Article Text

Abstract
Objectives The aim of this paper was to analyse the impact of obesity, in addition to known predictors, on disease outcome in early rheumatoid arthritis (RA).
Methods Body mass index (BMI) was available in 260 patients from the Swedish pharmacotherapy trial (SWEFOT). Differences in disease activity (DAS28), functional impairment (HAQ), pain (Visual Analogue Scale, VAS-pain) and radiographic damage were evaluated over 24 months between BMI categories (obese BMI >30, n=43; overweight BMI=25–29.9, n=74; normal BMI <25, n=143) using non-parametric testing. Predictors of European League Against Rheumatism non-remission (DAS28 ≥2.6) at 24 months of follow-up were evaluated using binary univariate and multivariate logistic regression.
Results Obesity at baseline was associated with worse continuous-scale clinical outcomes over 24 months (DAS28, HAQ and VAS-pain at last visit: obese vs normal: p<0.001; obese vs overweight: p<0.05). Furthermore, obese patients compared with non-obese patients had significantly greater odds of non-remission at 24 months (adjusted OR (aOR) 5.2; 95% CI 1.8 to 15.2). Other independent predictors were female sex (aOR 2.6; 95% CI 1.1 to 5.8), current smoking (aOR 2.6; 95% CI 1.1 to 6.3) and HAQ (per-unit increase, aOR 1.9; 95% CI 1.1 to 3.4). The pattern was similar among seropositive and seronegative patients; and in the subgroups of methotrexate responders and patients randomised at 3 months to add-on of sulfasalazine+hydroxychloroquine, although not significant with add-on of infliximab. Obesity had no independent association to radiographic progression.
Conclusions In this early RA trial reflecting today’s standard treatment, obesity, in addition to sex, smoking and functional impairment strongly lowered the chance of attaining good clinical outcomes, including remission, today’s treatment goal. This highlights the importance of considering lifestyle modification as one of the cornerstones of RA care.
Trial registration number NCT00764725; Post-results. WHO database at the Karolinska University Hospital: CT20080004.
- early rheumatoid arthritis
- disease activity
- DMARDs (synthetic)
- anti-TNF
- treatment
- body mass index
- predictions and projections
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- early rheumatoid arthritis
- disease activity
- DMARDs (synthetic)
- anti-TNF
- treatment
- body mass index
- predictions and projections
Key messages
What is already known about this subject?
In rheumatoid arthritis (RA), obesity has been associated with worse clinical but not radiographic outcomes. However, there are only limited data from early disease and from randomised clinical trials in the context of specific treatments. Furthermore, it is not clear whether known predictors of outcome might explain this association.
What does this study add?
In this early RA trial reflecting today’s standard treatment (methotrexate with add-on of anti-tumour necrosis factor or triple therapy in non-responders), obesity strongly lowered the chance of attaining good clinical outcomes, including remission.
Other independent predictors of non-remission were female sex, current smoking and functional impairment.
How might this impact on clinical practice?
These findings show that manifold differences in the likelihood of remission can be predicted using measures that are easily available in the clinic at diagnosis and highlight the importance of considering lifestyle modifications as one of the cornerstones of RA care.
Introduction
Despite important therapeutic improvements of the inflammatory control of patients with rheumatoid arthritis (RA), two-thirds of patients do not respond to first-line treatments and are at increased risk of functional impairment, work disability and decreased health-related quality of life.1–4 Thus, it is important to identify useful clinical predictors of outcome in early disease.
In RA, obesity or overweight (body mass index (BMI) ≥30 or 25–29.9 kg/m2, respectively) have been associated with worse outcomes, including a lowered likelihood of achieving good inflammatory and pain control and more functional impairment in observational studies.5–8 On the other hand, an elevated BMI has also been shown to be associated with somewhat less radiographic damage.5 9
However, there are only limited data from randomised clinical trials—especially in the context of specific treatment options, controlling for potential biases such as different dosage or treatment changes over time. Furthermore, it is not clear whether other known predictors of worse outcome or treatment response, such as female sex, current cigarette smoking habits, functional impairment or positive autoantibodies (anticitrullinated protein antibodies (ACPA) and/or rheumatoid factor (RF)) might explain this association.
Thus, the aim of this study was to examine if obesity can predict clinical disease activity or radiographic outcomes in a well-described early RA trial population reflecting standard treatment and to analyse obesity as a prognostic factor of outcomes for individual antirheumatic agents.
