Article Text

Abstract
Introduction We have limited data on the sustainability of tumour necrosis factor (TNF)-blocker tapering in rheumatoid arthritis (RA) in remission over the long term in real-life settings. This study aimed to assess the probability of sustained dose reduction of TNF-blockers in an observational 3-year extended follow-up of the Spacing of TNF-blocker injections in Rheumatoid ArthritiS Study (STRASS), a randomised controlled trial comparing progressive TNF-blocker injections (spacing arm (S-arm) to maintenance arm (M-arm)) in patients with RA in stable remission.
Methods In 2015, clinical data for the completer population were retrospectively collected at 1, 2 and 3 years after the end of the trial. The endpoints were the proportion of patients free of a biological disease-modifying antirheumatic drug (bDMARD) treatment, a sustainably spaced injection of TNF-blockers and a full-dose regimen as well as the mean dose of bDMARD intake and treatment switch rate.
Results Overall, 96 patients (76.8% of the completers) had data available up to 3 years; 11.5% discontinued TNF-blockers (5.8% vs 18.2% in the M-arm and S-arm, p=0.06), 30.2% had a tapered regimen (28.8% vs 31.8%, p=0.76) and 37.5% retained a full dose (44.2% vs 29.5%, p=0.14). The mean TNF-blocker dose quotient was 66% of the full dose (74% vs 58% in the M-arm and S-arm, p=0.06); 20.8% switched to another bDMARD (21.2% vs 20.5%, p=0.94).
Conclusion Sustained TNF-blocker de-escalation or withdrawal is achievable in 41% of patients over 3 years with limited dose reduction. Optimal strategies remain to be determined to maintain remission after TNF-blocker tapering or discontinuation.
- Anti-tnf
- Rheumatoid Arthritis
- Treatment
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Biological disease-modifying antirheumatic drug (bDMARD) discontinuation in rheumatoid arthritis (RA) in sustained remission is feasible but exposes to an increased risk of relapse.
Treatment tapering is associated with almost no structural damage progression if the Treat-To-Target (T2T) strategy is applied.
Most of the data are derived from randomised controlled trials of limited duration.
What does this study add?
This long-term follow-up study provides an insight into the management of RA in remission in a real-life setting.
The probability to achieve long-term drug-free remission remains low.
The average treatment reduction is between 25% and 40% of the initial dose regimen.
How might this impact on clinical practice?
bDMARD tapering in respect of the T2T paradigm seems a reliable strategy in everyday clinical practice.
Introduction
The launch of tumour necrosis factor (TNF)-blocker agents has deeply modified the management of rheumatoid arthritis (RA). These days, clinical remission or low disease activity (LDA) is a realistic objective achieved in a large proportion of patients.1 However, maintaining such treatments at full dose over the long term may not be necessary, and some authors have suggested that treatment should be reduced when disease activity becomes minimal or null.2 Moreover, biological disease-modifying antirheumatic drugs (bDMARDs) are associated with substantial costs and safety issues.
Several studies have tested discontinuation and dose-tapering strategies once clinical remission is achieved. Whatever the bDMARD considered, treatment discontinuation often led to disease relapse in most patients.3–8 Treatment tapering (dose reduction or injection spacing) seems feasible for a substantial proportion of patients with RA, although with a limited increased risk of structural damage progression.8–13 An 18-month clinical trial (Spacing of TNF-blocker injections in Rheumatoid ArthritiS Study (STRASS)) compared the effect of Disease Activity Score (DAS)-steered progressive spacing of TNF-blocker injections (spacing arm (S-arm)) to their maintenance (maintenance arm (M-arm)) for patients with established RA in sustained remission for more than 6 months.14 At the end of the study, in the S-arm, 39.1% had stopped the TNF-blocker, 35.9% had tapered the treatment and 20.3% maintained the full dose. Relapse was more common in the S-arm than the M-arm, but 79.6% of relapsers achieved remission or LDA again after TNF-blocker re-escalation. This finding suggests that such a tapering strategy is feasible but exposes patients to greater risk of relapse.
