Article Text

Abstract
Objective To assess the influence of disease activity of patients with rheumatoid arthritis on treatment choices of rheumatologists in countries with restricted access to expensive, innovative drugs.
Methods Rheumatologists from Hungary, Romania and UK were invited to complete two consecutive discrete choice experiments with hypothetical drug treatments for two different patient profiles: high and moderate disease activity. Rheumatologists were asked to choose repeatedly between two unlabelled treatment options that differed in five attributes: efficacy (expected improvement and achieved disease activity state), safety (probability of serious adverse events), patient's preference (level of agreement), total medication costs and cost-effectiveness. A heteroscedastic discrete choice model using interaction terms between attribute levels and patient profiles (binary variable) was used to assess the preferences of rheumatologists towards each attribute and the influence of the patient profile.
Results Overall, 148 rheumatologists completed the survey (46% females, mean age 49 years, 49% academic). For both patient profiles, efficacy dominated the treatment choice over patient's preference, safety and economic aspects. However, for patients with high compared with moderate disease activity, the importance of drug efficacy significantly increased (from 48% for moderate to 57% for high disease activity), whereas the importance of patient's preference significantly decreased (from 15% to 11%). No significant differences were observed for economic and safety considerations.
Conclusion Rheumatologists were willing to give up some efficacy to account for patient's preference when choosing treatments for patients with moderate compared to high disease activity. Disease activity however did not influence importance of economic aspects in treatment choices.
- physician's attitude
- DMARDs (biologic)
- patient perspective
- economic evaluation
- rheumatoid arthritis
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Drug efficacy drives treatment choices in patents with active rheumatoid arthritis, independently of the level of disease activity.
What does this study add?
With decreasing disease activity, shared decision making becomes increasingly important in rheumatologists' treatment decisions.
How might this impact on clinical practice?
Rheumatologists remain similarly conscious of economic consequences in their choice, irrespective of patient's disease status.
Introduction
Latest treatment recommendations for patients with rheumatoid arthritis (RA) suggest that treatment of patients with RA should aim to lower disease activity and should target remission in every patient. Initial treatment should include conventional synthetic disease modifying anti-rheumatic drugs (csDMARDs). When the treatment target cannot be achieved and disease remains at least moderately active despite csDMARDs (with or without steroids), addition of a biologic DMARD should be considered.1
It has been widely acknowledged that complexity of clinical decision making increased enormously. While exploding healthcare costs call for cost-effective treatment choices, the philosophy of patient centredness and shared decision making has been widely advocated as approach that improves health outcomes.2–4 However, cost constraints may frequently come at the expense of patient's preference and even may compromise freedom of choice towards more efficacious drugs, thus posing a great challenge to doctors.5 6
The drivers of rheumatologists’ treatment decisions are intriguing but still little is known about this topic and insight is needed into how rheumatologists value different aspects such as costs, cost-effectiveness (CE) or patient’s preferences when making treatment decisions. Recent studies revealed that across countries and independent of sociodemographic background rheumatologists balance different characteristics of a drug treatment7 8 when choosing treatments for their patients with RA. Drug efficacy clearly dominated the treatment choices, while clinicians were increasingly willing to consider economic implications as well as patients' preferences (in particular when patients expressed their dislike). However, it is not known to what extent the level of disease activity influences preferences in the treatment choice.
Reimbursement and budget restrictions experienced in daily clinical care may contribute to treatment benefits and costs. Especially in countries where access to expensive drugs is more restricted, rheumatologists might more consciously trade-off different drug treatment characteristics.
This study therefore aimed to investigate how the patient's disease status influenced the personal attitude of rheumatologists towards the different drug characteristics and how the importance of these characteristics changed when facing a different patient's disease profile.
