Article Text

Abstract
Objective To evaluate the responsiveness of a simple routine assessment of patient index data (RAPID3)-like index that includes only 3 patient self-report measures (physical function, pain and patient global estimate) compared to that of traditional composite indices to assess change in patients with axial spondyloarthritis (Ax-SpA).
Methods Devenir des Spondylarthropathies Indifférenciées Récentes (DESIR) is a prospective cohort of patients with inflammatory back pain suggestive of Ax-SpA. The study included 461 patients, who met the Assessment of SpondyloArthritis International Society (ASAS) classification criteria for Ax-SpA. A simple RAPID3-like index was compared with the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) and the AS Disease Activity Score (ASDAS) scores for responsiveness over 6 months. Construct validity was also evaluated through Pearson correlations and discrimination of disease activity through standardised mean differences for the 3 indices.
Results The RAPID3-like index was correlated significantly with BASDAI (r=0.84, p<0.005) and ASDAS-C-reactive protein (CRP) (r=0.74, p<0.005), similar to correlations of BASDAI with ASDAS-CRP (r=0.76, p<0.005). The percentage of patients with inactive disease ranged from 9% to 25% and with high activity from 10% to 45%, according to various measures. The capacity to discriminate between high and low disease activity was similar for the 3 indices. The strength of agreement of RAPID3 with ASDAS-CRP was moderate (0.44) and lower with BASDAI (0.37). Responsiveness over 6 months was slightly higher for ASDAS-CRP and the RAPID3-like index than that for BASDAI.
Conclusions The RAPID3-like index provides similar information to BASDAI and ASDAS-CRP concerning responsiveness over 6 months. RAPID3 appears feasible to assess patients with Ax-SpA quantitatively over time in busy clinical settings.
- Disease Activity
- Outcomes research
- Patient perspective
- Spondyloarthritis
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
The BASDAI and ASDAS-CRP are two disease-specific indices, which are used to assess patients with axial spondyloarthritis (Ax-SpA) in clinical research and at specialised sites. BASDAI is the index that has been used most frequently in RCT, but most recent clinical trials include ASDAS.
What does this study add?
A RAPID3-like index provides similar responsiveness to BASDAI and ASDAS-CRP over 6 months in 461 well-characterized patients with Ax-SpA in the Devenir des Spondylarthropathies Indifférenciées Récentes (DESIR) cohort.
How might this impact on clinical practice?
Quantitative clinical data are more informative than narrative descriptions for improvement in clinical decisions, but appropriate and validated measures are needed.
In busy clinical settings, it is far more feasible to assess all patients, including those with Ax-SpA, with the same patient questionnaire before seeing the rheumatologist, than to attempt to administer different questionnaires to patients with different diagnoses.
Introduction
An index is needed to assess and monitor patients with most rheumatic diseases,1 including axial spondyloarthritis (AxSpA), as no gold standard is available. Different indices have been developed to assess patients with AxSpA.2 The Bath Ankylosing Spondylitis Disease Activity Index (BASDAI)3 and AS Disease Activity Score (ASDAS)4 ,5 are disease-specific indices, which are used widely in clinical research and at specialised sites. However, it is a challenge to incorporate these specific indices into routine standard care in a large number of patients.6 For example, only 29% of rheumatologists reported using a quantitative measure in rheumatoid arthritis (RA) in clinical practice, according to a survey by the American College of Rheumatology.7
Changes in status of most patients with AxSpA (and other rheumatic diseases) are recorded at most busy rheumatology sites only as narrative descriptions, rather than as quantitative data. The only quantitative data in the medical records of most patients seen by rheumatologists in routine care are laboratory tests, the limitations of which led to recognition of a need for indices.1 ,8 This practice may result in a situation in which ‘clinicians may easily write “doing well” in the notes of the patient who has become progressively crippled before their eyes’.9 It is ironic that pharmaceutical companies collect indices to document improvement in patient status for registration of new therapies, but most rheumatologists do not assess an index in patients with Ax-SpA.7
Most indices to assess patients with Ax-SpA (and other rheumatic diseases) include patient self-report measures. Patient questionnaires may be regarded as tools to record information from a patient history as standard, quantitative, ‘scientific’ data rather than only as narrative descriptions.10 Patient history information is far more prominent in clinical decisions concerning diagnosis and management in RA (and likely other rheumatic diseases) than in many other chronic diseases which are dominated by ‘gold standard’ biomarkers.11
A patient questionnaire can be distributed and completed in the waiting area by a patient prior to seeing a doctor, with minimal disruption of office and patient flow, resulting in saving time for doctor and patient, with improved doctor–patient communication.12 However, successful implementation of this process is far more feasible if all patients complete the same questionnaire.