To date, we have only limited data on the feasibility and sustainability of tapering strategies in the longer term. For this reason, we conducted an observational 3-year extended follow-up of patients who participated in the STRASS trial. The main objectives of this study were to assess (1) the proportion of bDMARD-free patients, (2) the proportion of patients with spaced (but did not stop) injections of etanercept (ETA) or adalimumab (ADA), (3) the proportion of patients requiring full-dose regimen, (4) the mean bDMARD dose intake and (5) the treatment switch rate because of loss of efficacy or safety issues during follow-up.
Patients and methods
Study design
Details of the STRASS trial have been reported elsewhere14 and in online supplementary appendix. Briefly, 137 patients recruited in 23 French departments of rheumatology were randomly assigned between 2008 and 2011 to one of two strategies: S-arm (progressive spacing of TNF-blocker injections) or M-arm (maintenance of full-dose regimen) and followed up during 18 months. In the S-arm, the frequency of bDMARD injection was adjusted every 3 months on the basis of the DAS in 28 joints (DAS28),15 according to a prespecified algorithm. The STRASS trial population consisted of 137 adults with a diagnosis of RA according to the 1987 American College of Rheumatology classification criteria,16 who were receiving subcutaneous injections of ETA (n=74) or ADA (n=63). Patients needed to be in clinical remission according to the DAS2815 (ie, DAS28 ≤2.6) for at least 6 months to be included in STRASS. The study was approved by the ethics review board (CPP, Ile de France VI).
Supplementary file 1
Population
In the present study, all patients with RA (from both M-arm and S-arm) who completed the STRASS clinical trial were followed up and assessed by hospital-based or office-based rheumatologists who were completely free for therapeutic decision making. In 2015, physicians were contacted, and follow-up data were retrospectively collected from medical charts. The extended follow-up population corresponded to all patients in the STRASS population who completed the trial and continued to be followed up over the 3-year period.14 A non-opposition form (certifying that the patients did not express any opposition with retrospective data collection from his/her medical charts) was completed by the local investigator.
Data collection
A structured case report form was sent to all STRASS investigation centres between April and October 2015. Data collected from the medical charts were (1) swollen and tender joint counts, (2) patient global assessment of disease activity (Visual Analogue Scale) and physician global assessment of disease activity and treatment efficacy, (3) acute-phase reactants (erythrocyte sedimentation rate (ESR) and C reactive protein (CRP) level), (4) DAS28-ESR and DAS28-CRP, (5) structural damage progression (assessed by the physician as yes or no X-ray progression between the end of STRASS trial and the end of the follow-up) and (6) treatment regimen (drug name, dose and injection frequency) and reason for change in case of bDMARD discontinuation or switch. These data were collected for three different times: 1 year, 2 years and 3 years after the end of the trial (see online supplementary figure S1).
Supplementary file 2
Endpoints
The main endpoints of this extended follow-up study were as follows:
the proportion of bDMARD-free patients, defined as the number of patients who were able to discontinue ETA or ADA due to persistent remission at a given visit to the total number of patients with available data at the same visit;
the proportion of patients with tapered regimen, defined as the number of patients with spaced injection of ETA or ADA at a given visit to the total number of patients with available data at the same visit;
the proportion of patients with a full-dose regimen, defined as the number of patients who kept a full-dose regimen or required a return to a full-dose regimen due to RA relapse at a given visit to the total number of patients with available data at the same visit;
the mean dose quotient, defined as the ratio between the bDMARD dose regimen at 3 years and the labelled full-dose regimen, only for patients who kept their initial treatment;
the treatment switch rate because of loss of efficacy or safety issues.