Methods
The SWEFOT trial
The Swedish Pharmacotherapy Trial (SWEFOT)10 11 was a 2-year open-label multicentre randomised clinical early RA trial where all patients first received methotrexate (MTX) monotherapy for 3 months. Patients achieving low disease activity (28-joint Disease Activity Score (DAS28) ≤3.2) remained on MTX, and non-responders were allocated either to triple therapy (TT: MTX, sulfasalazine, hydroxychloroquine) or to anti-tumour necrosis factor therapy (anti-TNF: MTX, infliximab). For this current study, SWEFOT patients were included if they had available baseline BMI, which was subdivided into normal (<25), overweight (25–29.9) or obese (≥30) categories. Core set measures including DAS28, the Health Assessment Questionnaire (HAQ), Visual Analogue Scale (VAS) for pain, radiographic damage (Sharp-van der Heijde Score (SHS)) and other clinical outcome measures (VAS-global; tender and swollen joints; C reactive protein; erythrocyte sedimentation rate (ESR)) were evaluated over 24 months, including the 3–24 months European League Against Rheumatism (EULAR) good response. DAS28 and other clinical outcome measures were available at baseline, 3, 6, 9, 12, 18 and 24 months; and SHS was available at baseline, 12 and 24 months. Clinical non-remission (DAS28 ≥2.6) at 24 months was the primary outcome measure, and analyses were performed based on an intention-to-treat approach.
SWEFOT was approved by the national health authorities/ethics committees at all including sites and was conducted in accordance to the Declaration of Helsinki. Written, informed consent was obtained from all patients prior to study inclusion. Trial registration: ClinicalTrials.gov (NCT00764725); WHO database at the Karolinska University Hospital: CT20080004.
Statistical analyses