A multidimensional health assessment questionnaire (MDHAQ),13 which includes a simple index, routine assessment of patient index data (RAPID3), has been used effectively in many clinical settings.7 RAPID3 is a composite index based on the three patient self-report core data set measures, physical function (FN), pain and patient global estimate (PATGL),14 which may be calculated on an MDHAQ in about 5 seconds.15 RAPID3 is useful to recognise clinical changes in many other rheumatic diseases, including osteoarthritis, gout, systemic lupus erythematosus, vasculitis as well as Ax-SpA.16–22 Four reports concerning RAPID3 in Ax-SpA indicate high correlations between RAPID3 and BASDAI and ASDAS.19–21 However, these studies do not analyse responsiveness according to RAPID3 in Ax-SpA, compared to AS-specific indices such as BASDAI and ASDAS.
The Devenir des Spondylarthropathies Indifférenciées Récentes (DESIR) cohort is a well-characterised cohort of patients with Ax-SpA seen at multiple French clinical rheumatology sites.23 FN, pain and PATGL were queried at each visit, although not in the same format as RAPID3 on an MDHAQ. Nonetheless, different formats of these constructs are highly correlated18–20 ,22 and provided an opportunity to analyse responsiveness to change in an RAPID3-like index compared to BASDAI and ASDAS in the large DESIR cohort, as presented in this report.
Methods
Patients
DESIR is a prospective cohort in France involving 25 rheumatology centres and 708 patients. Patients were evaluated every 6 months over the first 2 years and annually thereafter. This cohort meets the current Good Clinical Practice Guidelines and has obtained the approval of the appropriate ethical committees. More detailed descriptions of inclusion criteria and baseline characteristics of this cohort have been published.23 The data presented in this study are based on a longitudinal analysis from baseline to 6-month follow-up in 461 DESIR patients who met the Assessment of SpondyloArthritis International Society (ASAS) criteria for Ax-SpA.24
Assessments
Bath Ankylosing Spondylitis Disease Activity Index
The six individual questions to calculate BASDAI were available in the database as 0–10 visual analogue scale (VAS) scores, with 0 representing normal and 10 the most severe status: BASDAI 1—Fatigue; BASDAI 2—Total Back Pain; BASDAI 3—Pain/swelling peripheral joints; BASDAI 4—Enthesitis; BASDAI 5—Severity of Morning Stiffness (MS); BASDAI 6—Duration of MS, with 10 representing a duration of 2 hours or longer.3 To calculate the total BASDAI, the average of questions 5 and 6 (severity and duration of MS) is calculated, added to the other 4 items, and divided by 5 to give a final BASDAI score of 0–10. A cut-point of 4 has been used in trials with tumor necrosis factor alpha (TNF) blockers as the threshold for ‘high disease activity’,25–27 which is similar to the BASDAI cut-point of 3.9 based on patients' perceptions of symptom relief.27 Additional cut-points for ‘inactive’ <2.5 and ‘highly active’ >6.9 disease activity also were analysed.28
AS Disease Activity Score
PATGL and c-reactive protein (CRP) (mg/L) were available to calculate the ASDAS-CRP. The score for ASDAS-CRP (the preferred version of ASAS) is calculated as: ASDAS-CRP=0.12×Back Pain+0.06×Duration by Morning Stiffness+0.11×Patient Global Estimate+0.07×Peripheral Pain/Swelling+0.58×Ln (CRP (mg/L)+1); Ln represents the natural logarithm.4 Cut-off values for disease activity states using ASDAS have been developed: <1.3 for inactive, 1.3–2.1 for moderate, 2.1–3.5 for high and >3.5 for very high disease activity.29
Routine assessment of patient index data-like index
RAPID3 scores are calculated as the sum of the three RA core data set measures included on an MDHAQ: FN, pain, and a PATGL.30 The FN scale is derived from the Health Assessment Questionnaire (HAQ),31 which includes 10 items, 8 from the original HAQ32 and 2 complex activities of daily living designed to overcome ‘floor effects’.33 Pain and PATGL are both scored on a VAS (0–10). The range for RAPID3 is 0–30 and severity categories have been defined for RA: ≤3 for remission, 3.1–6.0 for low, 6.1–12.0 for moderate and >12 for high severity.34
In this report, since patients in the DESIR cohort did not complete an MDHAQ, we calculated a composite index of FN, pain and patient global estimate which we termed ‘RAPID3-like’. FN was scored from a modified HAQ for SpA (HAQ-S) developed by Daltroy et al35 This version was generated by adding 5 items to the original HAQ32 concerning activities more specific for patients with SpA to increase the ability to capture functional limitations. HAQ-S is highly correlated with the original HAQ (Spearman's correlation=0.96).35
Pain was calculated as a composite of back pain (BASDAI item 2) and peripheral joint pain (BASDAI item 3), scored 0–10 and described simply as ‘pain’. PATGL was available in the DESIR database.