Statistical analyses
Descriptive statistics are presented as mean±SD (95% CI) or number (%). The proportion of patients with spaced bDMARDs, no treatment or new treatment (if switch) was compared in each initial arm over the 3-year follow-up by χ2 test. The dose quotient in the two arms over 3 years was tested by the Wilcoxon test. This analysis involved all patients and the subgroup of patients who kept their initial treatment. The outcomes over 3 years of follow-up (mean DAS28, proportion of patients in LDA or remission and proportion of patients with structural damage) were compared in each arm by Student’s t-test. Survival curves were constructed for patients in the initial M-arm and for patients in the initial S-arm with effective spacing of TNF-blockers at the beginning of the follow-up. Relapse was defined as a switch or re-escalation of the TNF-blocker dose. There was no imputation of missing data except for survival curves (if the exact date of the switch or relapse was unknown, the median days between the two follow-ups were used). The predictors of relapse were explored by Cox proportional hazards models. Potential predictors were DAS28 score, rheumatoid factor, anticitrullinated peptide antibodies (ACPAs), CRP, initial randomisation arm disease duration and presence of erosions. If data for one treatment were missing but the following data were unchanged, patients were not considered in relapse. All statistical analysis involved use of R V.3.2.3 (R Corporation). p<0.05 was considered statistically significant.
Results
Extended follow-up study at baseline
