Article Text

Abstract
Objectives Clinical joint activity is a strong predictor of joint damage in rheumatoid arthritis (RA), but progression of damage might increase despite clinical inactivity of the respective joint (silent progression). The aim of this study was to evaluate the prevalence of silent joint progression, but particularly on the patient level and to investigate the duration of clinical inactivity as a marker for non-progression on the joint level.
Methods 279 patients with RA with any radiographic progression over an observational period of 3–5 years were included. We obtained radiographic and clinical data of 22 hand/finger joints over a period of at least 3 years. Prevalence of silent progression and associations of clinical joint activity and radiographic progression were evaluated.
Results 120 (43.0%) of the patients showed radiographic progression in at least one of their joints without any signs of clinical activity in that respective joint. In only 7 (5.8%) patients, such silent joint progression would go undetected, as the remainder had other joints with clinical activity, either with (n=84; 70.0%) or without (n=29; 24.2%) accompanying radiographic progression. Also, the risk of silent progression decreases with duration of clinical activity.
Conclusions Silent progression of a joint without accompanying apparent clinical activity in any other joint of a patient was very rare, and would therefore be most likely detected by the assessment of the patient. Thus, full clinical remission is an excellent marker of structural stability in patients with RA, and the maintenance of this state reduces the risk of progression even further.
- Rheumatoid Arthritis
- Disease Activity
- Outcomes research
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
It is known that clinical joint activity is one of the main predictors of radiographic progression in rheumatoid arthritis, but it is also known that silent progression (without any clinical activity) may occur.
What does this study add?
Our study quantifies the prevalence of silent progression in a real-life cohort of patients with rheumatoid arthritis.
How might this impact on clinical practice?
We could show that silent radiographic progression in an individual joint without any signs of clinical activity also in any other joint is very rare. Thus, aiming at a state of full clinical remission should minimise the risk of silent progression in any joint of this patient.
Introduction
The links between synovial inflammation, joint damage and impairment of physical function are well established in rheumatoid arthritis (RA).1–6 Therefore, joint assessment is a central part of the evaluation of RA disease activity and it was consistently shown that radiographic progression in RA relates to clinical joint activity, especially joint swelling.7 ,8 This is a major reason why most common composite disease activity indices for RA employ swollen joint counts (SJC).9 ,10 Appropriate interference with disease activity according to such scores, therefore, has become the mainstay of RA management and will reduce or halt progression of damage and optimise physical function.11
However, joint progression despite clinical inactivity (‘silent’ progression) has been discussed as a potential risk for patients, as it may go clinically undetected and therefore may not lead to respective treatment adaptations. In particular, a low sensitivity of clinical joint assessment was proposed as a potential explanation for silent progression.12 One possible way to account for this critique would be to use more sensitive methods for detection of residual joint activity, such as ultrasound or MRI. The other possibility, however, is that silent progression in clinically inactive joints is detectable in patients who have significant activity in other joints, since the proinflammatory cytokines released from these joints are known to exert local and systemic osteoclastogenic effects13 and thus could induce continuation of some joint damage via such systemic effects, especially in patients in whom osteoclasts are already active and have led to damage. The first part of our study explores how frequently this clinical situation is present.
In the second part of our study, we will investigate the association of disease activity and progression on the level of the individual joint. The existing literature on this topic has been partly inconsistent, because some associations were performed on the patient level only,7 ,14–18 and because the temporal gap between active disease (disease process) and manifestation of joint damage (disease outcome)14 is neglected in cross-sectional analysis. Thus, we will adopt a joint level analysis with consideration of joint activity longitudinally over several years to address this topic.
Methods
Database and patient selection
The basis of our analysis was a clinical practice data set of patients with a confirmed diagnosis of RA (based on the evaluation of the respective classification criteria at the time)19 ,20 who were 18 years or older. All routinely performed clinical, functional and radiographic assessments were documented for all visits since 1998.21 All therapies were initiated and adapted according to the clinical needs at the discretion of the treating rheumatologist and were also documented in the database. All data were accrued before the study was designed and none of the evaluators of joint activity or radiographs were aware of the questions raised in this study.
We selected only patients in whom at least one joint of the hands (wrist, metacarpophalangeal joints (MCP) or proximal interphalangeal joints (PIP)) had radiographic progression (increase≥1) on the Sharp van der Heijde score (SHS)22 ,23 over an observation period of 3–5 years. This was done to exclude the non-progressing patients, who would not be informative for our study. Importantly, the ‘baseline X-ray’ in our study was not necessary the first X-ray taken from the patient as we also included clinical data 1 year prior to the first X-ray. No further restrictions, such as by treatment, disease duration, laboratory results or comorbidities, were applied. We considered radiographic progression in the 22 hand and finger joints (PIPs, MCPs and wrists), for which matching clinical joint assessment was available retrospectively.
