Article Text

Abstract
Objective To evaluate the predictive value of tender joints compared to synovitis for structural damage in rheumatoid arthritis (RA).
Methods A post hoc analysis was performed on a prospective 2-year study of 59 patients with active RA starting on antitumour necrosis factor (TNF). Tenderness and synovitis was assessed clinically at baseline, followed by blinded ultrasound assessment (B-mode and power Doppler ultrasound (PDUS)) on the hands and feet (2 wrists, 10 metacarpophalangeal, 10 proximal interphalangeal and 10 metatarsophalangeal (MTP) joints). Radiographs of these joints were performed at baseline and at 2 years. The risk of radiographic progression with respect to the presence of baseline tenderness or synovitis, as well as its persistence (after 4 months of anti-TNF), was estimated by OR (95% CI).
Results Baseline tender joints were the least predictive for radiographic progression (OR=1.53 (95% CI 1.02 to 2.29) p<0.04), when compared to synovitis (clinical OR=2.08 (95% CI 1.39 to 3.11) p<0.001 or PDUS OR=1.80 (95% CI 1.20 to 2.71) p=0.005, respectively). Tender joints with the presence of synovitis were predictive of radiographic progression (OR=1.89 (95% CI 1.25 to 2.85) p=0.002), especially seen in the MTP joints. Non-tender joints with no synovitis were negatively predictive (OR=0.57 (95% CI 0.39 to 0.82) p=0.003). Persistence of tender joints was negatively predictive (OR=0.38 (95% CI 0.18 to 0.78) p=0.009) while persistence of synovitis was predictive (OR=2.41 (95% CI 1.24 to 4.67) p=0.01) of radiographic progression.
Conclusions Synovitis is better than tenderness to predict for subsequent structural progression. However, coexistence of tenderness and synovitis at the level of an individual joint is predictive of structural damage, particularly in the MTP joints.
Trial registration number NCT00444691.
- Rheumatoid Arthritis
- Synovitis
- Ultrasonography
- Outcomes research
- Disease Activity
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Synovitis (joint swelling or ultrasound-confirmed synovitis) can predict structural progression in rheumatoid arthritis, assessed at the individual joint level, but evidence is conflicting for tender joints.
What does this study add?
Tender joints were least predictive compared to synovitis to predict for structural progression.
Coexistence of tender joints and synovitis at the individual level is most useful, particularly in the metatarsophalangeal joints.
How might this impact on clinical practice?
Synovitis (joint swelling or ultrasound-confirmed synovitis) should be preferred over tender joints in assessing for potential structural progression.
Tender joints should be interpreted together with synovitis when assessing for potential structural progression.
Introduction
Rheumatoid arthritis (RA) is a chronic immune-mediated systemic inflammatory condition with synovitis as the pathological hallmark, presenting with symptoms of joint pain, swelling and also systemic effects such as fatigue. Synovitis has been recognised as one of the most important predisposing factors for subsequent structural damage, which if untreated leads to significant physical disability.1 ,2 Therefore, predicting RA outcomes such as structural damage is crucial for optimal clinical management, in order to effectively identify patients who would benefit from appropriate aggressive therapy at an early stage.3
Joint counts for tenderness and swelling have traditionally been used to assess for disease activity and remain as core data sets used in clinical practice and research.4 Initial disease activity measurements were largely based on evaluation of joint tenderness, such as the Ritchie articular index,5 a semiquantitative scale, later simplified by Hart et al.6 Tender joints continue to be an integral part of clinical assessment of disease activity by its inclusion as one of the core variables in both the American College of Rheumatology (ACR) response criteria as well as the disease activity score (DAS).7 ,8 The tender joint count (TJC) has better interobserver reliability compared to the swollen joint count (SJC); thus, it has a higher weighting than the SJC in the DAS calculation, for example.8–10 It is also more sensitive to change.11 Criteria for reimbursement for biological therapies, inclusion into clinical drug trials and measurement of treatment response usually include a tender joint evaluation.