Among the 125 patients of the STRASS completer population, 96 (76.8%) had data available 3 years later: 52/69 (75.4%) of the initial M-arm and 44/56 (78.6%) of the initial S-arm (figure 1). The main clinical and biological characteristics at the baseline extended follow-up are summarised in table 1. Briefly, the mean DAS28 was 2.4±1.2; 72 (75.0%) were in LDA or remission, 47 (48.9%) were taking ETA, 35 (36.5%) were taking ADA, 2 (2.1%) were taking bDMARD and 12 (12.5%) were bDMARD free. Among patients still on their initial TNF-blocker, 60/80 (75.0%)—100% from the M-arm and 30.0% from the S-arm—were under a full-dose regimen and 22/80 (27.5%)—all from the S-arm—a tapered regimen.

Flow chart of the STRASS RCT and the 3-year extension study. RCT, randomised controlled trial; STRASS, Spacing of TNF-blocker injections in Rheumatoid ArthritiS Study.
Patient characteristics at the end of the STRASS trial
Clinical outcomes at 3 years (ie, the end of the extended follow-up study)
The mean DAS28 at 3 years after the start of the extended follow-up was 2.6±1.3 (table 2) (2.7±1.4 and 2.6±1.2 in the initial M-arm and S-arm population, respectively, p=0.89). In total, 72.5% of the extended follow-up study population was in LDA or remission, with no difference between trial arms (72.1% and 73.0%, p=0.93). Only 43 patients had formal structural damage assessment at 3 years; among them, 13 (30.2%) had structural damage progression during the extended follow-up (25.0% and 36.8% in the initial M-arm and S-arm, p=0.54).
Patient outcomes after 3 years of follow-up