Statistical analysis
Mean (SD) values for RAPID3-like, BASDAI and ASDAS-CRP were compared between baseline and the 6-month follow-up using Student paired t-tests. Reliability, construct/criterion validity, the capacity to discriminate high versus low disease activity and responsiveness of the RAPID3-like index were analysed and compared to BASDAI and ASDAS-CRP.
Internal consistency was tested as a component of reliability using Cronbach's α, for each index, as well as the α obtained when each specific item was dropped. The results were interpreted following general rules (α=0.70–0.90 indicates good reliability, <0.70 indicates that included items provide an inadequate contribution to the overall scale and >0.90 indicates redundancy).
Construct validity of the RAPID3-like scores was analysed according to Pearson correlations with BASDAI and ASDAS-CRP (because of their normal distributions). Criterion validity was analysed using PATGL and physician global assessment (DOCGL) as surrogate ‘gold standard’ measures, representing patient and physician perspectives for disease activity. Pearson correlations between PATGL and DOCGL and the three composite indices (BASDAI, ASDAS-CRP and RAPID3-like score) as well as the individual components were also performed, including a version of RAPID3 not including PATGL (table 1).
Summary of single items included in the BASDAI, ASDAS and RAPID3-like indices
Predefined levels of PATGL and DOCGL were applied <1, <3 and <6 cm for ‘inactive’, ‘moderate’, ‘high’ and for ‘very high disease activity’, respectively, as described in the development of ASDAS previously.29 To assess the capacity of the indices to discriminate between patients with high (>6) and low (<3) disease activity states, we calculated the standardised mean difference (SMD) between these two states for each index (difference in the group means divided by the pooled SD of the group means) and also for each individual item.29
In addition, patients were classified using the cut-points for remission/inactive, low, medium and high/highly active scores for BASDAI (2.5, 4 and 6.9),25 ,28 ASDAS-CRP (1.3, 2.1 and 3.5)29 and RAPID3 (3, 6 and 12).34 The level of agreement between categories was evaluated using weighted κ and interpreted according to the Landis and Koch guidelines where <1=no agreement; 0.01–0.20=slight agreement; 0.21–0.40=fair agreement; 0.41–0.60=moderate agreement, 0.61–0.80=substantial agreement and 0.81–0.99=almost perfect agreement.36
The Bland-Altman method also was used to assess agreement between the RAPID3-like index and the two specific indices.37 The RAPID3-like index and ASDAS-CRP were converted to 0–10 scales to be comparable to BASDAI for these analyses using simple mathematical transformations. To convert RAPID3-like, each value was multiplied per 30 (maximum possible value) and divide by 10. To convert ASDAS-CRP, each value was multiplied per 6.16 (maximum value in our data set because ASDAS-CRP has no defined upper level) and is divided by 10. The Bland-Altman method calculates the mean difference between two instruments of measurement (the ‘bias’), and 95% limits of agreement as the mean difference ±2 SDs. It is expected that the 95% limits of agreement include 95% of differences between the two measurement methods. A Bland-Altman plot is included as a visual presentation of the 95% limits of agreement. The smaller the range for difference, the better the agreement between these two methods of measurement.
