Article Text

Abstract
Objective To summarise the evidence on intra-articular therapies (IAT) to inform the 2020 EULAR recommendations.
Methods An overview of systematic reviews (SR) including randomised-controlled trials (RCTs) of IAT in adults with arthropathies was performed up to July 2020. Pain, function, and frequency of adverse events were the main efficacy and safety outcomes, respectively. Quality was assessed with the A MeaSurement Tool to Assess Systematic Reviews (AMSTAR)-2 tool.
Results Of 184 references identified, 16 met the inclusion criteria, and a search of their reference lists identified 16 additional SRs. After quality assessment, 29 were finally included. Of these, 18 focused on knee osteoarthritis (KOA), 6 on hip osteoarthritis (HOA), 3 on shoulder capsulitis (SC), and 3 on rheumatoid arthritis. Overall, hyaluronic acid showed a small effect on pain and function in KOA but not in HOA or shoulder capsulitis. Intra-articular glucocorticoids showed a small effect in pain and function in KOA and function in HOA and SC. Platelet-rich plasma showed benefit in pain and function in KOA but not in HOA. Mesenchymal stem cells behaved similarly. Most SR results were of moderate quality and RCTs included often presented a high risk of bias, mainly due to inadequate blinding and heterogeneous results. All interventions were well tolerated with no clear safety differences.
Conclusions This overview underlines that most IAT currently used in KOA, HOA, and SC exert small effects and are well tolerated. However, no firm conclusions can be drawn for inflammatory arthritis due to the limited data found.
- arthritis
- glucocorticoids
- osteoarthritis
- therapeutics
Data availability statement
Data are available upon reasonable request to the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Intra-articular therapies are frequently used in clinical practice by a wide range of health professionals from different specialties.Several compounds are currently available for intra-articular administration, from glucocorticoids to the more recent platelet-rich plasma or mesenchymal stem cells. Nonetheless, data on their efficacy in certain diseases are inconsistent and a matter of debate.
What does this study add?
This overview of systematic reviews provides a summary of the current evidence on the efficacy and safety of most compounds commonly used for intra-articular injections.
How might this impact on clinical practice or future developments?
This overview of systematic reviews informed the task force for the 2021 EULAR recommendations for intra-articular therapies and constitutes an evidence base for future updates
Introduction
Intra-articular therapies (IAT) have been widely used in clinical practice for years to reduce joint pain and improve function.1 They are used in many joint disorders including osteoarthritis (OA) and rheumatoid arthritis (RA) and delivered by a range of health professionals including clinicians from a range of specialities and also allied healthcare professionals.2 3 However, evidence on the efficacy and safety of available therapies is not always consistent, due in part to methodological limitations in published trials.4 5
Currently, many compounds are available as IAT from glucocorticoids (GC)—methylprednisolone acetate (MPA), triamcinolone acetonide (TA), and triamcinolone hexacetonide (TH)—radioisotopes—yttrium-90, rhenium-186, etc—or hyaluronic acid (HA) to more recent therapies such as platelet-rich plasma (PRP) and mesenchymal stem cells (MSC), mostly used for treating OA.6–10 The arrival of the latter three products on the market was accompanied by a vast amount of literature with contradictory results that are still under debate. Furthermore, intra-articular procedures elicit an important placebo effect, something that adds more complexity to its efficacy assessment.5 11–13
As around the world life expectancy, obesity, and sedentary lifestyle increase,14–16 the burden of disease imposed by chronic arthropathies and their comorbidities also increases, thus providing the right scenario for local treatments such as IAT, while the search for disease-modifying osteoarthritic drugs continues.
Based on all this, a task force was assembled by the EULAR to produce recommendations for IAT in arthropathies. The objective of the present work was to inform the task force about the current state of the evidence.
Methods
Study design
We performed an overview of systematic reviews (SR) following a prespecified protocol. The present study is reported following the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) statement.17
Eligibility criteria
To be eligible, the SR had to include randomised clinical trials (RCT) assessing IAT in adults (≥18 years old) with any arthropathy, excluding the spine and temporomandibular joints.