Clinical data on individual joints (swelling and tenderness), as well as disease activity data and laboratory results on the patient level, were extracted from the patients' charts for each clinical visit performed between 1 year prior to the baseline radiograph of this study until the time of the X-ray end point. Typically, these clinical data are documented every 3 months.
All eligible patients had at least one radiographic follow-up over a period of 3–5 years with a minimum of 10 clinical visits after the baseline assessment to ensure that the clinical data were representative of the observation period. The period of at least 3 years of radiographic observation was introduced to allow for a higher sensitivity for progression, and a greater specificity for non-progression. If a patient had more than one X-ray performed between years three and five from the index (baseline) radiograph, the earliest one was chosen for reasons of best data consistency.
Clinical assessments
Patient demographics, such as age, gender and disease duration, as well as treatment type and status, were collected from the patients' charts. Clinical tender and SJCs were performed using a 28 joint count (shoulders, elbows, wrists, metacarpophalangeal joints, interphalangeal joints of the thumb, PIP, and knees;24 (TJC and SJC, respectively). Joint assessment was performed by two trained biometricians with good inter-observer reliability (ICC 0.8; 95% CI 0.77 to 0.83), in accordance with the recommendations by EULAR, classifying a joint as swollen and/or tender only if this was beyond doubt.25
For the evaluation of pain, patient global assessment (PGA) and physician (evaluator) global assessment (EGA) of disease activity, visual analogue scales were used. To assess physical function, the Health Assessment Questionnaire Disability Index (HAQ) was performed at every outpatient visit.26 Additionally, laboratory results (including C reactive protein (CRP) and erythrocyte sedimentation rate (ESR) as well as rheumatoid factor (RF) and anticitrullinated peptide antibodies (ACPA) had been collected at every routine visit. Rheumatoid factor was routinely determined using nephelometry. For ACPA testing, IgG antibodies against cyclic citrullinated peptides (CCP2 test, second-generation assay) were measured on an ImmunoCAP250 using the EliA-CCP assay. These tests did not change during the observational period.
Disease activity was evaluated using the simplified and clinical disease activity index (SDAI, CDAI) and the disease activity score based on 28 joint counts, 4 variables and ESR (DAS28).24 ,27–29
Radiographic assessments
All radiographs were scored according to the SHS22 ,23 by a trained reader (GS), unblinded for sequence but blinded to clinical assessment. Joints were scored for erosions (grade 0–5 per evaluated joint; 0=no erosion, 5=complete collapse of the joint or the total surface of the joint being affected) and joint space narrowing (JSN; grade 0–4; 0=normal joint space, 4=bony ankylosis or complete luxation of the joint). Thus, on the individual joint level, the SHS can amount up to 9, while the maximum SHS in the hands of a patient can be 280 (160 for erosion and 120 for JSN score).22 Progression at the joint level was defined as a minimum increase of 1 (either in the erosion score or in the joint space narrowing score). Since the small joints of the wrists (the carpometaphalangeal joints, the radiocarpal joint, the scaphocarpal joint, the radioulnar joint as well as the os lunatum, os scaphoideum and os trapezium) are scored separately in the SHS, we summarised them and defined a minimum increase of 1 (either in erosion or in joint space narrowing) in any of these joints as radiographic progression of the wrist region. Intrareader reliability on the SHS was high with an ICC of 94% in a subset of 41 images that were read twice; inter-reader reliability was also high with an ICC of 98% in a subset of 28 patients that were scored by two readers (GS and KK).
Statistical analyses
We first descriptively investigated the frequency of joints without clinical activity but with radiographic progression. Hereby, we addressed the first question of our study: does silent progression exist, and can clinical monitoring of all 28 joints be used to prevent it?
We then compared patients with radiographic progression only in joints with present or past clinical activity to patients with radiographic progression and no current or past clinical activity in the respective joint(s). The latter patients could of course also have one or more other clinically active joints, with or without radiographic progression. Differences between these groups in clinical variables, such as levels of CDAI, SDAI, DAS28, PGA, EGA or CRP, or treatment status were investigated.
In a subanalysis, we evaluated joints without radiographic damage at baseline for their radiographic progression.