Longitudinal studies indicate that synovitis, both clinical and by ultrasonography, can predict subsequent structural damage in RA both evaluated at the ‘patient’ level (ie, joint counts) and also at the ‘joint’ level.12–18 However, the predictive validity of tender joints for structural damage is less clear. Conflicting results from previous studies were seen with the ability of TJC to predict for radiographic progression. Wolfe and Sharp19 had found a positive correlation of TJC with subsequent radiographic progression, while Smolen et al20 found that TJC was unhelpful as compared to SJC. More importantly, no studies to date have evaluated tender joints at the ‘joint’ level, and neither has there been a comprehensive comparison with synovitis (evaluated clinically and also by ultrasonography). The aim was therefore to evaluate the predictive value of tenderness compared to synovitis for structural damage in RA.
Methods
Study design
This was a post hoc analysis on the original prospective multicentre 2-year study which evaluated the validity of ultrasound-confirmed synovitis scoring systems in RA.18 ,21 The appropriate ethical committees approved the study and all patients gave their written and verbal informed consent before study enrolment18 ,22 (NCT00444691).
The study had two phases:
Four months of follow-up in patients starting anti-TNF;
Assessment of radiographic progression (evaluation of hands and feet) at 2 years.
Patients
Adult patients fulfilling the 1987 ACR criteria for RA23 were included from March 2007 to August 2008 in the rheumatology outpatient clinics of nine French university teaching hospitals. Patients had to have active disease, enough to require anti-TNF therapy according to the opinion of the investigators. They also needed to have at least more than or equal to six tender and swollen joints on physical examination at time of inclusion.
Centres
Each centre required one dedicated clinician or metrologist (either a rheumatologist or research nurse) with experience in assessment of joint counts as well as one dedicated ultrasonographer (either a radiologist or rheumatologist) experienced in evaluating synovitis in RA (with at least 70 different examinations).
Collected data
Joints were evaluated clinically for tenderness and swelling (clinical synovitis), followed by a blinded assessment for ultrasound (US)-confirmed synovitis in B-mode and power Doppler ultrasound (PDUS) at baseline and 4 months after start of anti-TNF. These included a total of 32 joints for each patient: 10 metacarpophalangeal (MCP), 10 proximal interphalangeal (PIP), 2 wrists and 10 metatarsophalangeal (MTP) joints.
B-mode and PDUS examination was carried out according to a validated scanning method described previously.18 ,21 Evaluation of synovitis, both clinically and by ultrasonography, was standardised among investigators prior to the study during a 1½-day meeting in Brest, France.21 ,24 Interobserver agreement in clinical synovitis had a κ up to 0.62, while agreement in B-mode and PDUS synovitis ranged up to κ of 0.62 and 0.55, respectively.21 ,24
US-confirmed synovitis was defined according to the Outcome Measures in Rheumatology Clinical Trials.25–27 B-mode synovitis scoring was evaluated using a four-grade scale from 0 to 326 with the following subjective definitions for each category: grade 0, absence of synovial thickening; grade 1, mild synovial thickening; grade 2, moderate synovial thickening; grade 3, marked synovial thickening. PDUS synovitis scoring was also evaluated using a four-grade scale from 0 to 327 with the following definitions for each category: grade 0: absence of signal, no intra-articular flow; grade 1: mild, one or two vessels signal (including one confluent vessel) for small joints and two or three signals for large joints (including two confluent vessels); grade 2: moderate confluent vessels (>grade 1) and less than 50% of normal area; grade 3: marked vessels signal in more than half of the synovial area.
For both B-mode and PDUS, a grading of more than or equal to 1 was considered as the presence of US-confirmed synovitis, respectively.
Structural damage
Structural damage of the corresponding joints, assessed clinically, was evaluated by X-rays of hands, wrists and feet; performed at baseline and at 2 years.