Interventions (IAT) could be any of the following: GC, HA, PRP, MSC, radiopharmaceuticals, anaesthetics, opioids or biologicals. Comparators could be any of the above mentioned, any form of intra-articular placebo or drugs administered orally as the standard of care (SoC), such as paracetamol/acetaminophen, non-steroidal anti-inflammatory drugs, pregabalin, tricyclic antidepressants. Studies evaluating botulinum toxin as intervention were excluded since its use was deemed to be irrelevant to the current clinical practice of the specialities represented within the task force. Surgical procedures were also excluded as comparators since they do not represent the SoC in most diseases covered in the current study. SRs assessing multiple comparators, including ozone or botulinum toxin, were included as long as they presented separate comparisons for the interventions mentioned in the inclusion criteria.
All efficacy and safety outcomes were considered, especially change in pain and function with any available measure, such as the Visual Analogue Scale (VAS), Lequesne index18 or the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC),19 and adverse events (AE), including serious adverse events (SAE), such as local reactions or swelling for the former and infections in the injected joint for the latter.
Search strategy
A search was performed in MEDLINE with the assistance of an expert librarian, from inception to January 2019 and updated in July 2020. The references of the included SRs were reviewed, as well as publications provided by the members of the task force. Details on the complete search strategy are provided in the online supplemental material.
Supplemental material
Study selection and data collection
Two investigators (SCR-G and RC-M) independently screened the titles and abstracts to ascertain eligibility. The full texts of the eligible articles were then appraised using the same approach, with discrepancies solved through consensus, including a third investigator (LC) if needed. Data regarding study and population characteristics, inclusion/exclusion criteria, interventions, outcome definition, outcome measures, and follow-up was extracted using a standardised form.
Methodological quality assessment
The same two investigators performed an independent quality assessment of the eligible SRs using the ‘A MeaSurement Tool to Assess Systematic Reviews (AMSTAR)−2’ tool.20 Briefly, this instrument rates the overall confidence in the results of a given SR by thoroughly analysing seven critical domains. The quality was used as a criterion for inclusion. Only SRs of high or moderate quality were included unless a low quality focused on a disease or intervention not covered by the already included SRs.
Data analysis
The qualitative synthesis was carried out by disease and compound. For binary variables, we extracted the ORs or risk ratios (RR) with their 95% CI. For continuous outcomes, data were retrieved as mean difference (MD) with 95% CI. When different measurements were used for the same outcome, treatment effects were retrieved as standardised mean difference (SMD) with CI. To interpret the magnitude of the effects, we used the criteria proposed by Cohen.21