Finally, we investigated the association between proportional duration of clinical activity (ie, time with documented swelling or tenderness divided by whole observation time, including activity 1 year prior to the baseline X-ray) and radiographic progression. We therefore used logistic regression analysis employing—in separate univariate models—either per cent of time clinically swollen, tender or both as independent variables, while in all models any progression in SHS in the respective joint (ie, change of ≤0 vs >0) was used as the dependent variable.
For statistical analyses, we used IBM SPSS software (V.20.0). T-Tests were performed for continuous data; analyses of variance were conducted for multiple group comparisons; and Pearson's χ2 tests were used to analyse categorical variables. Except for the initial descriptive assessment (see above), all analyses were primarily performed on the individual joint level.
The study was approved by the local ethics committee (ethics committee of the Medical University of Vienna) and conducted according to the guidelines of the Declaration of Helsinki. All patients on our register gave written consent to use their data from the database.
Results
A total number of 279 patients (81.4% female) with a mean±SD number of 16.5±4.8 visits fulfilled the inclusion criteria for this study. Their baseline demographic and disease characteristics are shown in table 1. The mean observation period amounted to 4.1±0.7 years with a mean progression in total SHS of 5.8±15.4 (3.0±6.8 for JSN and 2.7±9.7 for erosion). During the observation period, the mean±SD radiographic progression per joint (non-progressing joints included) was 0.3±1.4, 0.1±0.8 for erosiveness and 0.2±0.8 for narrowing. Among the progressing joints (n=943), the mean progression per joint progressing radiologically (non-progressing joints excluded) was 1.9±2.0 (out of a total maximum score of 9), 1.8±1.3 for single joint erosion score (out of maximally 5), and 1.5±1.2 for single joint narrowing score (out of maximally 4). These data indicate that only relatively few individual joints had progression of both erosions and JSN (see below).