Sensitivity to change, defined as ‘the ability of an instrument to accurately detect change when it has occurred’,38 was evaluated using receiver operator characteristic (ROC) curves and trough standardised response means (SRM). For ‘change’ defined as improvement, we calculated the minimal clinically important difference for improvement in the patient and physician global.39 A cut-point of 1 (equivalent to 10 mm in 0–100 mm scales) to define improvement for PATGL and for DOCGL from baseline to 6-month follow-up is consistent with a similar cut-point used in previous studies.40–42 The area under the curve (AUC) of the ROC curves for improvement in the RAPID3-like index, BASDAI and ASDAS-CRP were compared for statistically significant differences.43 Since PATGL accounts for a third of the RAPID3-like index, we also assessed a version, which excluded PATGL. Internal responsiveness was evaluated according to SRMs calculated by dividing the mean change between baseline and 6 months by the SD of the change score for each index.
Statistical significance was set at a p value of <0.05; if a Bonferroni adjustment because of multiple comparisons was needed, then the p value was set at less than 0.0125. All the analysis was performed using Stata V.12.0 for Mac (StataCorp LP, College Station, Texas, USA).
Results
Cross-sectional analyses
Mean BASDAI (SD) at baseline was 4.3 (2.0) and 3.4 (2.1) 6 months later, with a mean change of 0.9 units (p<0.001). Mean ASDAS-CRP (SD) at baseline was 2.5 (1.1) and 1.9 (1.0) 6 months later, with a mean change of 0.6 units (p<0.001). Mean RAPID3-like (SD) at baseline was 10.9 (5.8) and 8.4 (6.0) 6 months later, with a mean change of 2.5 units (p<0.001).
Cronbach's α for BASDAI was 0.85 and for RAPID3-like index was 0.82; all items contributed equally and none provided higher internal consistency if dropped. Cronbach's α for ASDAS-CRP was 0.35, with a higher α of 0.77 if CRP was removed (table 2).
Internal consistency through Cronbach's α for each index and values obtained when dropping each single item
The RAPID3-like score was correlated significantly with BASDAI, at r=0.84, p<0.005, and with ASDAS-CRP at r=0.74 (p<0.005), similar to the correlation of BASDAI with ASDAS-CRP of r=0.76 (p<0.005).
Correlations of PATGL with the AS-specific indices ranged from 0.70 for ASDAS-CRP to 0.76 for BASDAI (p<0.005). Since the RAPID3-like index includes PATGL, a high correlation was expected (r=0.90; p<0.005); and a correlation excluding PATGL was calculated as r=0.72 (p<0.005). The BASDAI single items most highly correlated with PATGL were ‘pain’ (calculated as the sum of back and peripheral pain) r=0.76 (p<0.005), back pain r=0.74 (p<0.005) and severity of MS r=0.63 (p<0.005; table 3).
Pearson correlations between PATGL and DOCGL and the three composite indices (BASDAI, ASDAS-CRP and RAPID3-like index) including a version of RAPID3 not including PATGL, as well as the individual components to evaluate criterion validity
Correlations of DOCGL with the AS-specific indexes were r=0.61 (p<0.005) for ASDAS-CRP and r=0.62 (p<0.005) for BASDAI. DOCGL also was correlated with the RAPID3-like index r=0.62 (p<0.005). Correlations between unique items with DOCGL were lower than with PATGL, but nonetheless statistically significant. The BASDAI items most highly correlated with DOCGL were ‘pain’ at r=0.57 (p<0.005), back pain at r=0.54 (p<0.005) and severity of MS at r=0.54 (p<0.005). DOCGL was correlated with PATGL at r=0.58 (p<0.005). The lowest correlations of any individual measure with PATGL and DOCGL were seen for CRP (table 3).