Methods
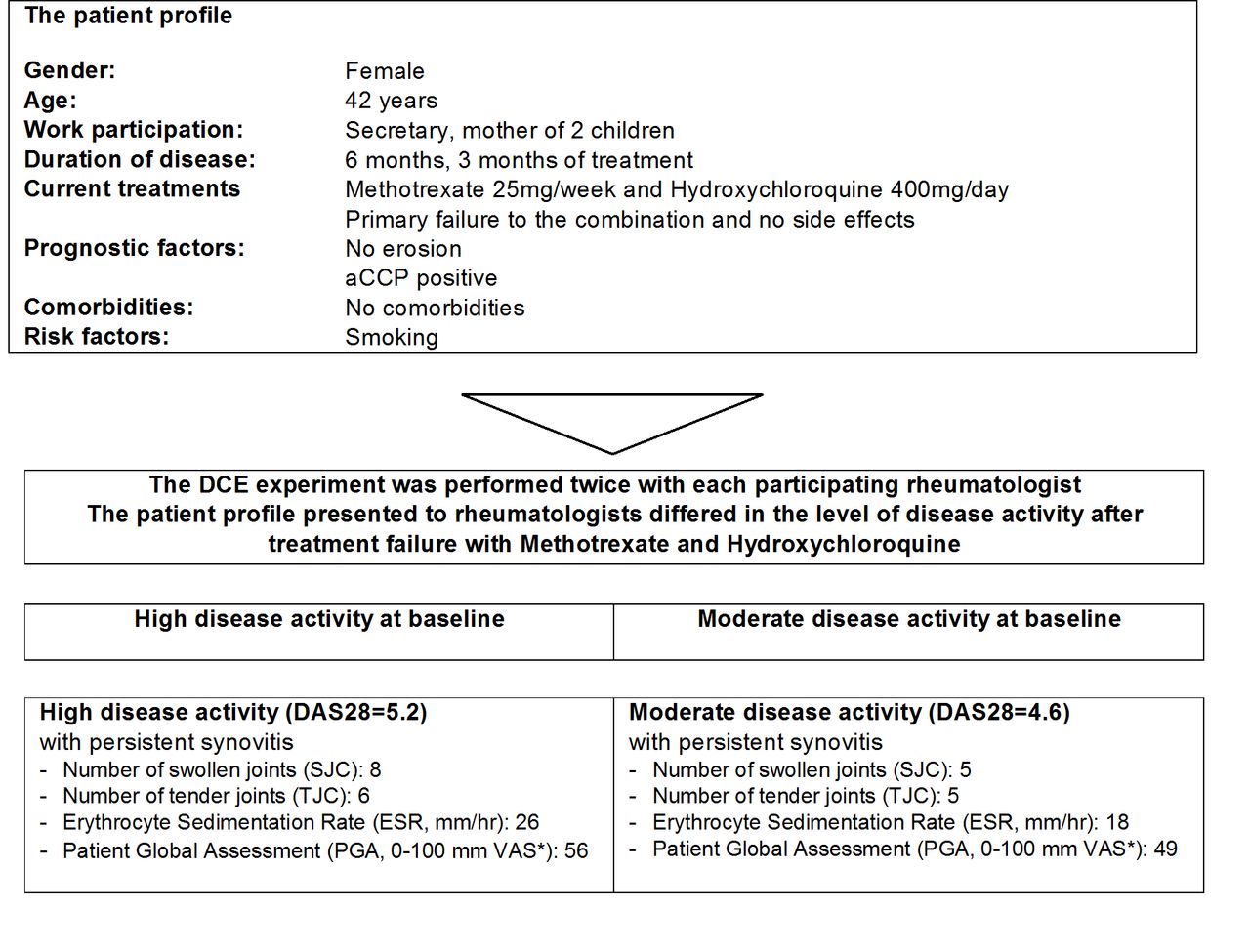
A discrete choice experiment (DCE) among rheumatologists was designed to assess the relative importance of different drug characteristics when selecting a drug treatment for a patient with RA. A DCE is based on the assumption that interventions can be described by characteristics (attributes) and corresponding attribute levels. In our study, rheumatologists from three countries with access to innovative, expensive antirheumatic drugs restricted to patients with high disease activity, were asked to select the preferred drug treatment in a series of choices that contained two hypothetical treatment options (A and B). Each treatment was described by a set of attributes and levels.9 To understand how the patient's disease characteristics would influence treatment choices, the DCE was repeated for two patient profiles, differing in the level of disease activity (figure 1).

The patient profiles presented to rheumatologists in the discrete choice experiment (DCE). aCCP, anti-cyclic citrullinated peptide; DAS28, 28-joint Disease Activity Score; VAS, visual analogue scale.