Radiographic progression/structural deterioration at the ‘joint’ level was defined as either the appearance or worsening of erosion or joint space narrowing (JSN). This was recorded as a binary variable for each joint (scored 0=no change, or 1=worsening or appearance of either erosion or JSN) in radiographs performed at 2 years compared to baseline. The level of structural damage was defined as the total number of joints with radiographic damage (ie, presence of either erosion or JSN) per patient (range, 0–32). A single experienced reader (VD-P) who was aware of the chronologies of the films but blinded to the clinical and US findings assessed all the X-rays, with a previous interobserver reliability (intraclass correlation coefficient) of 0.80–0.90.28–30
Statistical analysis
All analysis was performed using SAS V.9.2. The statistical analysis was performed on patients with a complete data set (clinical and US evaluation at baseline and after 4 months of follow–up, and radiological evaluation at baseline and after 2 years).
First, radiographic progression in specific joint regions was evaluated by calculating the percentage of joints with radiological progression. Then baseline structural damage (total number of joints with radiographic damage, ie, presence of either erosion or JSN) was evaluated to see if there was any relationship with baseline TJC, SJC, US-confirmed B-mode synovitis count or US-confirmed PDUS synovitis count using Spearman's correlation.
Risk of radiographic progression
The risk of radiographic progression, at the ‘joint’ level, with respect to the presence of tenderness, clinical synovitis or US-confirmed synovitis at baseline, was estimated by OR (95% CI), using generalised estimating equations (GEE) with a logit link adjusting for within-patient correlation (exchangeable correlation matrix), and also other cofactors such as age, gender, disease duration, baseline TJC, baseline SJC, ESR, joint type (PIP, MCP, wrists, MTP) and baseline joint structural damage. These cofactors were determined a priori, as for the previous analysis reported on comparison of the predictive value of clinical and US-confirmed synovitis on radiographic progression.18 GEE allows correction for within-patient correlation between time points and produce estimates of time averaged ORs for binomial data.31
The probability of radiographic progression was initially calculated independently on the joints assessed for tenderness, clinical synovitis and US-confirmed synovitis.
The second step of the analysis calculated the probability of radiographic progression when joints were assessed together (tenderness and synovitis, clinically or by US). The findings in the joints were stratified under the following groups: (1) joints that were tender with no synovitis, (2) tender with synovitis, (3) not tender with no synovitis and (4) not tender but with synovitis. The respective groups were compared to the rest of the other joints that did not fulfil that particular definition so that they were coded as binary variables.
Third, to evaluate specifically whether tenderness in particular locations such as MTP joints would less likely be predictive of structural progression, a subgroup analysis was performed by (1) evaluating only the MTP joints as well as (2) only the joints of the hands (wrist, MCP and PIP joints).
Finally, we checked whether a positive short-term treatment effect on synovitis (either clinical or US) or tenderness enabled prevention of structural progression. For this purpose, joints were divided into two categories: (1) joints that had either persistence of the abnormality at baseline or (2) joints that had normalisation of the abnormality after 4 months of anti-TNF. The probability of observing radiological progression after 2 years with respect to this treatment effect was calculated.
Results
In all, 59 of the 77 recruited patients had completed the study with radiographic evaluation at baseline and 2 years. Table 1 shows the clinical characteristics at baseline of patients with (1) complete baseline data, (2) 4-month data and (3) complete radiographic data at 2 years. There were no statistical differences. Of the 59 patients with complete radiographic data at 2 years, 81% were female, 73% positive for rheumatoid factor, with a mean age of 56 years and disease duration of 10 years. Patients had active disease with mean DAS in 28 joints of 5.1. Regarding anti-TNF therapy, 34 patients were started on etanercept, 23 on adalimumab and 2 on infliximab.