Discrimination between patients with high disease activity/low disease activity and agreement
The mean (SD) value for each index according to high disease activity versus low disease activity is presented in table 4. According to PATGL as the external construct, the SMD was higher for RAPID3-like index (SMD=1.94), followed by BASDAI (SMD=1.33), the RAPID3-like index without PATGL (SMD=1.17) and ASDAS-CRP (SMD=1.08). According to DOCGL as the external construct, the SMD was similar for the three indices ranging from 0.78 to 0.80. As expected, the level of agreement with PATGL was higher for the RAPID3-like index (κ=0.70) followed by BASDAI (κ=0.48) and ASDAS-CRP, which also includes PATGL (κ=0.44). In contrast, the level of agreement with DOCGL was similar for all indices ranging from 0.38 for RAPID3-like to 0.41 for ASDAS-CRP. The strength of agreement of RAPID3 with ASDAS-CRP was moderate (κ=0.44) and slight with BASDAI (κ=0.37). The strength of agreement of BASDAI with ASDAS-CRP was also moderate (κ=0.50) (table 4).
Discrimination between high disease activity (patient or physician global higher than 6) and low disease activity (patient or physician global lower than 3) and level of agreement between the patient and physician global and the composite indices
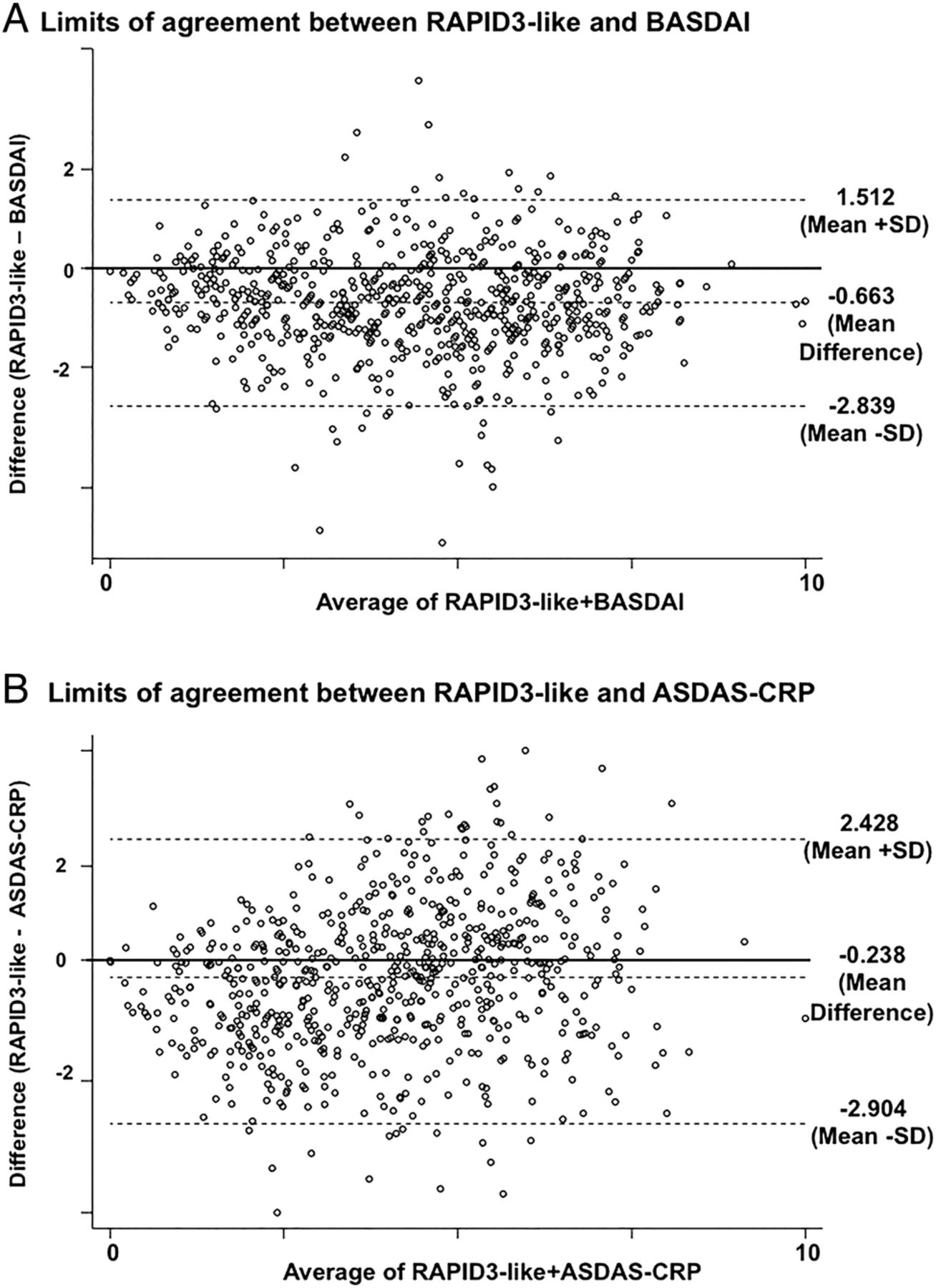
A Bland-Altman analysis indicated that the limits of agreement between the RAPID3-like index and the BASDAI ranged from −2.839 to 1.512, with a mean difference of −0.663 (CI −0.744 to −0.582) (figure 1A) and the limits of agreement between the RAPID3-like index and ASDAS-CRP ranged from −2.904 to 2.428, with a mean difference of −0.238 (CI −0.339 to −0.137; figure 1B). The average difference between these indices may not be considered large enough to be clinically relevant, allowing the use of any of these measures in similar clinical context.