Data collection
Rheumatologists have been recruited from three countries that restrict access to expensive drug treatments to patients with high disease activity (28-joint Disease Activity Score (DAS28)>5.1) and participated in the international study8 (Hungary (HU), Romania (RO) and United Kingdom (UK)).
From October 2014 until May 2015, certified and clinically active rheumatologists were invited to participate in this study. An anonymous online survey was distributed by email through a national principle investigator (PI) per country. PIs were requested to invite at least 150 rheumatologists per country applying different approaches (convenience sampling, systematic involvement of societies, snowball sampling techniques).
The patient profiles
Both profiles were developed together with clinical rheumatologists (n=8). The smoking female patient with RA was diagnosed 6 months ago, and was anti-cyclic citrullinated peptide positive but non-erosive. She continued to have active disease despite two csDMARDs. In the first profile, the patient had moderate disease activity defined as a DAS28 of 4.6, while in the second profile the patient had high disease activity with a DAS28 of 5.2. Both profiles indicated a need for treatment change when following international treatment recommendations.
Design of discrete choice task and experiment
In a DCE, careful selection of attributes and their levels is essential to obtain valid results.10 In this study, a stepwise approach was followed that emphasised that patient's preferences and the economic attributes of treatment had to be included to meet the study objectives. First, potentially important attributes, attribute definitions and levels related to choosing RA treatments were identified from the literature. Second, a consensus meeting with an expert group (n=6) consisting of rheumatologists and methodologists in the field of economic evaluations, DCE and decision making was performed to agree on an initial list of attributes. Third, the proposed candidate attributes/definitions/levels were further discussed with rheumatologists (n=8) that were not involved in previous steps to ensure that they reflected clinical realities.