Baseline characteristics of the patients with RA of the various subsets of patients
Radiographic progression was observed in 9% of the 1888 evaluated joints (16% of the 119 wrists, 7% of the 590 MCP, 8% of the 590 PIP and 11% of the 590 MTP joints; table 2). At baseline, 33% of 1888 joints were tender, with the wrist, followed by the MTP joints, being more commonly affected. The wrist was also more often accompanied with tenderness and US-confirmed PDUS synovitis. However, 28% of MTP joints were tender with no evidence of active inflammation (US-confirmed PDUS synovitis) at baseline.
Baseline characteristics of the 1888 evaluated joints of the 59 patients with rheumatoid arthritis
Relationship of structural damage with joint counts at baseline
The relationship of TJC, SJC, US-confirmed B-mode synovitis count and US-confirmed PDUS synovitis count with existing structural damage was evaluated at the ‘patient’ level at baseline. SJC, US-confirmed B-mode synovitis count and US-confirmed PDUS synovitis count correlated positively with the degree of structural damage at baseline (r=0.39, 0.27 and 0.51), respectively. This correlation was not seen with TJC.
Value of baseline tender joints (‘joint’ level) to predict for radiographic progression
Tender joints versus clinical synovitis or US-confirmed synovitis
Structural deterioration, defined as either occurrence or worsening in either erosion or joint space narrowing after 2 years, was observed in 11.9% of the 625 tender joints. For joints that had synovitis, structural deterioration was observed in 12.1% (clinical synovitis), 12.1% (B-mode) and 15% (PDUS), respectively (table 3). Although both tender joints and synovitis (both clinical and US) at baseline appeared to be predictive of radiographic progression at 2 years, baseline tender joints were the least predictive with OR=1.53 (95% CI 1.02 to 2.29) p<0.04. Synovitis, on the other hand, performed better, especially with clinical synovitis with OR=2.08 (95% CI 1.39 to 3.11) p<0.001 (figure 1).
Radiological progression of joints at 2 years according to presence of baseline tenderness or synovitis and when tenderness and synovitis analysed together

Ability of baseline tenderness to predict for radiographic progression at 2 years compared to synovitis.
Tender joints and clinical synovitis or US-confirmed synovitis analysed together
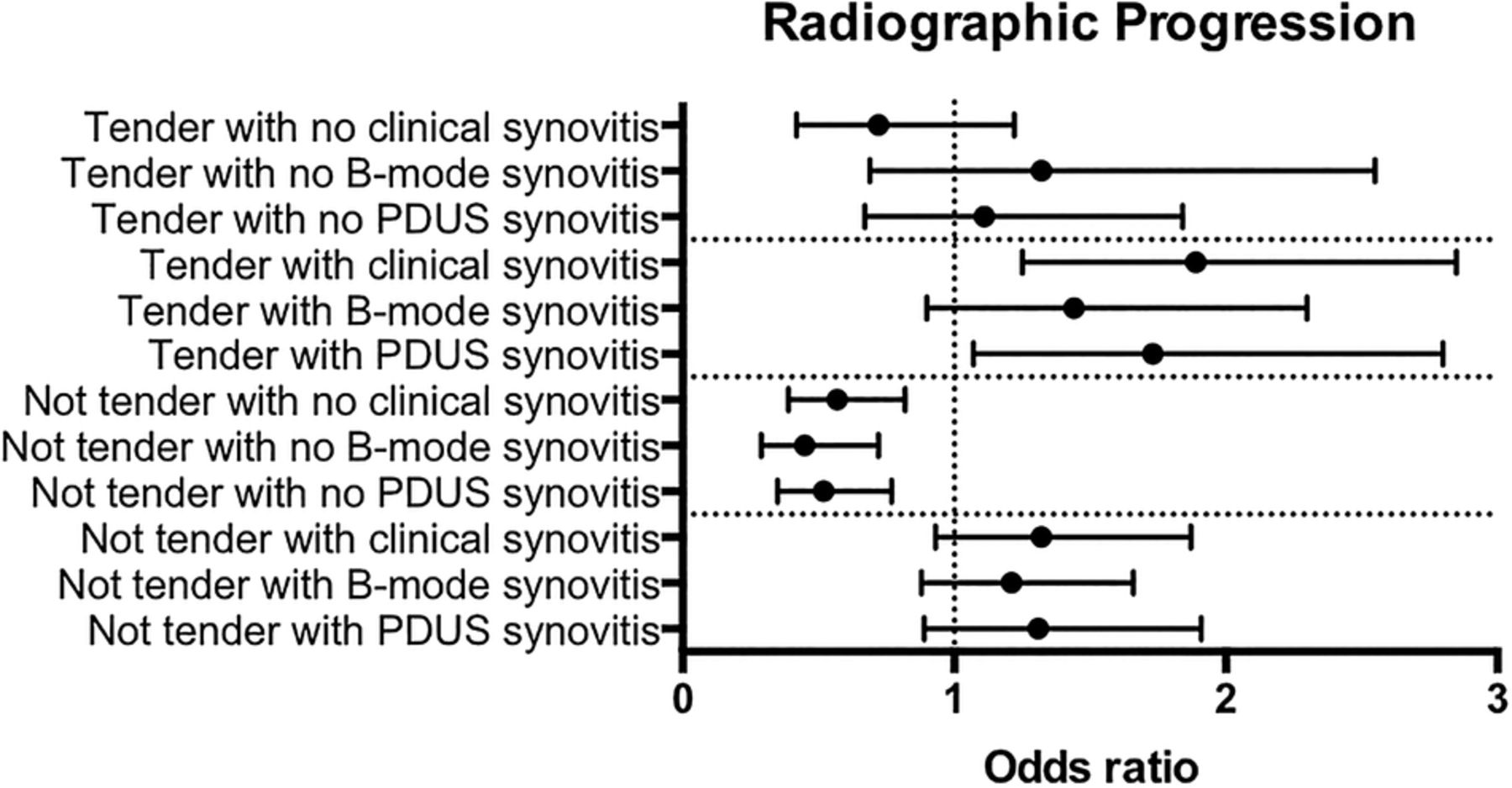
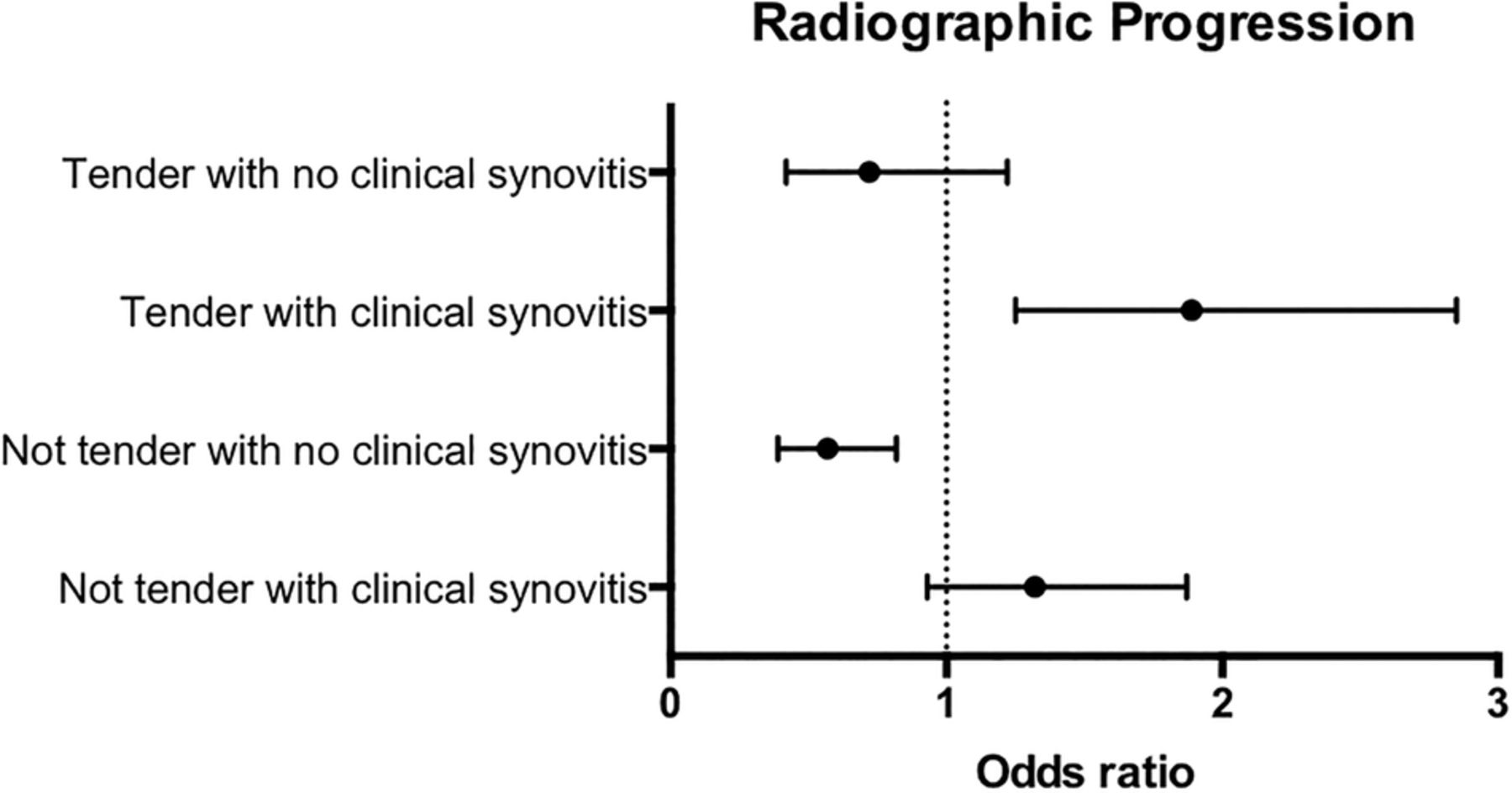
Subsequently, we explored the predictive value for radiographic progression when tender joints were assessed together with synovitis. Joints that were tender with the presence of synovitis (both clinical and US) appeared to be highly associated with radiographic progression. For example, of the 422 tender joints with clinical synovitis at baseline, 14% vs 7.5% had radiographic progression with OR=1.89 (95% CI 1.25 to 2.85) p=0.002) (figure 2 and table 3). There was also a trend in favour of a prediction of radiographic progression in the case of joints that were not tender but had clinical synovitis.