The Mann-Whitney U test and Kruskal-Wallis test with Dunn-Bonferroni correction were performed for continuous scale measures, and Pearson’s χ2 or Fisher’s exact test were performed with proportional categorical measures. ORs with 95% CIs were calculated using univariate and multivariate binary logistic regression. Significant findings, in addition to parameters of known or potential predictive value for RA outcome (eg, seropositivity, symptom duration, age, smoking, functional impairment and sex), were kept in the multivariate model to adjust for potential confounding. All calculations were performed on IBM SPSS V.23.0. Two-tailed p values <0.05 were interpreted as significant.
Results
Patient characteristics
Of 487 initially enrolled individuals, 403 patients remained in the SWEFOT trial until 3 months of follow-up. Of these, 260 patients had available BMI at baseline (see online supplementary figure S1). No baseline characteristics differed among patients with available BMI included in the current analyses compared with the original SWEFOT population (table 1). Baseline characteristics of obese patients did not differ from overweight and normal-weight patients except that they were somewhat older (see online supplementary table S1).
Baseline characteristics of early DMARD-naive patients with RA participating in the SWEFOT trial
BMI categories and disease outcome during 24 months of follow-up
All patients
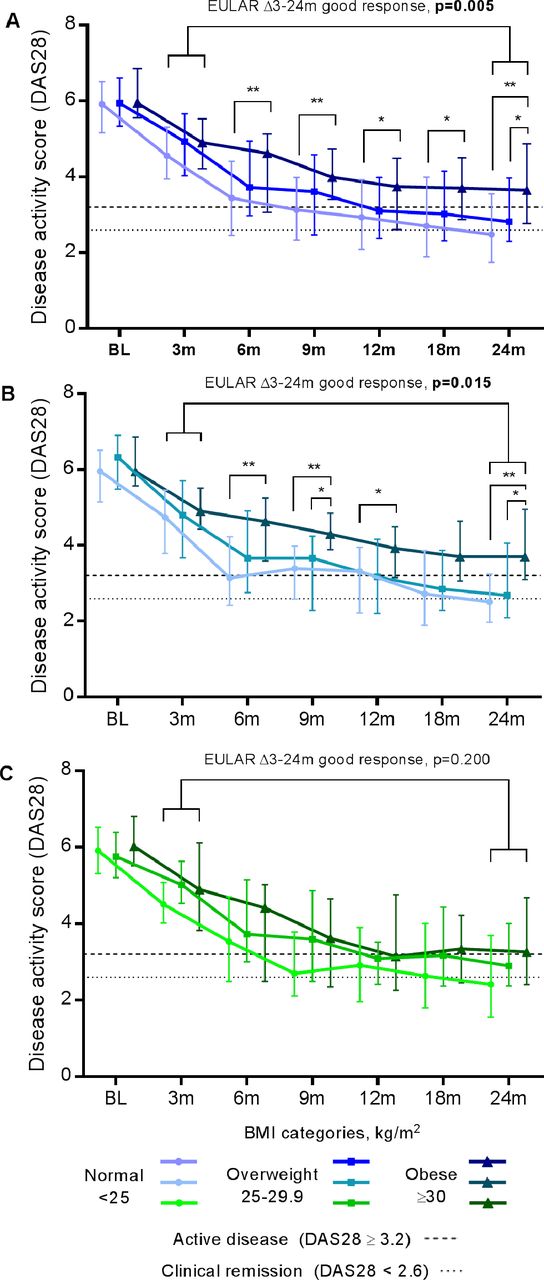
When clinical outcome measures were analysed on a continuous scale over 24 months (DAS28, HAQ, VAS-pain and ESR) stratified for BMI categories, there was a clear dose–response relationship observed, with better outcomes among normal and overweight compared with obese patients (figure 1). When the DAS28 components were analysed, a similar pattern was observed, except for the swollen joint count, although it should be noted that very few patients had remaining swollen joints at follow-up (figure 1 and supplementary figure S2). Furthermore, normal weight (58%, n=66/114) and overweight patients (50%, n=31/62) had a greater chance of attaining 24-month clinical remission (DAS28 <2.6) than obese patients (23%, n=9/39) (OR (95% CI) 4.6 (2.0 to 10.5); 3.3 (1.4 to 8.2), respectively). When non-obese were compared with obese patients (remission, 55% vs 23%, 4.1 (1.8–9.1), respectively), comparable differences were also observed for the 24-month EULAR good response (50% vs 31%, 2.3 (1.1 to 4.7)).