Results
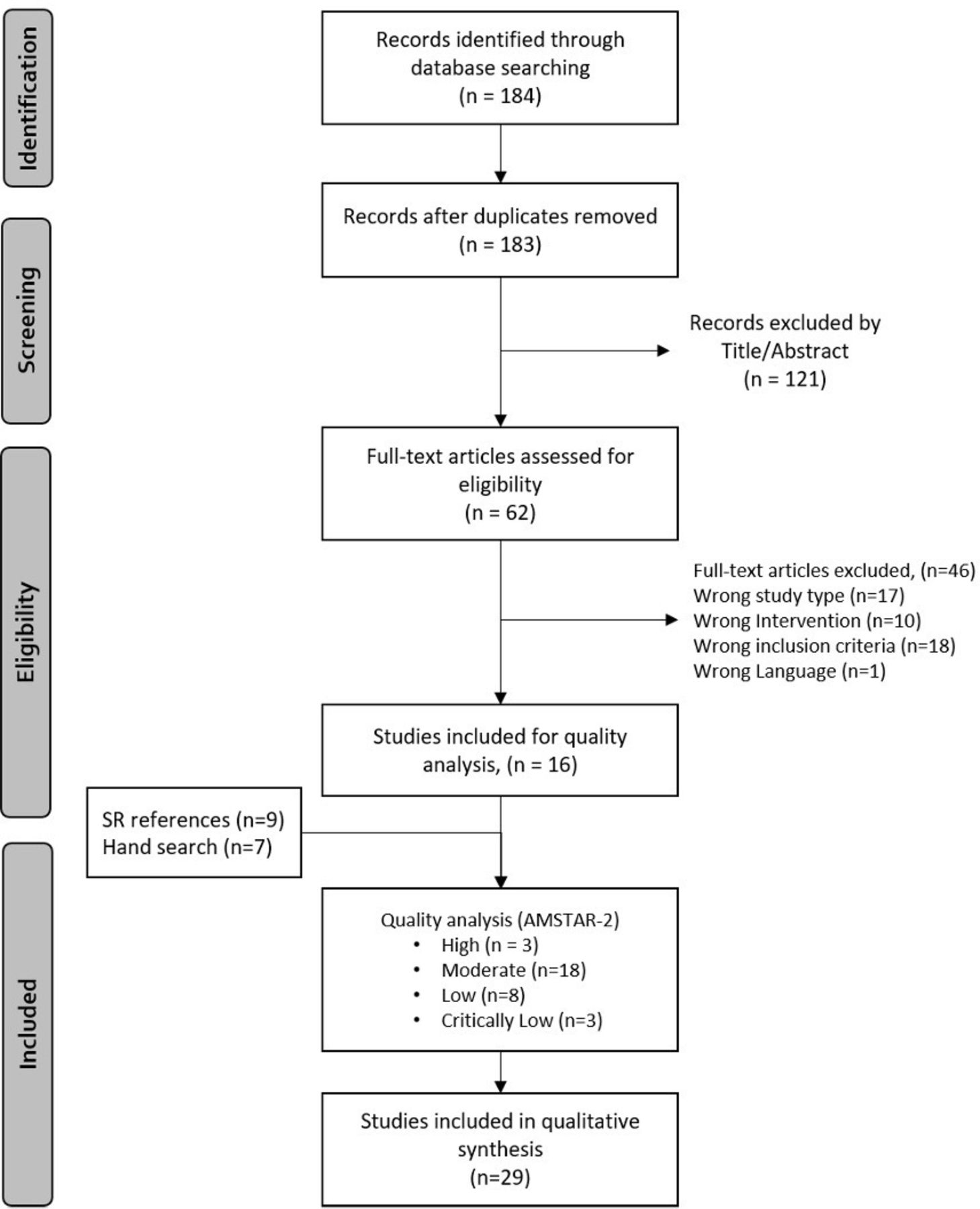
From a total of 183 references, after removing duplicates, 62 were selected for full-text review and 16 met inclusion criteria. Additionally, 16 SRs were identified through the reference lists of included studies and after an update to July 2020. Hence, 32 SRs underwent quality assessment. Three SRs were rated as of ‘high confidence’, 18 as ‘moderate’, 8 as ‘low’, and 3 as ‘critically low confidence’. Following the prespecified protocol, the latter were excluded. Those rated as of low confidence were finally included due to the low amount of data on the studied compounds. Therefore, 29 SRs were included in the qualitative synthesis. A flowchart is shown in figure 1 and a list of excluded articles with reasons for exclusion is provided in the online supplemental material.
{kind=link}
Flow chart of the overview of systematic reviews (SR).
The main features of the SRs included are summarised in table 1. Knee osteoarthritis (KOA) was analysed in 18 SRs,4–7 22–35 hip OA in 6,36–42 shoulder adhesive capsulitis in 3,43–45 and RA in 3.34 46 47 One SR analysed the efficacy of IAT in both KOA and RA.34 Different HA-containing compounds were assessed in 13 SR,4–7 22 30 31 33 35 37 40 44 47 PRP in 8,25–27 29 32 36 39 41 42 GC in 6,23 28 34 38 43 45 and MSC and yttrium synovectomy in 1 each.24 46
Main characteristics of the SR included
Efficacy of intra-articular treatments
Knee osteoarthritis
The main efficacy results are shown in table 2. The most frequent outcomes were pain, function, OMERACT-OARSI responder index, and quality of life (QoL). An SR included the change in joint space width and cartilage volume.31
Main efficacy results of IAT for knee osteoarthritis
HA compounds were extensively analysed in comparison mostly against IA placebo followed by IA GC. Compared with the former and according to Cohen’s criteria,21 the effect sizes observed for the intervention on pain and function were small and further reduced to no effect when pooling large-blinded RCTs only. An SR analysed the OMERACT-OARSI response and found that patients treated with HA were more likely to achieve such a response than those receiving placebo (RR, 1.11 (1.01 to 1.20)).30 Likewise, when compared vs IA GC, the effect sizes of the intervention were small on pain and function. Of note, one study favoured IA GC in the 1-week to 2-week assessment and HA from the 7–10 weeks until the 17-week to 29-week evaluations.48 In other SRs, there were no differences between groups in most RCTs analysed, although pooled OMERACT-OARSI responses reached statistical significance (RR, 1.15 (1.02 to 1.30)).30 Finally, one SR compared HA compounds and showed an increasing effect with increased molecular weight (MW).22 Of note, the number of studies included was rather low and no differences were seen in QoL.