In summary, treatment options were characterised by five characteristics, each specified by three levels: expected treatment efficacy (level of improvement and achieved state of disease activity), safety (probability of a serious adverse event (AE)), patient's preference (level of agreement with proposed treatment), total medication costs and CE (incremental cost-effectiveness ratio (ICER)). An overview of final attributes, levels and level descriptions can be found in table 1.
Attributes and levels describing drug treatment options in the DCE experiment
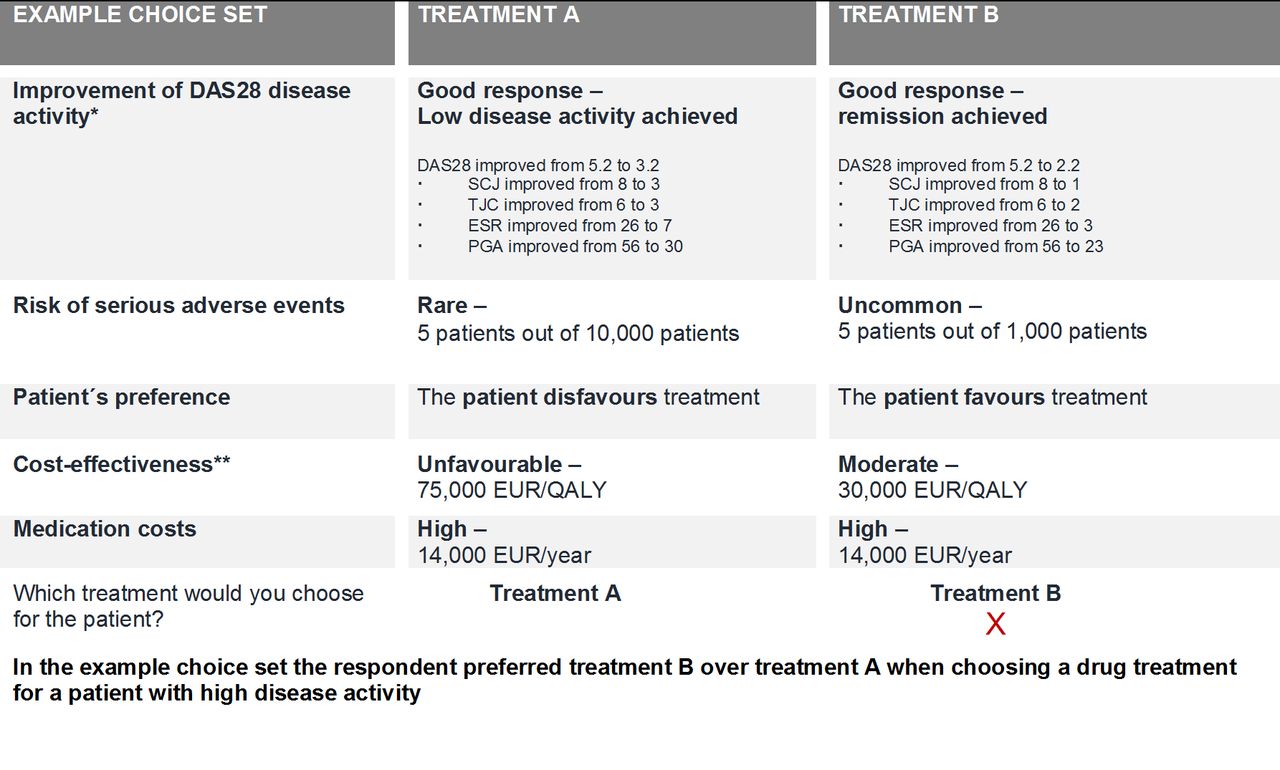
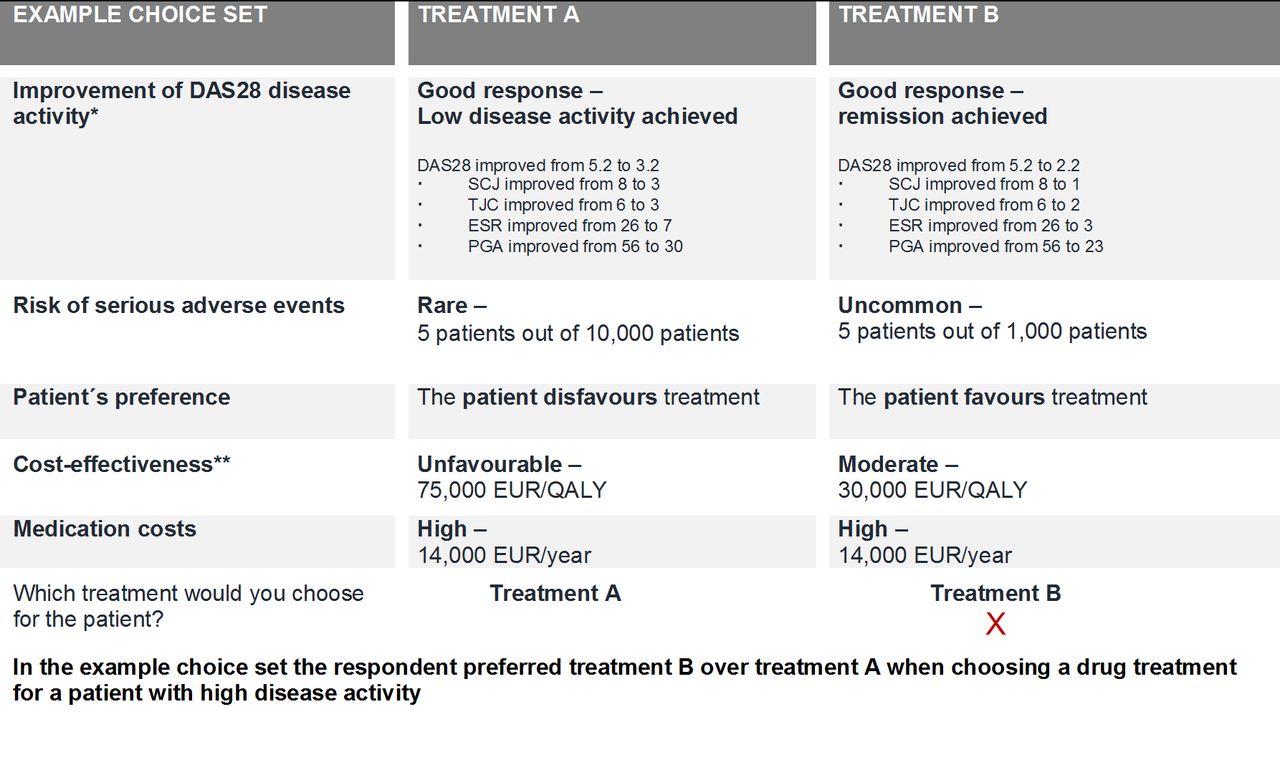
To increase the response rate and/or improve response reliability,11 the number of choice sets in the DCE had to be limited.12 A Bayesian efficient experimental design was applied, resulting in 14 choice sets per patient profile (Ngene software13). A Bayesian design maximises precision of estimated parameters for a given number of choice questions,9 by incorporating a priori information about the sign and value of parameters. A pilot DCE experiment with 10 rheumatologists was performed to generate the a priori information. Furthermore, to avoid presenting respondents with implausible treatment options, the experimental design was restricted to realistic combinations between efficacy, costs and CE (eg, within a choice option, a treatment with highest efficacy levels and lowest cost levels could not be allocated to the worst CE level). A dominance test (a choice set with one treatment option clearly dominating the other to ensure that treatment options were carefully reviewed by respondents) and two re-test choice sets (repetition of a choice set to assess test-retest reliability) were integrated in the final design. An example of a choice set is shown in figure 2.