Changes in clinical outcome measures over 24 months on a continuous scale in the whole SWEFOT trial population with available baseline BMI categories. Mann-Whitney U tests were performed for all calculations. Medians and IQR are plotted for each BMI category. (A–D): DAS28, HAQ, VAS-pain and ESR, respectively, are plotted at BL; and at 3, 6, 9, 12, 18 and 24 months (m). BL, baseline; BMI, body mass index; SWEFOT, Swedish Pharmacotherapy Trial.
MTX monotherapy
Among the patients who achieved low disease activity and continued with MTX monotherapy, those who were obese had an overall worse outcome at 24 months of follow-up than non-obese patients, despite their initial response at 3 months. Thus, on a continuous scale, a trend was observed for DAS28 (median (IQR) 2.9 (2.6–3.1) vs 2.0 (1.6–2.8) units, p=0.062); and significant differences were observed for HAQ and VAS-pain (median (IQR) 0.63 (0.25–0.75) vs 0.25 (0–0.63) units, p=0.042; 30 (19–48) vs 11 (5–35) mm, p=0.048, respectively).
Randomised arms
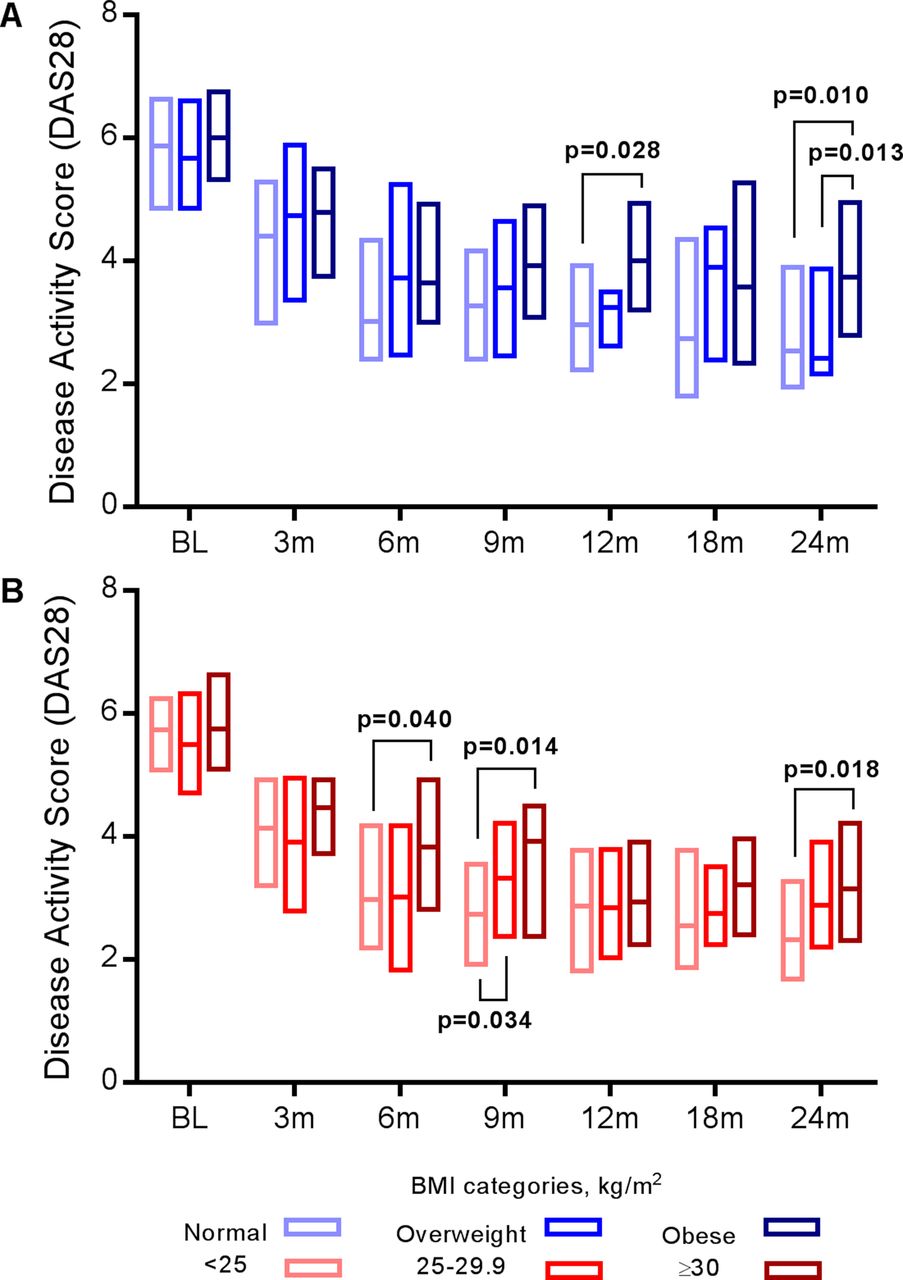
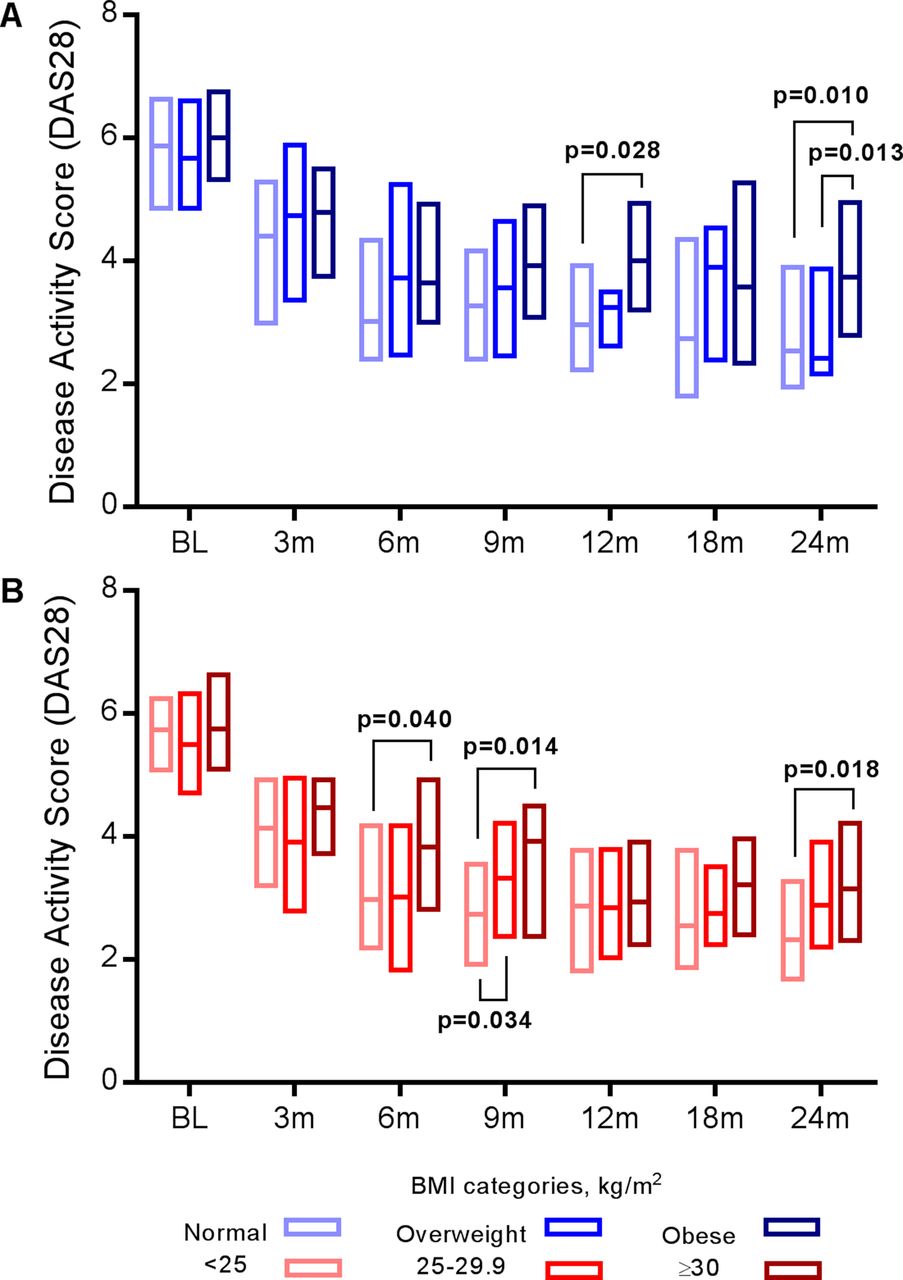
As shown in figure 2, a similar dose–response pattern was observed for BMI categories and DAS28 among all randomised patients (figure 2A), just as was seen for all patients, however, this dose–response relationship was significant only in the TT arm (figure 2B) and not for anti-TNF (figure 2C). Normal-weight patients more frequently achieved a EULAR good response at 24 months of follow-up (66% vs 38%, OR (95% CI) 3.2 (1.4 to 7.3)) than obese patients among all randomised patients, and this was also significant only in the TT arm (67% vs 35%, 3.9 (1.3 to 11.8)) but not for anti-TNF (64% vs 42%, 2.5 (0.69 to 9.0)). For other outcome measures, obese patients on TT, but not on anti-TNF, had significantly worse HAQ and VAS-pain over 24 months (data not shown).