Ability of tenderness and clinical synovitis assessed together, to predict for radiographic progression at 2 years.
On the other hand, for 899 joints that were not tender with no clinical synovitis at baseline, only 6.6% of joints progressed, and were negatively associated with radiographic progression (OR=0.57 (95% CI 0.39 to 0.82) p=0.003). This negative association was additionally observed with US-confirmed B-mode and PDUS synovitis (OR=0.45 (95% CI 0.29 to 0.72) p<0.001 and OR=0.52 (95% CI 0.35 to 0.77) p=0.001, respectively; figure 3 and table 3).
{kind=link}
{kind=link}
{kind=link}
Ability of baseline tenderness and various synovitis definitions (both clinical and ultrasound), assessed together to predict for radiographic progression at 2 years.
Subanalysis on tender joints in the feet
Radiographic progression was seen in 13% of the 239 tender MTP joints. However, tender joints were not associated with radiographic progression (OR=1.20 (95% CI 0.73 to 1.97) p=0.47). A higher proportion of joints with US-confirmed PDUS synovitis had radiographic progression (17% of 128 joints) and was the most predictive of all the assessments (OR=2.65 (95% CI 1.33 to 5.27) p=0.005). Joints with US-confirmed B-mode synovitis also had a positive association with OR=2.24 (95% CI 1.23 to 4.10) p=0.009). There was also a trend in favour of prediction of progression with clinical synovitis (see online supplementary table S1).