{kind=link}
{kind=link}
Example choice set: DAS28, 28 joint disease activity score; EUR, Euro; QALY, quality-adjusted life year. * In the choice sets, changes of the individual DAS28 components (tender joint count (TJC), swollen joint count (SJC), erythrocyte sedimentation rate (ESR), patient global assessment of disease activity (PGA)) were also presented. ** Cost-effectiveness in costs (Euro) per QALY gained for the selected treatment compared with usual care.
The questionnaire
The questionnaire had four parts, with the first part providing a description of the DCE task followed by an explanation of attributes and levels and a description of the patient profiles (figure 1). The second and third part contained both DCE experiments (for two different patient profiles, respectively). The last part of the survey collected sociodemographic background information of respondents to support interpretation of results. A pilot study of the survey was conducted among rheumatologists (n=14) before dissemination of the final questionnaire. The online questionnaire was distributed using Qualtrics.14
Statistical analysis
Responses were considered for data analysis when both DCE tasks were completed and participants successfully passed the dominance test (a choice set in which one option clearly outweighs the other option).
A (utility) model was constructed with the observable relative rheumatologists' treatment preference (utility U) of rheumatologist (i) for a treatment choice (j) defined as a sum of preference scores for characteristics’ levels:
Uij = β0 + β1Good response + β2Remission + β3Rare AE + β4Uncommon AE + β5Favoured by patient + β6Disfavoured by patient + β7Cost-effectiveness + β8Costs
where β0 is the constant and β1-8 are the mean attribute utility weights (rheumatologists' preferences) for the respective attribute. A positive significant coefficient, β, means that the respective attribute levels significantly increase overall treatment preference (utility). This is, for example, expected for treatment efficacy (both levels) or patient's agreement with a drug treatment option. A negative significant coefficient, β, in contrast means that the respective attribute level decreases the treatment preference, which is for safety (both levels), a patient's disagreement with a drug as well as increased costs. A possible non-linear relationship between attributes has been ruled out using interaction studies. The findings are in line with what was assumed in other DCEs that investigate economic considerations and/or patient's preferences in treatment choices.15 16 Of note, cost and CE were presented as discrete levels in the experiments, they were coded as continuous variables in the model with a linear specification providing a better model fit.17 18
To investigate differences in treatment preferences between patient profiles, a heteroscedastic extreme value (HEV) model was selected (Nlogit V. 5).19 The HEV model took into account scale heterogeneity between countries, while assuming that the errors were identical across alternatives (profiles) and individuals (rheumatologists). A heteroscedastic discrete choice model using interaction terms between attribute levels and patient profiles (binary variable) was used to assess the attitude of rheumatologists towards each attribute and the influence of the patient profile. In the heteroscedastic model, a significant interaction reveals significant differences in rheumatologists' treatment preferences for a certain characteristics across the two patient profiles.20
Finally, the relative importance of the characteristics for each profile was estimated. The relative importance weights were calculated using the method described by Malhotra and Birks,21 by dividing the range of the level coefficients for one attribute by the sum of ranges of all attributes. Of note, for categorical variables the range is derived between the lowest and the highest level value.