Baseline characteristics of all 279 included patients
What is the extent of progression when patients are regularly monitored aiming at remission?
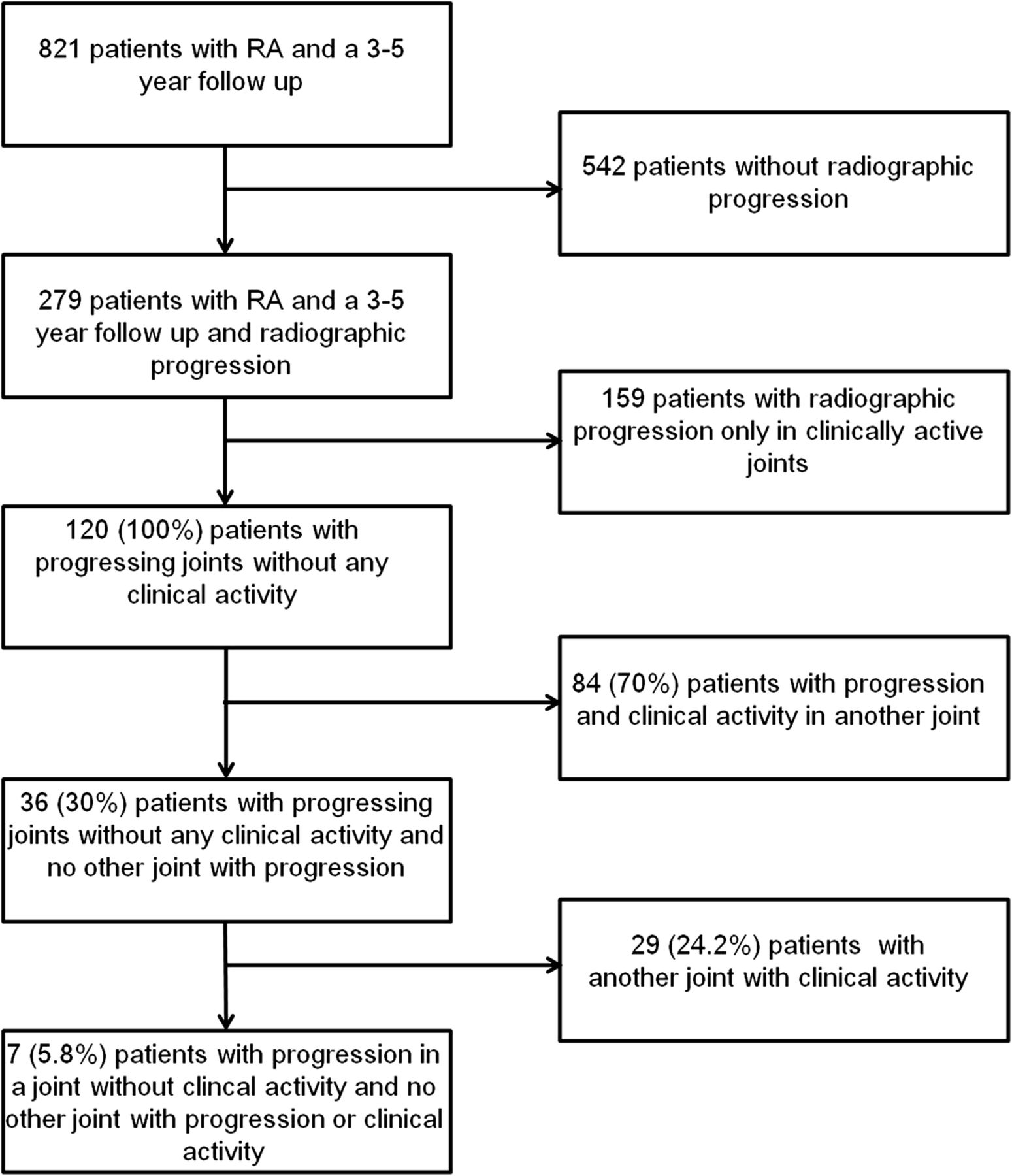
Figure 1 depicts a flow chart of the basic results among the 279 evaluated patients with radiographic progression; 159 (57.0%) of them showed progression only in joints that were clinically active (swollen and/or tender) at least once during the observation period. Of the 159 structurally progressing patients with active joints during the overall observation period, 63 (39.6%) showed changes in the overall joint space narrowing score, 22 (13.9%) changes in the overall joint erosion score and 74 (46.5%) progression in both. In these patients with radiographic progression, the mean number of joints with radiographic progression was 3.0±2.4. This number was similar for the joints that were only swollen (3.0±2.2) and those only tender during the observation period (3.0±2.4). In 132 of the 159 patients, clinical activity was seen only in the year before the baseline radiographic assessment, but not after this first radiograph was taken.
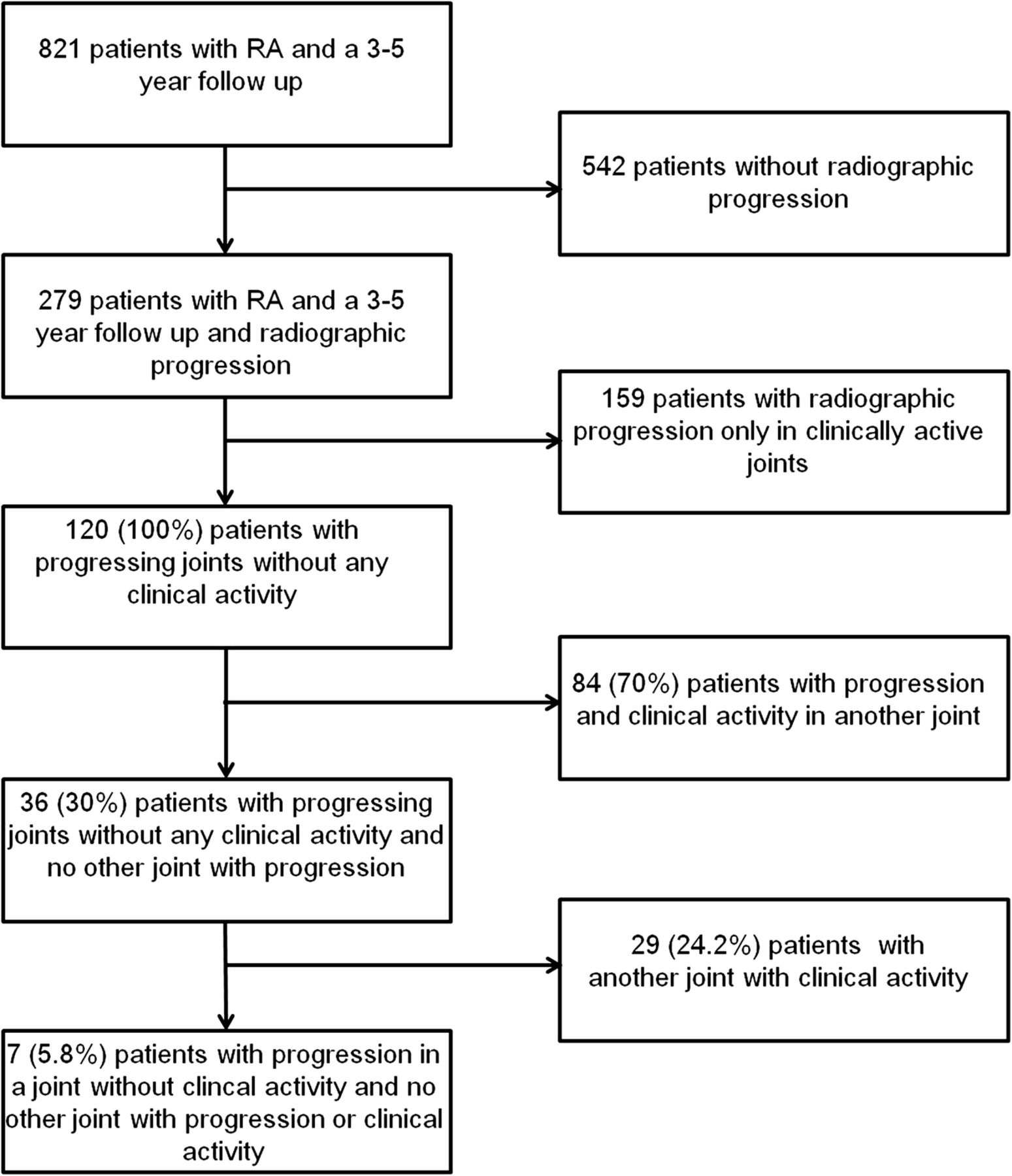
Distribution of patients with X-ray progression with or without signs of clinical activity. From a total number of 821 patients who had X-rays performed in a 3–5 year interval, only 279 showed radiographic progression. Excluding patients with radiographic progression in clinically active joints or any other joints with clinical activity finally left only 7 patients (5.8%) with radiographic progression despite clinical inactivity. RA, rheumatoid arthritis.
Of the 279 patients, 120 (43.0%) exhibited one or more joints with radiographic progression despite clinical inactivity in that joint (absence of swelling and tenderness during the whole observation period including 1 year prior to the baseline X-ray), with progression of erosions seen in 22 (18.3%), progression of JSN in 59 (49.2%) and progression of both in 39 (32.5%). For the 120 patients without any clinical activity in the progressing joints, the mean number of joints with radiographic progression was 2.0±1.4.