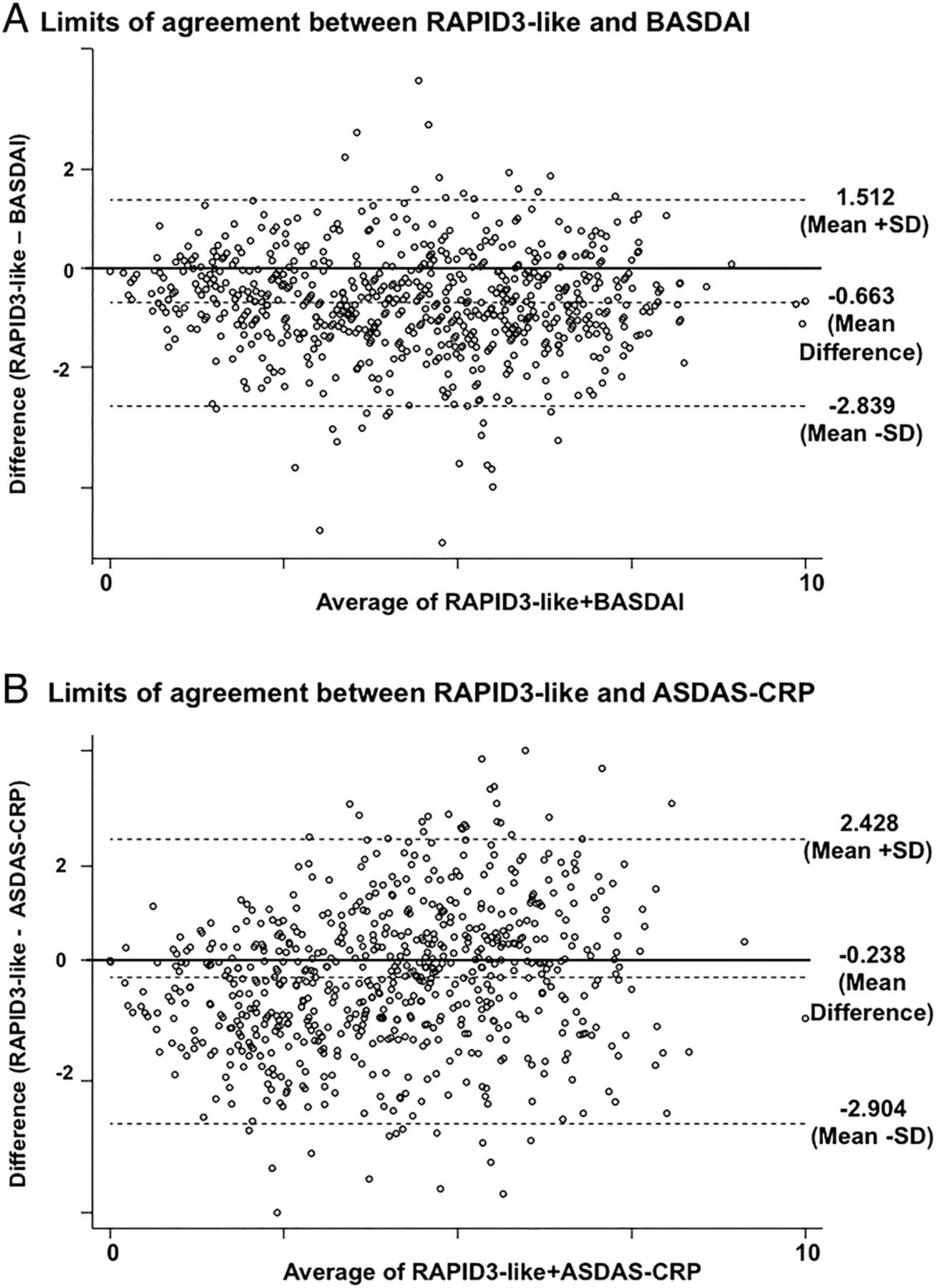
Bland-Altman plots showing agreement between RAPID3-like/BASDAI (A) and between RAPID3-like/ASDAS-CRP (B). The bubble size is determined by the number of patients with that combination of average and difference in both measures. ASDAS, Ankylosing Spondylitis Disease Activity Score; BASDAI, The Bath Ankylosing Spondylitis Disease Activity Index; RAPID3-like, routine assessment of patient index data-like.
