTB (<37 weeks’ gestation) by type of ARD diagnosis. ARD, autoimmune rheumatic disease; APS, antiphospholipid syndrome; AS, ankylosing spondylitis; JIA, juvenile idiopathic arthritis; PA, psoriatic arthritis; PTB, preterm birth; RA, rheumatoid arthritis; SLE, systemic lupus erythematosus.
Less common ARDs are also associated with adverse pregnancy outcomes
Less common ARDs (ie, PsA, JIA and AS) were also associated with an increased odds of PTB (figure 2 and table 2). Among women with PsA and JIA, the odds of PTB was higher compared with women without any ARD (OR 1.77, 95% CI 1.15 to 2.73; OR 1.60, 95% CI 1.17 to 2.19). The odds of PTB did not differ between women with AS and women without an ARD (OR 1.09, 95% CI 0.61 to 1.94). The odds of SGA were increased among women with AS (OR 2.06, 95% CI 1.28 to 3.30); however, this association did not meet statistical significance after adjusting for multiple comparisons. Diagnosis of PsA, JIA or AS was not associated with an increase in odds of congenital anomalies or LBW.
Discussion
Using a large, racially and ethnically diverse sample of pregnant women with linked birth records, our study showed that women with documented diagnoses of ARDs, including RA, SLE, PsA, APS, JIA and AS, have significantly higher odds of adverse birth outcomes such as PTB, LBW and SGA compared with women without one of these ARDs. However, ARDs were not associated with an increase in odds of congenital anomalies.
Previous work has shown that 0.09% of obstetric hospitalisations have a discharge diagnosis of SLE, which is comparable to the 0.12% of women that had a diagnosis of SLE in our study population.8 20 Most research to date on PTB in women with ARDs has focused on SLE. This is likely due to the larger number of women in the childbearing age group with this disease. We found that SLE was significantly associated with adverse pregnancy outcomes. Previously, a large meta-analysis showed worse pregnancy outcomes among women with SLE compared with those without SLE.21 Multiple studies have shown an increased prevalence of PTB of about 21%,7 22 which is similar to our finding of 22.8%. To our knowledge, this is the largest study to assess the risk of congenital anomalies among women with SLE.
Our study of women with RA is one of the largest in the literature. We found similar odds of PTB to other studies that had noted a 15%–17% prevalence of PTB in women with RA,23 24 which is comparable to our finding of 13.8%. LBW and SGA were also increased in women with RA in our study. In the National Inpatient Sample among women with JIA, there was an aOR of 2.1 for PTB and no difference in SGA.25 In our study, JIA was associated with PTB but not SGA or LBW.
There have been no large studies performed in the USA on birth outcomes of mothers with PsA. In a racially homogenous Scandinavian population, Broms et al studied 964 births among women with PsA and showed an increase in adverse pregnancy outcomes.10 Another study followed 29 women with 42 pregnancies and was only able to comment that 95% of births were live births.26
There are very few studies focusing on large groups of women with AS and their pregnancy outcomes, which may be due in part to its under-recognition and delayed diagnosis among women. Jakobsson et al had analysed 388 pregnancies in 301 Swedish women with AS and found an increased frequency of caesarean delivery; PTB was increased in women with AS relative to the general population (9% vs 4.9%).11 The OR for SGA in their study was 2.12 (95% CI 1.00 to 4.50), similar to an aOR of 2.06 (95% CI 1.28 to 3.30) in our cohort, emphasising that these pregnancies also need increased surveillance.
There have been a number of studies on APS in pregnancy likely due to its association with miscarriage. Other studies have shown a prevalence of PTB ranging from 19% to 48% and an increased frequency of SGA/IUGR at 5%–31%.27 28 These findings are similar to our study with 14.6% of women with APS having PTB and an increased frequency of LBW at 2.8%. There was no increased risk of congenital anomalies evaluated in these prior studies.