Among these 120 patients (figure 1), 84 (70%) had at least one other joint in which progression of damage occurred in the presence of swelling or tenderness (like in the 159 patients described above), possibly suggesting that the events ongoing in these joints may have influenced damage in the apparently clinically unaffected joint.
Twenty-nine of these 120 patients (24.2%) showed clinically detectable disease activity in at least one other joint, although that joint did not progress. Together with the 84 patients just mentioned above, this eventually leaves only 7/120 patients (5.8%), who had a joint with progression of structural damage without any appreciable clinical activity as indicator for a progression (figure 1). Focusing on clinical swelling only, we found a similarly small proportion of patients showing progression in joints without clinical swelling and without any other swollen joint during the observational period (11/173; 6.4%).
Differences between patients having structurally progressing joints with or without clinical joint activity
Patients with radiographic progression in individual joints without apparent clinical disease activity (n=120; figure 1) had significantly lower levels of HAQ, PGA, EGA, pain scores, CDAI, SDAI and DAS28 compared to patients with progression in clinically active joints (table 2; p<0.01 for all). Interestingly, in patients with radiographic progression, despite clinical inactivity, HAQ values improved during the observation period (mean±SD HAQ change −0.09±0.70, while physical function deteriorated in those being clinically active (HAQ progression+0.12±0.76; p<0.001).
Differences in clinical variables at baseline in patients with radiographic progression in clinically active/inactive joints
Baseline SHS, on the other hand, was significantly higher in patients who had clinically inactive progressing joints compared to patients with clinically active progressing joints (59.7±73.4 vs 40.1±53.4; p<0.015). Importantly, in those seven patients with radiographic progression without any clinical activity baseline, SHS was even higher with a mean±SD of 146.5±194.4 and at least three of them had high ACPA levels (mean±SD ACPA level of 213.9±282.8 U/mL).