Most SRs of HA reported moderate to high heterogeneity between studies, as well as publication bias and other biases, mostly concerning inadequate blinding, allocation concealment, and reporting.
Against placebo, GC compounds showed small to moderate effect sizes for pain and function in the short-term (until 3 months), and no differences in QoL, stiffness or joint space width.23 Among GC compounds, MPA shows a faster onset of effect on pain and function than TA or TH at 6 weeks.34 No differences were detected after this time-point as well as in OMERACT-OARSI response and no pooled analysis was performed for this comparison. As with HA, authors underline inadequate blinding and allocation concealment as possible sources of bias in the included RCTs.
PRP was evaluated mostly against HA and, secondarily, versus placebo. Compared with HA, PRP showed a small to null effect on pain, function, and stiffness. Two SRs pooled composite scores (WOMAC total score and IKDC) and found better responses with PRP than HA at 6 and 12 months showing large effects.27 49 Kanchanatawan et al25 found an improved EQ-VAS at 12 months with PRP.25 For PRP versus placebo, no differences were seen in the targeted outcomes, except for the composite scores, in which the pooled effect was large; this effect disappeared when only high-quality trials were pooled. Between-trial heterogeneity was high, in terms of PRP composition, endpoints, and comparators. Also, the SRs rated included RCTs as with moderate to high risk of bias, especially due to inadequate allocation concealment, blinding of participants, and outcome assessment.
A network meta-analysis analysed the effect of MSC against different comparators, including placebo, HA, or IA GC.24 The effect of MSC was moderate to large on pain and moderate for the KOOS at 12 months, whereas no effect was observed on the WOMAC total score at 6 months. High-dose adipose-derived MSC showed a longer effect. Overall, studies included in this SR were rated as of low risk of bias; nonetheless, there was evidence of publication bias for pain measured by VAS. Unfortunately, most branches of the meta-analysis were underpowered to draw conclusions on which strategy is better in clinical practice.
Hip osteoarthritis
The main results on hip OA are summarised in table 3. The most frequent outcomes measured were pain and function, the latter measured using the Harris Hip Score (HHS) and the OMERACT-OARSI response criteria.
Main efficacy outcomes for hip osteoarthritis
PRP was the most frequent compound studied in hip OA, and all comparisons were against HA. Almost all RCTs showed no difference between groups at all time points except for the study by Ye et al,42 favouring PRP. Regarding function, no differences were seen using the WOMAC function subscore or the HHS. An SR of four RCTs with high heterogeneity and unclear or high risk of bias showed inconclusive results.41 50 51
No differences were observed for pain, function nor OMERACT-OARSI response between HA and placebo or MPA. McCabe et al,38 on the contrary, reported an OR=7.8 (2.7–22.8) for reaching an OMERACT-OARSI response in patients treated with IA GC versus placebo. The latter SR included four RCTs, three of which showed better results in function (activities of daily life and WOMAC function subscore). All studies were deemed as having a low to moderate risk of bias and no evidence of publication bias.