Changes in clinical disease activity over 24 months on a continuous scale in SWEFOT trial participants randomised to triple therapy or anti-TNF with available baseline BMI categories. Patients not achieving low disease activity (DAS28 <3.2) at the 3-month follow-up visit were randomised, and the EULAR good response at 24 months of follow-up was calculated using randomisation at 3 months as the baseline value. Individual time points with DAS28 over 24 months are plotted with medians and IQR. Included among all patients (A) is the combination of the two randomised groups, triple therapy (B), n=94 or anti-TNF (C), n=91. Responders to methotrexate (DAS28 ≤3.2) continued on monotherapy and are not included due to non-randomisation. Sample size (n) for normal weight, overweight and obese in (A): 103, 48, 32; (B): 52, 22, 20; and (C): 53, 26, 12, respectively. Obese versus normal weight: *p<0.05; **p≤0.002. BMI, body mass index; EULAR, European League Against Rheumatism; m, months; SWEFOT, Swedish Pharmacotherapy Trial; TNF, tumour necrosis factor.
Already by 3 months after failing MTX (6 months after baseline), obese patients on anti-TNF achieved an equal remission (27%) to non-obese counterparts on anti-TNF (26%, supplementary figure S3). They also had a significantly better proportion of remission than obese patients assigned to TT, none of which reached remission—as opposed to several non-obese patients reaching remission on TT (28%). Obese patients on anti-TNF retained a significantly superior remission ratio at 9 months (33%) compared with obese patients on TT (0%), although some obese patients on TT improved after 12 months (15% remission). Remission at 24 months remained significantly more frequent among non-obese versus obese patients on TT (52%, 33/64 vs 15%, 3/20, OR (95% CI) 6.0 (1.6 to 22.6)), but a significant difference was not observed among anti-TNF counterparts (51%, 38/74 vs 33%, 4/12, 2.1 (0.59 to 7.6)). Consequently, remission at 24 months among non-obese patients either on TT or anti-TNF was identical.