Longitudinal analyses: sensitivity to change over 6 months
The responsiveness of the RAPID3-like index was compared with that of BASDAI and ASDAS-CRP based on data from the 403 patients for whom information of all indices was available at baseline and at 6-month follow-up.
According to PATGL improvement, the AUC for the RAPID3-like index (0.952) was greater than that of the ASDAS-CRP (0.865), followed by RAPID3-like score without PATGL (0.825) and BASDAI (0.681) (p<0.001; figure 2A). According to DOCGL improvement, the AUC for RAPID3-like (0.781) was similar to that of ASDAS-CRP (0.786), both greater for BASDAI (0.661), p<0.001 (figure 2B).

{kind=link}
{kind=link}
Receiver operator characteristic (ROC) curves to analyse responsiveness according to two different external criteria: improvement by PATGL (A) and by DOCGL (B). The values for the area under the curve (AUC) are shown at the bottom of graph. Statistical significance was set at p<0.016 (Bonferroni adjustment for multiple comparisons). ASDAS, Ankylosing Spondylitis Disease Activity Score; BASDAI, The Bath Ankylosing Spondylitis Disease Activity Index; DOCGL, physician global assessment; PATGL, patient global assessment; RAPID3-like, routine assessment of patient index data-like.
The internal responsiveness was similar for the three indices: 0.47 for BADAI, 0.50 for ASDAS-CRP and 0.43 for RAPID3-like (table 5).
Comparison of baseline and 6 months visit for each composite index and SRM
Discussion
Our results are consistent with previous studies, in which BASDAI and ASDAS are correlated at highly significant levels with RAPID3 of r ∼0.7–0.8.18–20 ,22 ,28 Our results extend those findings by comparing measurement properties of the RAPID3-like index to BASDAI and ASDAS-CRP, and by documenting that patient improvement over 6 months in a large, well-studied cohort is similar according to the three indices. Cross-sectional correlations may not necessarily translate into responsiveness to change, which has not been reported previously for RAPID3 compared to BASDAI and ASDAS in Ax-SpA in clinical practice.
RAPID3-like scores are comparable to BASDAI and ASDAS-CRP when classifying patients in different disease activity categories. Categories for disease activity states may be important to guide treatment during clinical practice, and cut-points for low activity are recommended in guidelines for achieving a therapeutic goal.44 The level of agreement between each index and patient or physician global estimate as an external construct was similar, although somewhat higher on the patient global estimate, reflecting evidence of discordance between patient and physician global estimates concerning disease activity.45 Although the level of agreement between RAPID3 and the other two specific indices was moderate, a percentage of patients would be not classified in the same disease activity category when using either index (20% in the case of RAPID3 vs ASDAS-CRP and 26% for RAPID3 vs BASDAI).