Shoulder capsulitis
Table 4 summarises the main efficacy results for shoulder capsulitis. Pain was only measured using VAS and function evaluated by the range of motion (ROM). Additionally, specific composite scores such as the Shoulder Pain and Disability Index (SPADI), the American Shoulder and Elbow Surgeons score and (ASES), and the Constant score were applied. HA and IAGC were the interventions evaluated and most comparisons were against placebo. One SR44 assessed the former and found no differences for pain or function. On the contrary, IAGC were evaluated in two SRs and a small effect was observed favouring the intervention on pain, ROM, and the SPADI whereas no differences were seen for the ASES and the Constant score.
Main efficacy outcomes for shoulder capsulitis and rheumatoid arthritis
Overall, there was high heterogeneity between studies regarding injection techniques dose and type of compound as well as comparators. Major sources of bias were inadequate blinding of participants and personnel, inadequate allocation concealment, and possible small study bias.
Rheumatoid arthritis
The main results of IAT in RA are also shown in table 4. Outcomes varied widely and included pain, ROM, global inflammation, number of flares, and grip strength. HA, IAGC, and yttrium synovectomy were the interventions assessed. Saito and Kotake47 observed better performance of HA over placebo for pain, global inflammation, and self-reported effectiveness. Brazilian Medical Association34 found no differences in the number of flares, ROM, morning stiffness, grip strength, Ritchie articular index, or thermography index, between MPA, TA, or TH. In one RCT, TH performed better in pain (VAS) at 1 week of follow-up but there were no between-group differences at 2 to 6 weeks. Finally, Heuft-Dorenbosch et al46 found no differences in pain between yttrium synovectomy and placebo or IAGC, whereas the former performed better in ROM and knee circumference (1 RCT) versus placebo. Conversely, ROM was best improved in the IAGC-treated group (vs yttrium synovectomy). Two out of three SRs assessing treatments for RA were deemed as of low quality and included a very low number of RCTs with evidence of small study bias and unclear or inadequate allocation concealment, as well as participant and provider blinding.
Safety of intra-articular treatments
Twenty-two SRs provided data on safety (table 5). In most cases, the outcome reported was the frequency of AEs (any), while some articles also analysed SAEs and withdrawals due to AEs.
Main safety outcomes of all included compounds
HA compounds were compared against placebo in a network meta-analysis specifically designed to assess safety in KOA.4 No between-group differences were observed for any AE but local reactions and withdrawal due to AEs favoured placebo versus HA. Other SRs analysing HA compounds reported similar results for any AEs, SAEs, and withdrawals due to AE.
Of note, Rutjes et al7 found a higher risk of local reactions, SAEs, and withdrawals with HA versus sham or no interventions. In this SR, the pooled RR of SAEs from 14 RCTs was 1.41 (1.02 to 1.97), consistent when pooling only large-blinded RCTs (RR=1.55 (1.07 to 2.24)). Said SAEs consisted of 27 events in visco supplementation patients versus 21 in control patients. Most frequent disorders were related to the gastrointestinal system (2 vs 8), cardiovascular system (5 vs 2), cancer (6 vs 0), and musculoskeletal system (4 vs 2). The authors underlined that the poor quality of reporting safety data of the RCTs analysed made the understanding of the probable causes for these observations difficult.
Results on withdrawal due to AEs were obtained after pooling 23 RCTs, but the effect disappeared when restricting the analysis to large-blinded RCTs. One SR reported significant differences between HA and IA GC, favouring the latter for joint pain after injection (17% vs 3.2%).30
Safety results for HA in HOA were also reassuring, with no between-group differences observed for any of the outcomes of interest, except for an episode of septic arthritis, reported in an RCT (vs placebo) included in the SR by Liao et al.37 Other SRs of HA for shoulder capsulitis and RA also did not report differences between groups.44 47
IA GC behaved similarly to placebo without any differences in safety outcomes in all SRs included in this overview for KOA, HOA, shoulder capsulitis, or RA. Of note, Juni et al23 also did not find differences between IAGC versus sham or no intervention, on any AEs, SAEs, or withdrawals due to AEs. Also, this trend remained consistent when comparing different IA GC compounds and doses. In the same line, SRs on PRP for KOA and HOA showed similar safety profiles than its comparators (mostly HA), except for an RCT in the SR by Medina-Porqueres et al41 that found significantly more pain after injection in the PRP group. Finally, results for MSC on KOA were in line with the previously described.