Predictors of non-remission at 24 months
All patients
Variables that were significantly associated with non-remission (DAS28 ≥2.6) at 24 months were obesity, female sex, HAQ, DAS28 and tender joints (table 2). After ruling out collinear variables and including previously known predictors,12 the final multivariate model included obesity, female sex, current smoking and HAQ, as well as age. Obesity was found to be the strongest independent predictor of non-remission (adjusted OR (95% CI) 5.2 (1.8 to 15.2)). Other independent predictors were female sex, current smoking and HAQ (figure 3A, table 2). Using BMI as a continuous scale (per kg/m2 increase) also predicted non-remission (unadjusted OR (95% CI) 1.1 (1.1 to 1.2); adjusted OR 1.1 (1.0 to 1.2)).

Independent baseline predictors of non-remission at 24 months of follow-up in the SWEFOT trial population. (A) Adjusted ORs with 95% CIs for significant predictors in a binary logistic multivariate analysis of non-remission. Additional information can be found in table 2. (B) Risk matrices showing the likelihood (%) of non-remission with different combinations of predictors presented in (A). BMI and 24-month disease activity was available for 215 out of originally 403 SWEFOT trial participants. Of these, HAQ was available for 211 patients and smoking habits for 156 patients. Of those with HAQ and smoking habits (n=154), 26 were obese; 34, current smokers; 22, methotrexate responders; 65, randomised to triple therapy; 67, randomised to methotrexate+TNF inhibitor infliximab. HAQ, Health Assessment Questionnaire; NS, not significant; SWEFOT, Swedish Pharmacotherapy Trial; TNF, tumour necrosis factor.
Baseline predictors of non-remission at 24 months in the SWEFOT trial population with available BMI, ORs and 95% CIs
A risk matrix was created, illustrating the proportion of patients not achieving remission for different combinations of baseline predictors, ranging from the lowest for those lacking all predictors (<35%) to the highest among obese females (88%, figure 3B).
Individual therapies
When stratified into the three treatment groups, the power was limited due to smaller subsets, but a similar trend among the MTX responders was observed. Here, non-obese patients achieved numerically although non-significantly greater 24-month remission rates than obese patients (68%, 26/38, vs 29%, 2/7, unadjusted OR (95% CI) 5.4 (0.92 to 32.0); adjusted OR 3.6 (0.21 to 62.0)). The adjusted model required last observation carried forward LOCF, due to limited data for a full model in this subgroup.
Among patients on TT, obesity remained the only significant independent predictor of non-remission, while HAQ was the only significant independent predictor of non-remission in the anti-TNF arm (see online supplementary table S2; figure S4B,C, respectively).
BMI categories and radiographic progression
For radiographic damage (SHS) as a continuous measure, no significant differences were observed between BMI categories. When categorised using ΔSHS ≥1 point as cut-off value, radiographic progression from baseline to 24 months was less frequent among obese (44%, n=14/32) than non-obese patients (63%, n=108/172) (unadjusted OR (95% CI) 0.46 (0.22 to 0.99)), but this was not significant after adjustment for known predictors of radiographic progression; current smoking, disease duration, baseline erosions, HAQ and ESR,13 in addition to age (adjusted OR (95% CI) 0.37 (0.13 to 1.1)).
Stratification into ACPA positive and negative RA
Worse outcomes in obese patients remained after stratification into the main subsets of ACPA positive and negative RA (figure 4), and this was also evident in the TT arm, but no differences were observed in the anti-TNF arm—although it should be interpreted with caution due to limited numbers (see online supplementary figure S5).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Baseline BMI and disease activity over 24 months among SWEFOT trial participants: stratification by ACPA serostatus (A) ACPA-negative patients; (B) ACPA-positive patients. Normal weight, BMI<25 (A, n=43; B, 91); overweight, 25–29.9 (A, n=25; B, 45); obese, ≥30 (A, n=17; B, 23). Mann-Whitney U tests were performed for all calculations. Medians, IQR for each BMI category with DAS28 are plotted at BL; and at 3, 6, 9, 12, 18 and 24 months. ACPA, anticitrullinated protein antibody; BL, baseline; BMI, body mass index; m, months; SWEFOT, Swedish Pharmacotherapy Trial.