Worse outcomes among women with ARDs likely have a multifactorial aetiology. Many explanations have been postulated in the past. Poorly controlled ARDs and increased prednisone use have been shown to increase the risk of delivering a low birthweight infant.29 It has also been suggested that tumour necrosis factor alpha, interleukin-1 beta and interleukin-6 can decrease the level of the enzyme that deactivates maternal cortisol and may lead to lower birth weights in a similar mechanism. All of these cytokines have also been associated with poorly controlled RA in the past.30 Adams and Nelson proposed that microchimerism may be an underlying cause of differences in outcomes even within women with a specific ARD and between pregnancies for one woman given the way specific maternal immune systems interact with fetal cells in circulation.31
Our study has several major strengths, most notably a large racially and ethnically diverse cohort which allowed us to analyse less common ARDs. Given that it is a population-based study, it is more likely to include the entire population of women with ARDs. Some prior work has excluded women with severe disease and other work may not include women with mild disease as they are not followed as frequently in clinical practice. Other studies, especially internationally, may have larger populations of white women, whereas our study included a larger number of women of other races and ethnicities that may have a predisposition to worse birth outcomes and more severe ARD manifestations. Our study was also strengthened by our use of propensity score matching, which aided in reducing bias and confounding introduced by non-randomisation of the cohort and allowed for a more accurate comparison of outcomes between the exposure groups.32 Due to our large sample size, we were able to match almost all women with an ARD to those without an ARD.
Our study has a few limitations. Given the use of a database, there are some inherent limitations such as the lack of information about activity and severity of rheumatic disease and medication use. Medications usage was not available for this cohort, and so we were unable to assess the effect of disease-modifying antirheumatic agents on adverse pregnancy outcomes. Future studies are needed to examine the risk of PTB among women being treated with disease-modifying antirheumatic drugs like methotrexate or tumour necrosis factor inhibitors compared with women who are not treated to better understand what is driving the increased risk of PTB observed in this study. Discharge records are limited in capture of behavioural and illicit exposures; smoking and alcohol use are usually under-reported and some comorbidities, if not severe, do not get coded. We used ICD codes for identification of ARDs, and hence, disease misclassification is possible. Prior work has shown that SLE diagnoses by ICD-9 codes from health plans in pregnancy have good validity, including a positive predictive value of 93% for SLE from birth records to correlating chart review.11 The timing of diagnosis of ARDs in this study included prior to pregnancy and up to 12 months after delivery. Although it is possible that the ARD was diagnosed a year after birth, based on the progression of this disease, it is likely the ARD was present during pregnancy. We conducted a sensitivity analysis of women with ARD diagnosis limited to only prior to delivery and found women with ARDs had 2.18 times the odds of giving birth preterm than women who did not have ARD prior to delivery, giving robustness to our results. Since there is usually a delay in diagnosis of these diseases, we feel it was imperative to include women diagnosed a year after delivery in our study cohort.
Conclusions
Our study confirmed the previously reported association between ARDs and adverse pregnancy outcomes. Women with SLE were found to have the highest risk of adverse outcomes. We were also able to show an association with less common ARDs and worse pregnancy outcomes in a large racially and ethnically diverse population. While outcomes such as PTB were increased among women with ARDs, congenital anomalies were not statistically increased. Given these results, women with ARDs should be counselled that there is an increased risk of adverse birth outcomes but not of congenital anomalies. Further studies using cohorts that could access linked mother–child records and assess the relative contributions of maternal disease severity and treatments used towards these adverse outcomes are needed.
Acknowledgments
Authors would like to thank the Preterm Birth initiative for generously providing data for this study. This work was previously presented as a poster at the 2018 EULAR conference in Amsterdam, Netherlands: JS, BMD, MF, RF-R, LJ-P, RJB, CF, GB, RP, NP, KKR and NS. 'The impact of autoimmune rheumatic diseases on birth outcomes in an ethnically diverse cohort of women in the United States. Ann Rheum Dis, 77(Suppl), 2018, A531'.
References
Footnotes
Contributors All the authors contributed substantially to the conception and design of the work; the acquisition, analysis and interpretation of data; drafting the work and revising it critically for important intellectual content and final approval of the version published.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Methods and protocols for the study were approved by the Committee for the Protection of Human Subjects within the Health and Human Services Agency of the State of California.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement The data used in this analysis is owned by the State of California who grants access through an application and approval process. This process is open to any interested researcher or other investigator who seeks access. No special permission was granted for this project. Interested researchers may apply for access to the data at: https://www.cdph.ca.gov/Programs/CFH/DGDS/Pages/cbp/default.aspx.