Results
Overall, 148 rheumatologists from three countries—HU (n=71), RO (n=42), UK (n=35)— completed the DCE and were included in the analysis. None of the respondents that completed both DCE tasks failed the dominance test. Mean age of participants was 49(SD 11) years, 46% being female. Forty-nine per cent of respondents worked in an academic setting. Further details can be found in table 2.
Rheumatologists' characteristics
Rheumatologists´ preferences for a treatment choice for a patient with moderate and high disease activity.
Interactions between patient profile and efficacy (both levels) as well as between profile and patients’ disagreement with treatment were significant (p<0.05). Table 3 presents the analyses for both patient profiles.
Rheumatologist's preferences for a treatment choice in a patient with moderate and high disease activity
Efficacy had the strongest contribution to the treatment choice independent of the patient profile. However, the relevance of efficacy somewhat decreased in the treatment choice when changing the profile from high (βGood response=1.97, βRemission=3.25) to moderate disease activity (βGood response= 1.57 βRemission=2.77). The relative importance of efficacy decreased accordingly from 57% for patients with high disease activity to 48% for patients with moderate disease activity. The decrease in rheumatologists' treatment preference was seen for both efficacy levels. In contrast, the relative importance of patients’ preference increased from 11% when choosing a treatment for a patient with high disease activity to 15% for patients with moderate disease activity. Specifically, the interaction revealed that rheumatologists consider a patient's dislike significantly more in treatment decisions for patients with moderate disease activity (compared with patients with high disease activity).
Economic and safety considerations played a relevant role with higher economic burden and increasing safety risks decreasing treatment preferences (table 3). However, no significant interactions were found between profiles for the economic attributes—absolute costs and relative CE—and safety (both levels) indicating that differences between profiles were not significant.
Discussion
Independent of the patient's disease severity, expected drug efficacy clearly dominated treatment choices when rheumatologists were faced with a treatment adjustment. However, for patients with moderate disease activity, efficacy became somewhat less important, when compared with drug choices for patients with high disease activity. This probably emphasises the urgency recognised by rheumatologists in efficaciously suppressing inflammation, particularly in the presence of high disease activity. On the other hand, patient's preference became more influential when the disease activity was less severe. Rheumatologists, however, remained equally conscious of cost and CE of drug treatments, irrespective of the patient's disease activity.
The dominating role of efficacy in treatment choices confirmed the findings of earlier studies.7 8 Interestingly, the attitude towards economic attributes did not change significantly when changing the patient's disease status. Rheumatologists included in the DCE experience stringent clinical criteria for costly drug treatment choices in clinical practice. In their countries, access to expensive innovative drugs is mostly limited to patients with high disease activity (ie, only one of the presented patient profiles). The DCE however presented hypothetical scenarios and asked clinicians to make personal, scientific trade-offs irrespective of limitations in clinical practice. The findings indicate that rheumatologists remain conscious of costs but feel higher treatment costs are justified for patients with high and moderate disease activity to help patients reach low disease activity or remission as proposed in scientific guidelines. In other words, rheumatologists target remission in RA, with its known benefits, rather than focus on cost issues and be satisfied with a moderate disease activity level. Of note, although CE provides more valuable information on the efficient use of healthcare resources, rheumatologists are still strongly focused on absolute costs when making economic trade-offs.
We have chosen to perform the experiment in European countries with restricted access to expensive innovative drugs that do not allow prescription of these drugs to patients with moderate disease activity, as recommended in the European League against Rheumatism recommendations.1 22 It was considered these rheumatologists make more conscious choices among all the attributes, and were therefore of special interest for this experiment although this selection might limit generalisability. However, when comparing rheumatologists' attitudes towards economic implications, no systematic differences could be observed between countries with high and low access to expensive drugs,8
The role of patients' preference in treatment decisions of clinicians was summarised in recent reviews on shared decision making.23 24 It was found that clinicians primarily support the concept of shared decision making in situations where multiple comparable treatment options exist, although they tend to propose a treatment rather than share decisions in situations where one option clearly outweighs the alternatives or in cases of acute treatment needs.