Using a 'last observation carried forward' approach or analysing only per-protocol completers who remained on their assigned therapy throughout the entire study did not modify the associations observed for obesity.
Discussion
In this early RA trial reflecting current standard treatment, obesity, in addition to known predictors, strongly lowered the chance of remission, today’s treatment goal. We demonstrated that the association of worse outcome with obesity was independent of female sex, current smoking and worse functional impairment at baseline. Obesity was the strongest independent predictor of non-remission, with more than a fivefold increased odds 2 years after diagnosis despite a treat-to-target approach initiatives in accordance with current guidelines. A persistent and dose-dependent association was observed for every clinical outcome measure captured at every follow-up visit; that is to say, a higher BMI category (obese>overweight>normal weight) was associated with a worse disease activity score, more functional impairment and more pain—thus validating, but extending previous clinical observations to the randomised setting.5–7 Whether obesity influences the outcome measures used—being to a large extent patient-reported in their nature—remains to be clarified, but the associations observed could not be explained by specific components of the DAS28 measure, with a similar pattern for all components except for the swollen joint count, where no significant associations were observed. However, very few patients had swollen joints at follow-up, so this observation should be interpreted with caution. An inverse, but not independent association between obesity and radiographic progression was observed in our study. Although not being independent from other predictors, our results indicate that obesity is associated with a clinically manifest yet non-erosive phenotype of RA. Stronger associations have been described in previous studies,5 9 and reasons for no significant association in our study can be the early RA setting with a low proportion of patients with progression.
To our knowledge, this is the first report indicating that obese patients with early RA respond differently to biological versus conventional disease-modifying anti-rheumatic drugs (DMARDs), where no significant differences were found for patients randomised to infliximab+MTX, in contrast to consistently worse outcomes for obese patients randomised to TT or a risk for worse long-term outcomes on monotherapy despite initial response to MTX. It is perhaps not surprising since infliximab doses are weight adjusted. However, previous reports with up to 1 year data on disease activity have yielded opposite results.14–16 In a report from the Italian GISEA network on RA, obesity was associated with non-remission to three different anti-TNF treatments.14 Here, obese patients who received infliximab had even worse outcomes than the other two anti-TNF agents, etanercept and adalimumab, which are not adjusted for weight. GISEA, however, was in an observational setting on established RA. Finally, an earlier non-randomised study with a small amount of patients found a worse 4-month response on infliximab if obese.15 However, our randomised results indicated—despite a 3–4 month MTX monotherapy non-response —statistically superior rates of remission directly after randomisation with 3 months of infliximab versus TT among obese patients. There are also findings from the BeSt four-armed randomised trial.17 18 Compared with SWEFOT,10 11 the glucocorticoid doses were higher, and steered treatment adjustments were applied every 3 months if remission was not achieved in the first three synthetic DMARD arms. The fourth arm, immediate infliximab+MTX, had dose elevations every 2 months on non-remission, up to a maximum of 10 mg/kg every 8 weeks (threefold higher dose than SWEFOT). In the post hoc study of BeSt, overweight/obesity was significantly associated with higher disease activity only in patients receiving infliximab after failure on several DMARDs.19 Among the other arms, overweight/obesity was significantly associated with worse outcomes on synthetic combination DMARDs. Thus, the findings in this intensive treatment approach are to an extent in accordance with our findings in a trial that may be closer to today's real-life care in several countries.
Although obese patients altogether had worse clinical outcomes, we demonstrated the value of analysing these outcomes individually by therapy in showing that infliximab with MTX led to non-significantly different outcomes in obese compared with non-obese patients, and that standardised-dose synthetic DMARDs are associated with inadequate treatment efficacy among obese individuals.