Discussion
To our knowledge, this is the first overview of published SR summarising the efficacy and safety of the most frequently used IA treatments. Based on the available literature, we assessed the performance of five treatment groups in four arthropathies. Most studies evaluated the effects of IAT on KOA and HOA. The average quality of the SRs was moderate, and high heterogeneity was a constant, prompting authors to be conservative when concluding. Most compounds evaluated presented a small effect for relieving pain and improving function, but with inconsistent results and a high risk of bias in most cases. Regarding safety, the frequency of AEs was low, and only a few SAEs were reported, without clear differences between the different injectables assessed.
HA compounds showed a modest effect on pain and function in KOA and RA and no effect on HOA or shoulder capsulitis. Of note, the effects seen for the former, despite remaining, were reduced when pooling only large studies with low risk of bias or longer follow-up.5 7 22 30 31 35 HA showed a better OMERACT-OARSI response in KOA versus placebo and IA GC.5 6 30 35 Only one SR assessed the effects of different HA compounds in KOA and observed differences in favour of those with higher MW on the WOMAC, but authors acknowledge there were too few studies to conclude about the superiority of one group over another.22 Regarding its effect on RA, it should be noted that the only SR addressing this topic included five RCTs performed in Asian populations and efficacy was measured using scales that are seldom used, and evidence of publication bias, so the results should be interpreted with caution.47
The body of evidence of IA GC in the target diseases was smaller compared with that of HA, very likely due to greater industry support for HA. Similarly, its effect versus placebo on pain and function in KOA ranged from a small, but significant, short-term effect to no effect. In contrast, IA GC showed a better, although modest, performance on HOA and shoulder capsulitis. Likewise, no evidence of an effect on QoL or joint space narrowing was observed. One SR compared different IAGC compounds in KOA and found no differences in the outcomes of interest, except for a longer effect of MPA compared with TH.34
Although IA GC have been among the most widely used tools for managing inflammatory arthritis for years, our search strategy did not retrieve any SR including RCTs comparing them against PBO. Only one study evaluated three different GC compounds in RA and found no differences between them in all outcomes evaluated except for pain VAS at 1 week of follow-up in which the analysis favoured TH.
SRs including RCTs on PRP are still limited and our strategy only retrieved articles assessing its performance on KOA and HOA. There were only a few RCTs included and substantial overlapping between SRs. Overall, better performance for pain and function was seen in KOA with large effects reported when pooling composite scores compared with placebo or HA.25 27 29 32 39 This trend was not present in HOA, with only a few RCTs showing modest effects on pain.36 39 41 42 One consistent observation between studies was that the PRP effect lasted longer than its comparators (mostly HA).
MSCs appear to be a potentially promising treatment for OA, but SRs including RCTs are scarce. Our strategy only retrieved one SR in KOA that met our inclusion criteria.24 Moderate to large effects were seen for KOOS and pain, respectively, that lasted until 12 months of follow-up. However, the data in which to draw firm conclusions were scarce. Finally, our thorough search retrieved one SR that evaluated radioisotopic synovectomy for RA in which a modest effect was seen over placebo, whereas it was outperformed by IA GC for some outcomes, such as ROM.46
Although we are aware that safety is best studied in large long-term observational studies, we retrieved information regarding AEs from the SRs of RCTs. Of note, many of them did not report on this aspect.5 6 30 31 33 35–37 39 43 44 The SR specifically aimed at analysing this for individual HA compounds versus different comparators found a frequency of any AE remarkably low and no increased risk or only for local reactions.4 7
Striking differences were seen regarding the number of published articles for the different compounds studied with HA the intervention which has been most widely studied to date. However, this was not translated into a better quality of evidence, preventing authors from drawing firm conclusions regarding many of the studied outcomes. Most of the trials included in the different SRs, especially the ones of PRP and MSC, were highly heterogeneous in terms of the composition of the PRP or the kind of MSC and the procedures used to deliver them. The overall risk of bias within all SRs in this work was high, mostly because of inadequate blinding, allocation concealment, selective reporting, or publication bias.