In this line, our findings may indicate that the extent to which patients' preferences are considered in treatment choices depends on the 'perceived' urgency. Persisting high disease activity and previous treatment failures may imply such an urgent need to change treatment, especially when available alternatives are limited.
Of note, an increasing number of DCEs investigated treatment preferences among physicians. A number of these DCEs were discussed in a recent review by Clark et al.25 Although the majority of DCEs systematically selected characteristics and levels, only a few clearly specified the selection of the patient profile. With this study, we could show that seemingly small adjustments in the patient profile can have an influence on the DCE results. Ideally, a clear definition of the patient profile for whom the clinician is making treatment decisions should become a routine part in the development of a DCE.
The study has some limitations. First, although the respondents represented the entire spectrum of age, work environment from each included country and experience we cannot exclude selection bias and generalisability of results. Second, the DCE has some inherent limitations including the number of characteristics used to describe the treatment options is limited and may not fully reflect the complexity of a treatment decision in reality (eg, multiple factors can influence the assessment of a drug's benefits, risks and the personal patient preference). Third, presenting two economic attributes—costs and CE—in the DCE has its limitations as also absolute costs together with efficacy and safety provide insights into CE of a drug. However, it is important to understand that DAS28 response, rate of rare but severe side effects and direct drug costs are not equivalent to cost-utility, and therefore cost-utility and overall costs were included. Also, caution was taken in the generation of the choice tasks and implausible combinations between attributes efficacy, safety and costs were removed from the choice sets to ensure that respondents were not confronted with unrealistic treatment options. Only including both economic attributes (drug costs and CE) allowed to raise awareness on the fact that clinicians are still predominantly focused on absolute costs despite relative CE being more informative to assess the value of a treatment. Fourth, by repeating the DCE with two different patient profile it cannot be completely ruled out that an increase in fatigue possibly influenced preferences (in particular, the latter profile—high disease activity). However, present literature indicates that important systematic differences are unlikely.26 Finally, we asked rheumatologists to state preferences to a hypothetical scenario. This showed that they trade-off various aspects; however, it remains unknown whether they reach decisions in the same way in clinical practice.27
Our study revealed that in countries with substantial economic restrictions for prescription of costly RA treatments, rheumatologists were willing to give up some efficacy to account for patients' preference when choosing treatments for patients with RA with moderate compared with high disease activity. Disease activity, however, did not influence the importance of economic aspects in treatment choices indicating that in line with present treatment recommendations rheumatologists consider higher treatment costs equally justified for patients with high and moderate disease activity.
Acknowledgments
The authors would like to thankall participating rheumatologists for their contribution to the study and theclinical rheumatologists for their support in the study design andquestionnaire development: Tubergen van, AM; Vosse D; Linden van der JMJP;Onna van MGB; Walravens MJF; Saritas AM; Schoonbrood T.H.M; BoursSPG; Denissen ECM; Spaetgens B; Essers IMM; Stolwijk C; Antoaneta I., S Dadoune, S.Rozenberg, Molto, A. Further the authors would like tothank the Romanian Societyof Rheumatology for their support in the study coordination.
References
Footnotes
Contributors MH contributed to conception and design of the study, performed the statistical analyses, contributed to the interpretation of results and drafted the manuscript. MH contributed to conception and design of the study, supervised the performance of the statistical analyses and contributed to data interpretation and manuscript writing. SR contributed to conception and design of the study, the interpretation of results and manuscript writing. VW contributed to conception and design of the study, statistical analyses and interpretation of results and reviewed the manuscript. FB, MP and AK contributed to conception and design of the study, were responsible for recruitment of rheumatologists as principle investigator in their country, contributed to the interpretation of results and reviewed the manuscript. JLS and BF contributed to conception and design of the study and reviewed the manuscript. AB supervised the study including conception and design, data analysis, interpretation and manuscript writing. All authors read, critically reviewed and approved the final version of the manuscript submitted for publication.
Competing interests MH contributed during an unpaid extended maternity leave (2013-2016) agreed with Hexal AG, Germany. Related to the topic of this study, all other co-authors have no disclosures to declare.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.