Although the current study was not designed to elucidate the potential mechanisms underlying the associations observed, there is substantial evidence available from basic studies about the connection between inflammation and adiposity. Macrophages are activated by free fatty acids, which are elevated in obesity due to the excessive amounts of adipose tissue.20 This also leads to more dead adipose tissue, creating a loop of chronic inflammation through consistent macrophage activation.21 Two biomarkers that could play a role in RA disease progression are adiponectin (inverse association with BMI) and leptin (positive association with BMI due to leptin insensitivity), which, in addition to TNF and interleukin 6, are both produced by white adipose tissue. Although additional studies are needed, both have been found to be potential stakeholders in RA—leptin in inflammation16 22 23 and adiponectin in bone erosions.16 24–26
It has recently been shown that MTX polyglutamates—the active metabolites which are associated with MTX efficacy— have an inverse association to BMI, and so was the frequency of hepatotoxicity, being observed in none of the obese patients, but in one-third of the patients in the lowest BMI category.27 It is possible that the lack of response to synthetic DMARDs is simply a question of dosage, since the associations with obesity were not observed for the anti-TNF arm but only for the TT and MTX responder arms. Infliximab is the only weight-adjusted TNF inhibitor, and future randomised trials therefore need to address whether or not similar responses can be achieved among obese patients with other TNF inhibitors. Notably, we are not aware of any studies investigating weight-adjusted MTX dosage in RA or other rheumatic diseases in adults, despite being done in juvenile forms as well as other indications for this treatment. Patients assigned to TT had a standardised dose and the only allowed increase was with sulfasalazine: from 1000 to 1500 mg twice daily. Thus, it is possible that obese patients on TT, including those with an initial MTX response who continued on monotherapy, required even higher doses to achieve effective responses.
Limitations and strengths
The main limitation in this study is its post hoc design, since the SWEFOT trial was not specifically designed to address the current questions pertaining to analysing clinically relevant predictors of specific treatment responses, such as lifestyle factors, for example, BMI or smoking status, where data were consequently not complete. However, there was no indication of selection bias in this subset. Furthermore, the size of the individual treatment groups does not allow us to draw firm conclusions pertaining to therapy response, especially for our findings concerning the infliximab arm due to a limited sample size. Additional studies investigating obesity as a predictor for response to specific therapies in early RA are thus required.
Obese patients were shown to have consistently worse disease activity, functional impairment and pain in all observations beyond diagnosis of early RA, and a clear dose–response relationship was observed with BMI categories in all core set outcomes. The strengths in this study are that we still observed this after taking into account other known clinical and lifestyle predictors; after performing sensitivity analyses (including LOCF, per protocol); and also finding similar patterns in both the seropositive and seronegative subsets of RA. At the same time, we analysed this within the treatment subgroups observing that this pattern was not significant for infliximab-treated obese patients.
To conclude, we found that obesity—a modifiable lifestyle factor—was associated with worse clinical outcomes over time, measured in disease activity (or its components), functional impairment and pain; but only a marginal inverse association was found for radiographic progression. Obesity at diagnosis was a strong and independent predictor of non-remission after 2 years of treatment according to current guidelines; the other significant predictors being female sex, current smoking and HAQ. When stratified into treatment groups, obesity was the only significant independent predictor of non-remission for MTX non-responders randomised to TT, but not if the weight-adjusted infliximab was added on to MTX. Thus, our findings confirm and yet extend previous findings, as it has now been performed in a well-defined trial-based clinical setting. Further studies are needed to explore whether this may be explained by the underlying biology, since TNF, which is secreted by adipose tissue and surrounding macrophages, could potentially pose as a more effective target than conventional DMARDs in the case of excessive adiposity; or it may be a question of dosage, since trials on weight-adjusted MTX treatment are, to our knowledge, lacking. Finally, these findings show that manifold differences in the likelihood of remission can be predicted using easily-available variables in the clinic at baseline and highlight the importance of taking both lifestyle and sex into account when conducting and reporting RA trials, as well as the importance of considering modification of lifestyle habits as one of the cornerstones of patient care in RA.
References
Footnotes
Contributors All authors meet the ICMJE guidelines for authorship and contributed equally to the design of the project, the discussion of the results and to the preparation of the manuscript. All authors read and approved the final version of the manuscript. AL conducted the statistical analyses, data management and preparation of the manuscript under the supervision of SS. KH and CL contributed to statistical analysis discussion and data management. KB and IH contributed with medical expertise in the project discussion. AL and SS created and finalised all graphical preparations. SS and RFvV were in charge of project supervision.
Competing interests AL, KB, IH, KH, CL and SS have no conflicts of interest to disclose; RFvV has received grants/research support from AbbVie, BMS, GSK, Pfizer, Roche and UCB—and has received consultancy fees from AbbVie, Biotest, BMS, Crescendo, GSK, Janssen, Lilly, Merck, Pfizer,Roche, UCB and Vertex outside the submitted work.
Ethics approval The regional Swedish ethics committees of all participating SWEFOT sites.
Provenance and peer review Not commissioned; externally peer reviewed.