Influence of various treatment regimes
The majority of the patients received conventional synthetic (cs) disease modifying antirheumatic drugs (DMARDs) for over 50% of the observation period, while 24.0% of the patients were treated with biological agents for more than 50% of that time. There was no significant difference in frequency of radiographic progression in clinically active/inactive joints comparing patients treated with a biological agent for more or less than 50% of the observation period (p=0.69 and p=0.19, respectively). We refrained from statistical modelling of treatment effects, as the composition of treatment segments was highly heterogeneous and variable in duration, and there is an established lag time between treatment effect and structural progression.14
Association of clinical joint activity (swelling and tenderness) with progression on the joint level
When assessing all 6138 joints of the 279 patients with progression of SHS, we found this progression to be confined to 943 (15.4%) of these joints. Of these, 267 joints (28.3%) progressed in their erosion score, 533 (56.5%) in their narrowing score and 143 (15.2%) in both (figures 2 and 3). Of all joints with progression in erosions, 44 were swollen (16.5%; in 29 patients) and 34 were tender (12.7%; in 28 patients) at least once and 121 joints (45%; in 76 patients) were swollen and tender during the observation period (figure 2). Interestingly, 57 joints (6.2%; in 40 patients), which showed progression, were clinically active only during the year prior to the first X-ray, but not within the observation period, indicating a potential carry-over effect of past disease activity (or continuing subclinical disease activity) until damage manifested, as previously described.14 38 (0.6%) joints had undergone joint replacement surgery and were thus not included for further analysis. Figure 2 depicts the distribution of swelling and tenderness in joints with radiographic progression as well as the percentage of time of clinical joint activity.

Distribution of swelling and tenderness in joints with or without x-ray progression. First, we separated joints into those with or without X-ray progression (squares in the second line). Joints with X-ray progression were further separated into those progressing in erosion (light grey), joint space narrowing (JSN, brown) or both (dark grey), as shown in the first circle. Then we evaluated how many of the joints were tender (blue), swollen (red), both (green) or none of them (light blue) during the observational time (second line of circles). In the last line of the figure, we show the respective per cent of time the joints were swollen or tender (red and blue bars). There was a significant difference between the number of swollen and tender joints between joints with or without X-ray progression as well as between the mean time of swelling and tenderness (p<0.0001 by *chi2 and by **t-test). Clinical assessments were regularly performed every 3 months.
{kind=link}
{kind=link}
{kind=link}
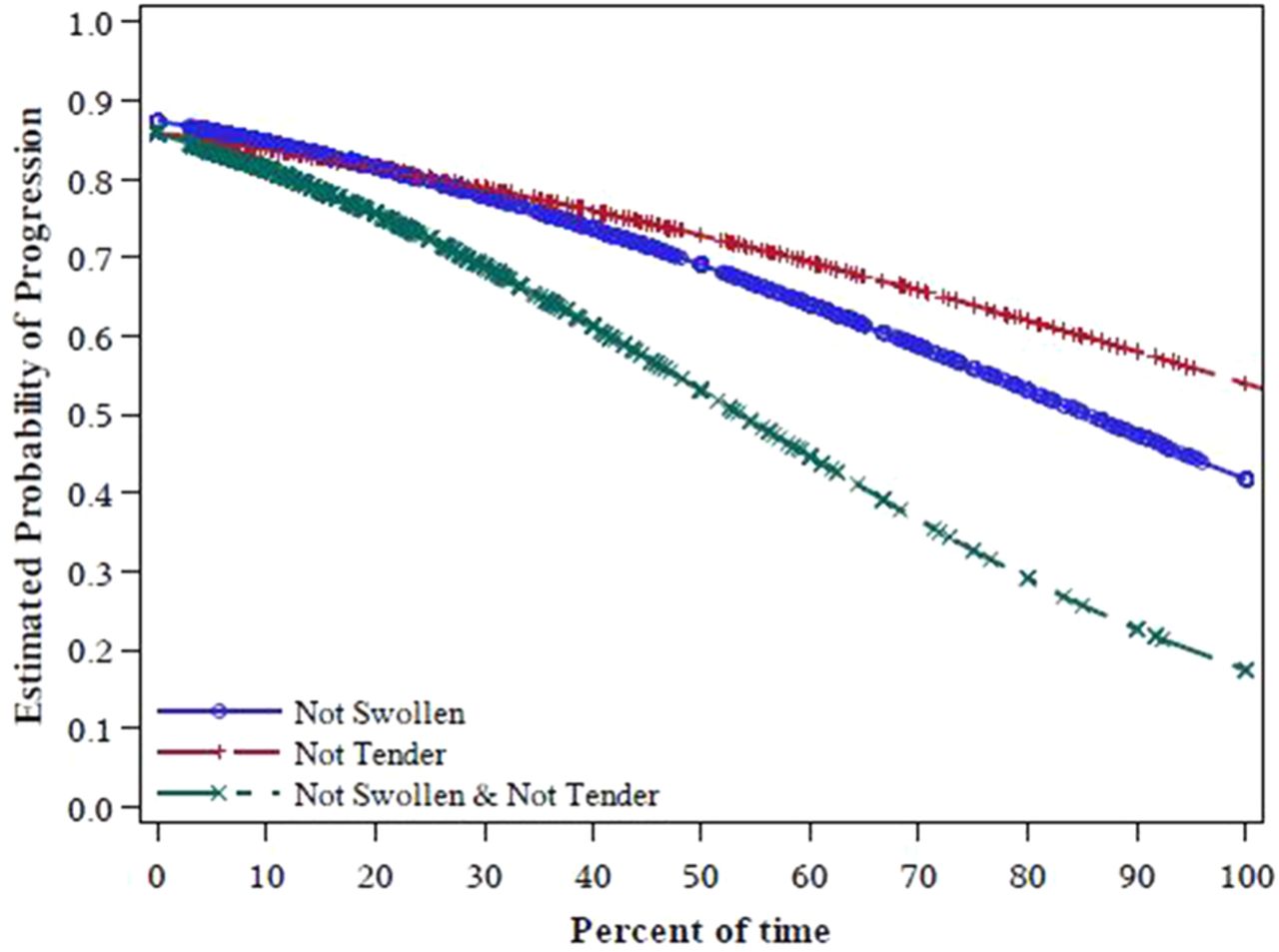
Probability of progression by time clinical inactive (% of total observational time) and radiographic progression. It is shown that the longer the joint was not swollen (blue line), not tender (red line) or not swollen and not tender (green line), the lower was the probability of radiographic progression (p<0.0001 for all).
Among the mentioned 6138 evaluated joints, 5157 (84.0%) showed no progression of joint damage during the observation period; among these, 2896 (56.2%) joints were clinically active during that time: 648 (12.7%) were only swollen and 838 (16.2%) were only tender, with 1410 (27.3%) exhibiting swelling and tenderness. The mean percentage of time with clinical activity (ie, swelling or tenderness or both) was significantly shorter in non-progressing joints compared with progressing joints (figure 2; p<0.0001). Further, we found a significantly shorter proportional period of clinical swelling in joints without X-ray progression versus those with progression (14.9±24.2% vs 21.8±27.4% of time swollen during the observation period; p<0.0001). When we evaluated the probability of progression in dependence of the duration of joint activity (percentage of the total time in clinical activity in the respective joint) using logistic regression analysis, we found a significant association (p<0.0001). Conversely, the longer the time in clinical inactivity, the lower the estimated probability for radiographic progression (p<0.0001; figure 3).