BASDAI and ASDAS-CRP are valid and reliable measures for AS, quite useful in clinical trials, other clinical research and clinical care in specialised SpA settings but more difficult to use in routine rheumatology care. The primary reason to introduce a more generic index to assess Ax-SpA is based on feasibility of collecting different questionnaires from patients with different diagnoses in busy clinical settings. Almost all settings in which measurement of clinical status is successfully performed in routine care have patients complete the same questionnaire. The same MDHAQ/RAPID3 can be used for patients with all rheumatic diagnoses17–22 and may be helpful to assess status in patients in whom no diagnosis is established, including patients new to a rheumatology setting.
Our study has several limitations. First, the measures of FN, pain and PATGL were not from an MDHAQ; hence, the term ‘RAPID3-like’. However, various measures of FN and pain are correlated at high levels in the same patient on the same day; HAQ-S is highly correlated with the original HAQ-DI (Spearman's correlation=0.96).35 In addition, three studies have documented high correlations of RAPID3 from an MDHAQ with BASDAI at levels (r=0.7–0.8; p<0.001).18–21 Second, to evaluate discrimination of disease activity, we included only patients with inactive or active disease according to the patient and physician assessments, which may limit the interpretability of our findings in patients with intermediate levels of disease activity. Third, indices that include patient measures are not strictly activity measures. Measures of disease activity are important, but in a sense surrogates for patient status. In RA clinical trials, RAPID3 distinguishes active from control treatments as efficiently as swollen joint-counts and at considerably higher levels than tender joint-counts and laboratory tests.46 Furthermore, patient function is more significant to predict work disability and mortality in RA than swollen joints or acute phase reactants.10
In summary, we have found that a simple composite RAPID3-like score, which includes only three patient measures, appears valid, reliable and responsive to change in patients with Ax-SpA. This simple measure provides similar results in comparison to BASDAI and ASDAS-CRP and also has the advantage of being applicable to all patients regardless of diagnosis, as well as patients in whom a diagnosis is not established. MDHAQ/RAPID3 may provide a feasible approach to quantitative assessment of all patients in busy rheumatology clinical settings.
Acknowledgments
The authors thank the regional participating centres: Professor André Kahan (Paris-Cochin A), Professor Olivier Meyer (Paris-Bichat), Professor Pierre Bourgeois (Paris-La Pitié-Salpétrière), Professor Francis Berenbaum (Paris-Saint Antoine), Professor Pascal Claudepierre (Créteil), Professor Maxime Breban (Boulogne-Billancourt), Dr Bernadette Saint-Marcoux (Aulnaysous-Bois), Professor Philippe Goupille (Tours), Professor ean-Francis Maillefert (Dijon), Dr Xavier Puéchal (Le Mans), Professor Bernard Combe (Montpellier), Professor Liana Euller-Ziegler (Nice), Professor Pascal Richette (Paris-Lariboisière), Professor Pierre Lafforgue (Marseille), Dr Patrick Boumier (Amiens), Professor Jean-Michel Ristori (Clermont-Ferrand), Dr Nadia Mehsen (Bordeaux), Professor Damien Loeuille (Nancy), Professor René-Marc Flipo (Lille), Professor Alain Saraux (Brest), Professor Corine Miceli (Le Kremlin-Bicêtre), Professor Alain Cantagrel (Toulouse) and Professor Olivier Vittecoq (Rouen).
References
Footnotes
Contributors IC, TP and MD contributed to the study conception and design. DW and MD contributed to the acquisition of the data. IC and TP contributed to the analysis and interpretation of data. All co-authors participated in the manuscript drafting, revision and approved the final version.
Funding The DESIR cohort is conducted as a Programme Hospitalier de Recherche Clinique (PHRC) with Assistance Publique—Hôpitaux de Paris as the sponsor and it is also under the umbrella of the French Society of Rheumatology. An unrestricted grant from Pfizer has been allocated for the first 5 years. The work presented in this manuscript was supported by internal funding of TP.
Competing interests TP is a president of Health Report Services, which owns a copyright for a trademark MDHAQ/RAPID3. No license is needed for clinicians who may freely use MDHAQ/RAPID3 to monitor patient status in usual clinical care. Royalties and license fee are received from for-profit pharmaceutical and electronic medical record companies for the use of MDHAQ/RAPID3, all of which are transferred to medical schools for further development of quantitative measurement in clinical rheumatology care.
Patient consent Obtained.
Ethics approval http://lacohortedesir.fr.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.