Treatment regimen evolution at 3 years
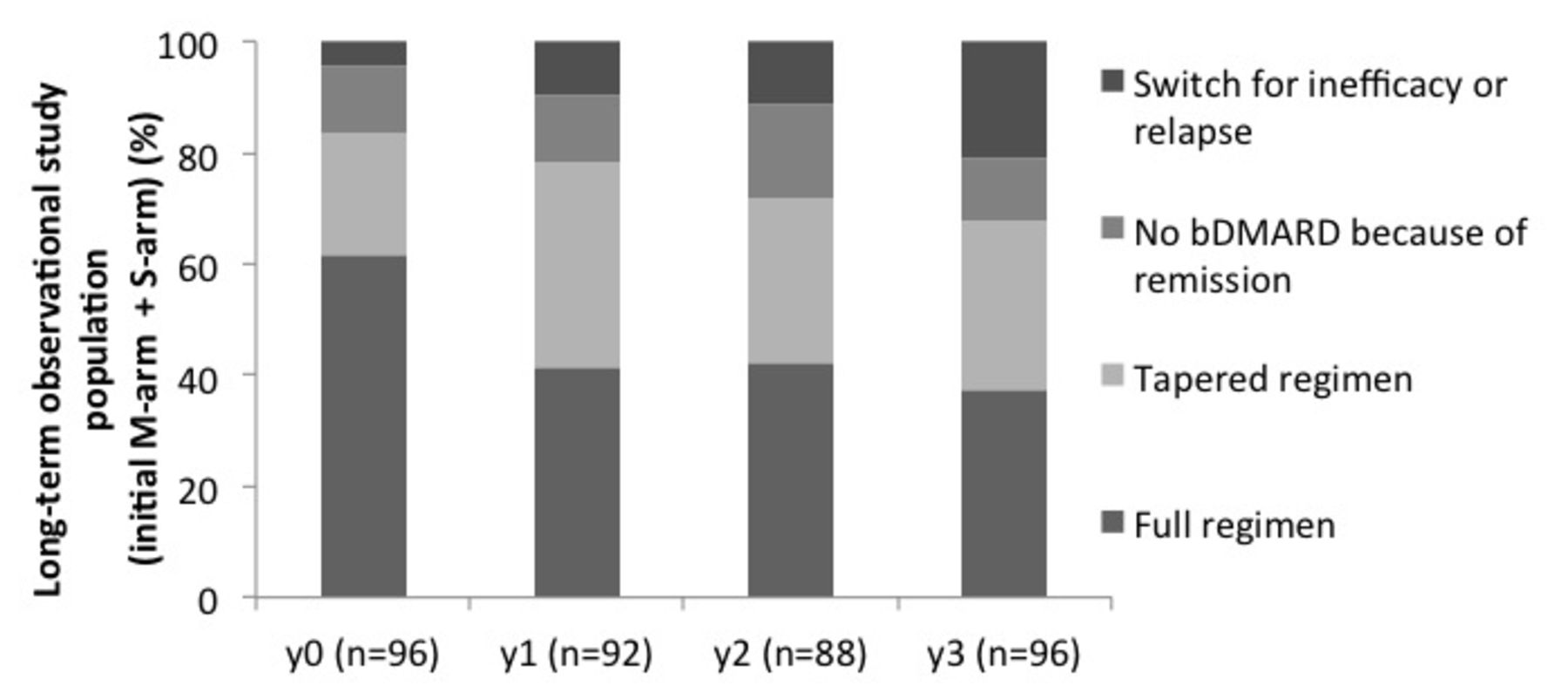
Among the 96 patients, 11 (11.5%) were able to completely stop their bDMARD at 3 years (figure 2), 29 (30.2%) had a tapered regimen, with whatever length of injection interval, and 36 (37.5%) had a full-dose regimen. In the two subgroups (initial M-arm and S-arm), 5.8% and 18.2% stopped their bDMARD (p=0.06), 28.8% and 31.8% spaced their injections (p=0.76) and 44.2% and 29.5% kept or returned to the full-dose regimen (p=0.14).
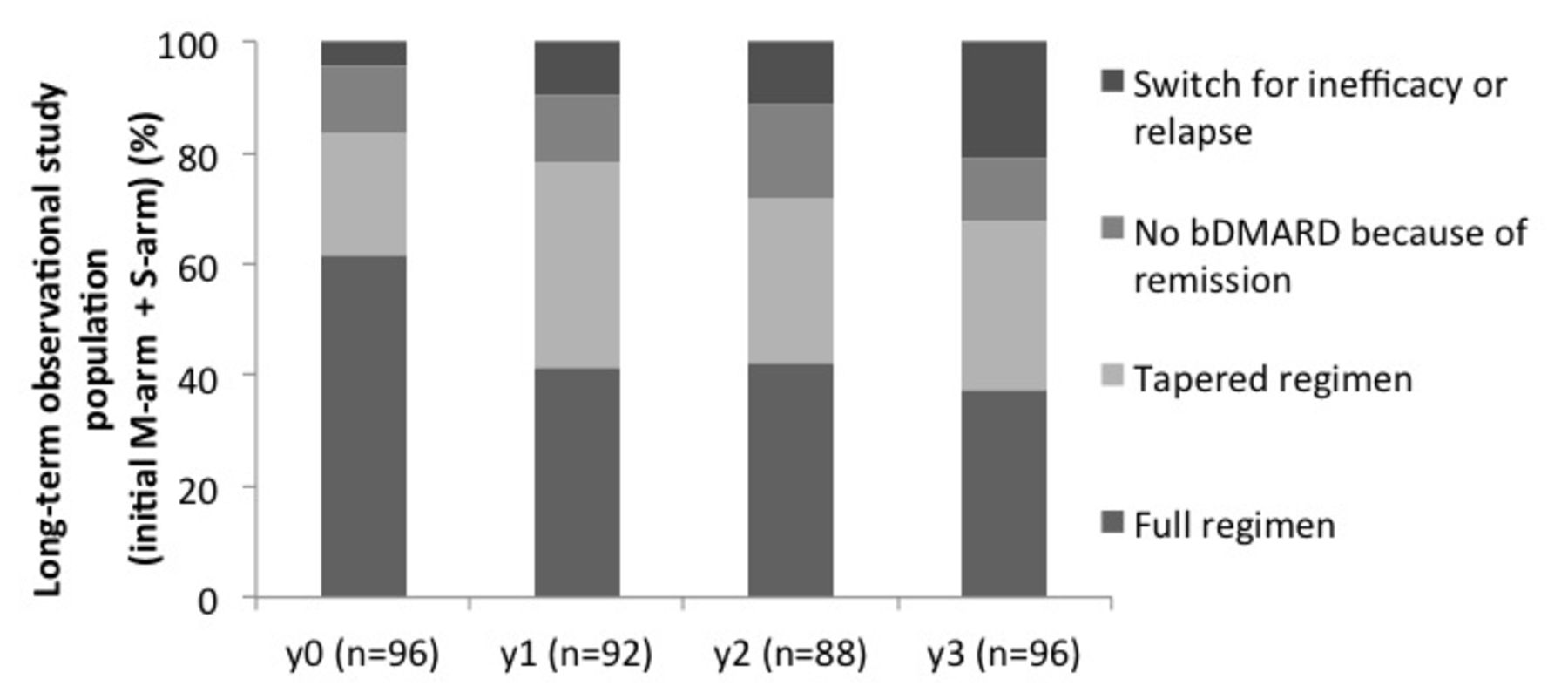
bDMARDs intake over time. bDMARD, biological disease-modifying antirheumatic drug; M-arm, maintenance arm; S-arm, spacing arm; y0, start of the long-term observational study.
bDMARD regimen at 3 years
Among patients who kept their initial bDMARD, the mean dose quotient at the end of the extended follow-up was 66%±36%, 74%±34% for patients in the initial M-arm and 58%±39% in the initial S-arm (p=0.06) (figure 3).

Dose quotient of bDMARDs intake over time. Data are presented as mean percentage. bDMARD, biological disease-modifying antirheumatic drug; dose quotient, ratio of actual bDMARD total intake over a month to standard bDMARD full regimen intake over a month; M-arm, maintenance arm; S-arm, spacing arm; y0, start of the long-term observational study.
Switches of ETA or ADA
During the 3 years of follow-up, 20 patients (20.8%) had to switch treatment because of loss of efficacy: 11 in the initial M-arm (21.2%) and 9 in the initial S-arm (20.5%) (p=0.94; figure 2 and online supplementary table S1). No switch for safety issues was observed.