Progression in joints without damage at baseline
Of the 943 joints with radiographic progression, 520 (55.1%, in 212 patients) showed no X-ray damage at baseline; 37.5% (195 joints in 71 patients) developed erosions, 56.0% (291 joints in 88 patients) developed joint space narrowing and 6.5% (34 joints in 53 patients) developed both.
No significant differences in percentages of clinically active time, duration of symptoms or duration of biological treatment were found between the patients with new signs of radiographic damage and those with progression in joints already affected at baseline.
Discussion
In this study, we evaluated the influence of clinical joint activity on radiographic progression at the joint level in 279 patients with RA. Previously performed studies mostly included patients from clinical trials, requiring strict treatment regimens, or early patients with RA;30–34 none of these studies had an observation period of 4 years or more and none accounted for potential carry-over effects by also assessing clinical activity during the year before the baseline radiographs, as we did in the present study.
In accordance with previous data,7 we found that the majority of the joints with radiographic progression showed clinical activity such as swelling, tenderness or both at least once during the observation period. Only 6.2% of these joints exhibited clinical activity solely prior to the first X-ray, implying progression due to a putative carry-over effect. Nevertheless, every fourth joint with radiographic progression never showed any signs of clinical activity, not even during the year before the baseline X-ray; taking this finding to the patient level, every second individual had at least one such clinically inactive but radiographically progressing joint. However, among these patients, 94.2% had clinically active joints at another location, indicating that on the patient level only very few patients with inactive but progressive joints had full clinical remission. This is well in line with findings that patients fulfilling stringent clinical remission criteria, such as the ACR-EULAR criteria, are very rarely afflicted with residual sonographic synovitis and have very good physical function.35–37 Further, it was shown that keeping a state of stringent clinical remission seems to be equivalent to sonographic remission considering radiographic progression.38
Explanations for such damage progression despite clinical inactivity or progression of joint destruction in joints distant from the clinically active joints can only be speculative: (1) patients could have subclinical synovitis as shown by some sonographic studies,39 but also by the fact that according to the EULAR handbook of standard methods doubtfully active joints are considered as not clinically active;25 on the other hand, sonographic data per se are often not unequivocal;36 ,40–42 (2) in an experimental model, Lefevre et al43 showed that activated synovial fibroblasts can move from an inflamed joint to a distant, unaffected joint and elicit damage, since fibroblasts can drive osteoclastogenesis;44 (3) autoantibodies, in particular anti-CCP antibodies, may activate osteoclasts directly and thus active synovitis may not always be needed;45 (4) pre-existing joint damage may enhance joint destruction either by pure mechanical forces or secondary to microenvironmental mechanisms;46 and (5) proinflammatory cytokines released from active joints can act systemically as evidenced by axial osteoporosis in experimental models and patients with active RA,47 and therefore the presence of significant joint activity might affect damage in distant, clinically quiescent joints, if the damage process has been ignited; indeed, the fact that patients with progression in clinically inactive joints exhibit more damage at baseline supports this possibility.