It should be also noted that, even although all compounds studied presented modest effect sizes, many authors underlined the fact that a proportion of the effect may be due to the placebo effect that accompanies injections5 23 35; something that should be acknowledged when interpreting their results.
This overview of SR has some strengths, such as the comprehensive summary of the currently available IAT including a large number of RCTs. However, it has some limitations. First, including only SRs of RCTs might have precluded the analysis of more recent studies still not included in said reviews, as well as a deeper evaluation of some treatments, such as MSC in OA or GC in inflammatory arthropathies. Second, for the most frequent diseases affecting the shoulder, SRs usually analyse both IA and peri-articular procedures together, which fell out of the scope of the present work, thus leading us to exclude them. Third, most information analysed in this work concerned some frequently assessed outcomes, such as pain and function, but only a few studies examined structural outcomes like joint space narrowing or cartilage volume loss, which are currently receiving more attention.52 53 Finally, a more thorough search in additional databases would have been desirable; but given the large amount of hits retrieved and the fact that we were looking for SRs, the potential selection bias would be kept at a minimum.
In summary, the evidence shows that IAT in the most frequent arthropathies is well tolerated, with a very low frequency of AEs, but only marginally efficacious in the short-to-medium-term when compared with placebo. Nonetheless, it should be noted that the limited data found regarding the efficacy and safety of IAT in inflammatory arthropathies prevented us from drawing firm conclusions.
Data availability statement
Data are available upon reasonable request to the corresponding author.
Ethics statements
Acknowledgments
The authors want to acknowledge the kind supervision of the search strategy by Maria Piedad Rosario-Lozano, from the Agency of Technology Evaluation of Andalusia, Fundación Pública Andaluza Progreso y Salud.
This paper presents independent research supported by the National Institute for Health Research (NIHR) Leeds Biomedical Research Centre (BRC).Professor Pandit is a NIHR Senior Investigator. The views expressed in this article are those of the author(s) and not necessarily those of the NIHR, or the Department of Health and Social Care.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @sdlcrodriguez, @raul_cast_morei, @ElenaNikiUK, @carmona_loreto
Contributors SCR-G, RC-M, LC, JU, and EN contributed to the conception and study design. SCR-G and RC-M performed study selection and data collection. SCR-G, RC-M, LC, JU, and EN analysed the data. SCR-G, RC-M, LC, JU, EN, TWON, MD, MB, HP, IMP, VV, LT, WUK, MADA, FB, EN, IP, and JdlT contributed to the interpretation of the data. SR-G and RC-M wrote the first version of the manuscript and LC revised it critically. All authors read and approved the final manuscript.
Funding This study was supported by a EULAR Task force grant CL109.
Competing interests SCR-G reports grants from The Spanish Rheumatology Foundation during the conduct of the study, and personal fees from Roche, Sanofi, MSD, UCB-Pharma, Bristol-Myers-Squibb and Novartis and non-financial support from Lilly, Pfizer, Sanofi, MSD, Abbvie, UCB-Pharma, outside the submitted work. MD has received personal fees for advisory boards from Grunenthal, Mallinckrodt and Pfizer, and author royalties from UpToDate, and was an investigator in an AstraZeneca-funded, non-drug study (the ‘Sons of Gout’ study), unrelated to this work. LT has received speakers fee from AbbVie, Janssen, Roche, Novartis, Pfizer, MSD, BMS and GE. FB reports personal fees from Boehringer, Bone Therapeutics, Expanscience, Galapagos, Gilead, GSK, Merck Serono, MSD, Nordic, Novartis, Pfizer, Regulaxis, Roche, Sandoz, Sanofi, Servier, UCB, Peptinov, TRB Chemedica, 4P Pharma, outside the submitted work. LC declares that her institute receives grants for studies and research courses from Novartis Farmaceutica, SA, Pfizer, S.L.U., Merck Sharp & Dohme España, S.A., Roche Farma, S.A, Sanofi Aventis, AbbVie Spain, S.L.U., and Laboratorios Gebro Pharma, SA.
Provenance and peer review Not commissioned; externally peer reviewed.