Supplemental material
When tender joints were assessed with synovitis, the predictive value improved. MTP joints which were tender had more frequent structural progression if there was concurrent synovitis—clinical synovitis, US-confirmed B-mode synovitis or PDUS synovitis (19.2% vs 9.2%, 15.8% vs 9.6% and 21.4% vs 9.2%, respectively). Radiographic progression ranged from OR=1.96 (95% CI 1.15 to 3.36) p=0.014 for clinical assessment (tenderness and clinical synovitis) to OR=2.83 (95% CI 1.56 to 5.15) p<0.001 by US-confirmed synovitis (tenderness and US-confirmed PDUS synovitis; see online supplementary table S2). On the other hand, this clear positive association was not seen in tender joints without concurrent synovitis, or in the situation when joints had synovitis but were not tender.
When only the small joints of the hands were analysed, joints which were not tender and without synovitis negatively predicted radiographic progression (see online supplementary tables S3 and 4).
Persistence of tenderness versus clinical synovitis or US-confirmed synovitis at 4 months
Finally, the persistence of either tender joints or synovitis with respect to subsequent radiographic progression was evaluated. This was carried out where persistence was compared to joints that had normalisation after 4 months of anti-TNF. Radiographic progression was observed less in joints that remained tender (9.8% vs 19.8%, OR=0.38 (95% CI 0.18 to 0.78) p=0.009)). On the other hand, radiographic progression was observed more frequently in the case when synovitis persisted (16.6% vs 8.9% for clinical synovitis (OR=1.26 (95% CI 0.79 to 2.02), p=0.336); 17.1% vs 5.9% for US-confirmed B-mode synovitis (OR=2.41 (95% CI 1.24 to 4.67), p=0.010) and 20.7% vs 11.9% for US-confirmed PDUS synovitis (OR=1.63 (95% CI 0.75 to 3.57), p=0.218) in joints with versus without persistent synovitis, respectively.
Discussion
This study has confirmed that synovitis, especially detected clinically and also by US, is better than tender joints to predict for subsequent structural deterioration in patients with RA at the ‘joint’ level, both at baseline and its persistence, in the setting of patients who received anti-TNF. However, the data observed in the whole set of joints suggest that the predictive value is best interpreted when both tenderness and synovitis are considered together.
This study has a number of limitations. This was a post hoc analysis of a previous study with the initial primary objective of evaluating the validity of ultrasonography in RA, with a formal follow-up of disease activity up to 4 months. As such, a large proportion of patients from the original study were unable to be included, mainly due to absence of radiographs at 2 years for comparison, and hence contributing to a smaller sample size.
Although there are many known potential predictors of radiographic progression, this analysis (as well as the previous study evaluating synovitis alone18) was focused on the comparison of the variables of tender joints and synovitis, adjusted on cofactors defined a priori. Therefore, this was not a study to extensively explore predictive factors of radiological progression. The list of cofactors remained the same in both analyses to ensure that our results were comparable. In addition, disease activity throughout the total duration of the study was not available and would be an important cofactor when assessing structural progression.
This cohort included patients who had received anti-TNF, which may have reduced the incidence of radiographic progression. However, patients had active disease at inclusion and would have been the group of patients most at risk of getting structural progression. Although metrologists and sonographists participated at a training session, where reliability in clinical synovitis and US-confirmed synovitis was evaluated, there was no formal documentation of tender joint reliability.32 Even though the metrologists were experienced in joint counts, the absence of standardisation in tender joint should be considered in the overall interpretation of results. In addition, the use of a non-validated system for assessment for radiographic progression could have been perceived as a limitation. However, in essence, the analysis was at the ‘joint’ level, and therefore a binary scoring was applied. Although other validated scoring systems such as the Sharp-van der Heidje or even the Larsen system of scoring would be desirable,33 ,34 it reflects radiographic damage at the ‘patient’ level and therefore would not be suitable for this analysis. Additionally, radiographic assessment rested only on the joints that were assessed both clinically and by US, thus omitting some of the joints that would be assessed with the aforementioned radiographic scoring methods.