There are several limitations to our study. First, this study comes from a single centre and confirmatory data from other centres will be needed; however, even in clinical trials with short periods of follow-up, joint damage progression was associated primarily with clinical activity, but some clinically inactive joints also exhibited radiographic progression.32 Second, we focused only on joints of the hands, while the feet are also evaluated by the radiographic scores; however, this allowed assessment of pertinent relationships between clinical and radiographic activity, since the routinely performed 28 joint count does not comprise the feet; moreover, clinical assessment of the feet may be obscured by problems which are not related to RA.48 Importantly, however, we are not aware that hands and feet behave differently in terms of progression of joint damage, even though they may behave differently in terms of detectable clinical activity, a discrepancy which in fact has led to the development of the 28 joint count.24 Third, while data in figure 1 are presented on the patient level, analysis depicted in figure 2 and the models for figure 3 were based on the joint level, and were therefore not independent (multiple joints per patient). Fourth, owing to the various mixed treatment segments over the 3–5 year study period and the lag times associated with structural treatment effects, we refrained from complex modelling of various therapies or using longitudinal data analysis (including multiple X-rays). As a guidance on the magnitude of the effect of therapies, we performed descriptive analyses using duration of the various treatment segments, particularly of biological compounds. Further, interobserver reliability of joint examination is generally low; however, assessments at our clinics are routinely performed by a specifically dedicated team of biometricians to ensure longitudinal reliability. Finally, the data obtained here may not be generalisable to all RA populations, since there can be differences in risk and extent of progression.
Importantly, the time spent with a clinically active joint was significantly predicting progression of structural damage in the respective joint. This association was best for the ‘overall’ activity (swelling and/or tenderness), followed by swelling and tenderness. All these observations support current paradigms and recommendations of achieving full clinical remission (ie, absence of clinical joint activity) in patients with RA,11 ,49 since, on the basis of our findings, this would also warrant the absence of progression in any other joint in most patients.
As expected, patients with progressing joints without clinical activity in these joints showed lower overall disease activity than patients with progressing joints that were clinically active. Interestingly, however, they had significantly higher baseline radiographic scores, further supporting some of the above potential explanations for our findings, as well as the well-established concept that patients with erosive disease are the most likely ones to develop new erosions.50 Our data suggest that this risk even overrules the risk of progression afflicted with (ongoing) disease activity. Further, it has to be mentioned that patients with progression in clinically inactive joints even improved in HAQ values over time, thus suggesting only a small impact of radiographic progression on physical function in these patients.
Conclusion
While damage may progress in some joints despite lack of any clinical activity in these joints, this event is heralded by the presence of significant pre-existing joint damage and occurs very rarely in patients whose disease activity is in full clinical remission. These observations strongly support the importance of using composite measures that include formal clinical joint examinations with the objective of achieving a state of full clinical remission.
Acknowledgments
The authors thank Kerstin Klöckl (KK) for supporting the X-ray reading.
References
Footnotes
Contributors MG carried out data acquisition, analysis, study conception and the writing of the manuscript; IKS carried out data acquisition and drafted the manuscript; FA carried out data analysis and the manuscript revision; GS read all the X-rays and revised the manuscript; HR carried out data acquisition and drafted the manuscript; KM and JS carried out the conception and design and manuscript revision. DA carried out the conception and design and data interpretation and manuscript revision. All authors read and approved the final manuscript.
Funding This work was supported by the Innovative Medicines Initiative Joint Undertaking under grant agreement n°115142 (BTCure) and by funding from the European Community's Seventh Framework Programme (project EuroTEAM; Projectnumber: 305549).
Competing interests None declared.
Ethics approval Ethics committee of the Medical University of Vienna.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.