Most of the studies evaluating the predictive validity of tender joints and radiological changes in the past were at the ‘patient’ level (the total number of joints with synovitis and a summed radiological scoring system), and only a few studies compared the predictive ability of tenderness and swelling in the same cohort.19 ,20 ,35 Although one study showed that both TJC and SJC were not predictive,35 two studies have indicated that SJC had better predictive validity than TJC.20 ,36 We have focused our study by evaluating the risk of structural progression at the level of the joints. The statistical analysis performed also factored into the potential bias of clustering with analysis at the level of the joints by applying GEE. Although GEE is theoretically an analysis for longitudinal studies with repeated measures,31 it is still an appropriate way to factor in potential bias of clustering, especially in studies evaluating multiple repeated measures such as joint count assessments.
An important strength of this study is that tender joints were compared with different forms of synovitis. Considering the increasing use of US in the assessment of synovitis, this study is important in order to further validate the role of US in daily clinical disease activity assessment. As in our previous study, there was no difference between clinical and US assessments of synovitis in terms of its predictive validity for structural progression.18 However, this is a cohort of patients who had active disease, while previous evidence on the superiority of US to predict radiographic progression as compared with clinical synovitis assessment was predominantly in patients with low disease activity or in clinical remission.15 ,41 ,42 In an active group of patients like our cohort, all forms of synovitis assessment were better than tenderness.
In this study, results suggest that the persistence of tender joints was unlikely to result in structural progression. Although further evaluations are required, one possible explanation would be that these tender joints could exist in the context of the ‘fibromyalgic rheumatoid’, where joints no longer had active inflammation despite reported joint pain. The small sample size prevented further subanalysis.
Despite the fact that tender joints were not as predictive as synovitis at baseline for structural progression, the combination of tender joints and synovitis could be clinically useful. This may seem obvious, however, has not been formally reported with US and clinical evaluations concurrently at the ‘joint’ level. Felson et al37 had evaluated combinations of various assessments for predicting structural damage; however, the components included other measures besides the TJC and SJC, evaluated at the ‘patient’ level. These components were predictive with positive likelihood ratios ranging from 3.2 (95% CI 1.9 to 5.3) up to 8.0 (95% CI 3.6 to 17.8).
In early RA, radiographic damage involves the fifth MTP joint early on, suggesting that the joints of the feet are important to assess,29 ,38 with good interobserver reliability.39 It has also been demonstrated that expected joint damage of patients with early RA predominantly occurs in the feet.40 Moreover, in patients who were predominantly foot progressors, the TJC and SJC were longitudinally related to radiographic progression.40 Although we included patients largely with active established RA, a significant number of MTP joints had radiographic progression. Hence, a subanalysis was performed, demonstrating that tender MTP joints are best interpreted in association with synovitis. A tender joint was likely to have radiographic progression only if it was associated with synovitis. One potential limitation was that we did not have information on osteoarthritic changes in the feet, which could have been a potential form of bias.
Conclusion
In conclusion, synovitis is better than tender joints to predict structural progression. The coexistence of both tender joints and synovitis is highly predictive of progression. The persistence of tender joints and its negative predictive ability for structural progression should be further evaluated in other cohorts.
Acknowledgments
The authors thank Abbvie France for financial assistance with the conduct of this study.
References
Footnotes
Twitter Follow Alain Saraux at @alain.saraux
Contributors MD, AS, VD-P, SJ-J, MAD, GC, PG and XM participated in the design of the study and in the collection of data. PPC, KM and MD carried out the design, statistical analysis and drafting of the manuscript. All authors read and approved the final manuscript.
Funding AbbVie France.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Assistance Publique Hôpitaux de Paris.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Additional unpublished data are available from the study on request to maxim.dougados@cch.aphp.fr.