Supplementary file 3
Survival without relapse
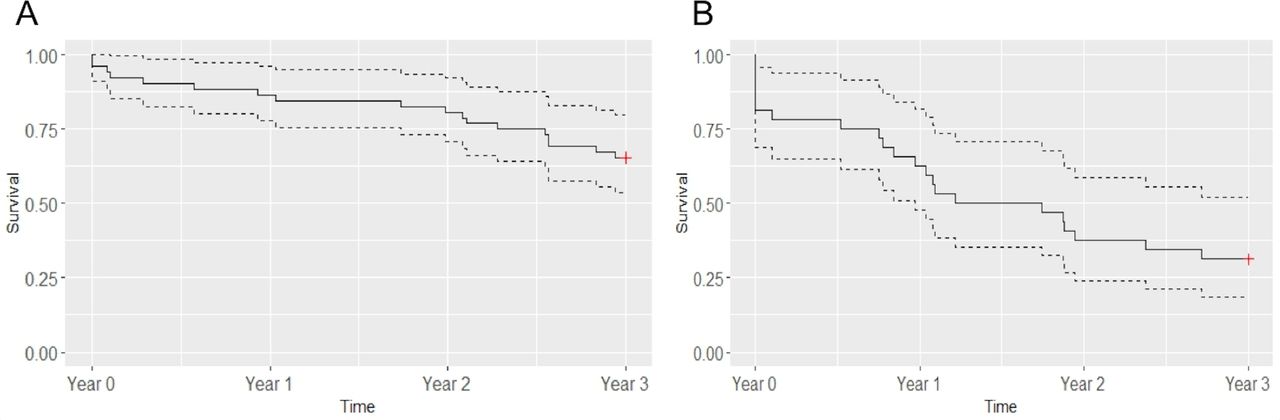
For patients with spaced TNF-blockers at the beginning of the follow-up, survival proportions without relapse were 65.4% (95% CI 53.7% to 79.7%) and 31.2% (18.7% to 52.2%) for those in the initial M-arm (figure 4A) and the initial S-arm (figure 4B). The predictors significantly associated with relapse were ACPAs positivity (HR 3.34 (95% CI 1.30 to 8.66)), initial spacing arm (HR 2.35 (95% CI 1.10 to 5.09)) and DAS28 at the beginning of the long-term extension study (HR 1.72 (95% CI 1.05 to 2.86)).
![[SP2.jpg]](https://rmdopen.bmj.com/content/rmdopen/3/2/e000474/DC2/embed/inline-supplementary-material-2.jpg?download=true){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Survival curves without relapse for patients in the initial maintenance arm (A) and patients in the initial spacing arm with effective spacing at the beginning of the follow-up (B). Data are proportion (solid line) and 95% CIs (dotted lines); n=52 in the initial maintenance arm and n=32 in the initial spacing arm.
Discussion
Although long-term evaluation is essential to adequately assess the relevance of therapeutic strategies, only a few studies reported such a long follow-up to explore the management of RA in remission in real-life clinical settings because the treatment strategy was at the discretion of the physician. Unlike patients randomised in tapering arms who must follow a strict pre-established step-down strategy, our patients with RA from the STRASS were under a more gradual spacing strategy, which also explains the low rate of bDMARD-free patients. In addition, we found a fair maintenance rate of 75% at 3 years. Although exact disease activity figures during the long-term follow-up were not available, our relatively high rate of patients with a tapered regimen suggests the sustainability (thus efficacy and tolerance) of such a strategy. Indeed, tight control and treat-to-target principles being widely applied, RA relapse or increases in disease activity were likely to be managed by treatment intensification by return to full dose.
The present study has shown that complete discontinuation of TNF-blockers during 3 years remains a rare event although truly feasible for a few patients (11.5%). Definitely, current bDMARDs are efficacious but are not able to cure RA; thus, their tapering requires careful monitoring and the continuation of the treat-to-target principle. TNF-blocker tapering seems a more achievable objective because 30.2% had a tapered regimen 3 years after the end of the STRASS trial. This rate was similar whatever the initial randomisation arm, maintenance or spacing.
In the STRASS trial and this follow-up study, the spacing strategy was chosen over a dose decreasing strategy. Decreasing the dose is indeed a good alternative for intravenous drug such as infliximab because the quantity of the drug can be easily adjusted. However, with regard to subcutaneous drugs, increasing the interval between injections allows a better handling in dose decreasing and appears more flexible to patients and physicians. Moreover, it has been previously showed that certolizumab pegol at the dose of 200 mg every 2 weeks is not different from 400 mg every 4 weeks.17 The proportion of more than one-third of patients with sustained tapered regimen is lower than that from short-term randomised controlled trials. In the two main studies with a DAS-steered progressive spacing of TNF-blocker injections—STRASS14 and DRESS (Dose REduction strategy of subcutaneous TNF inhibitors)10—the proportion of patients with spaced injections (or no injection) at 18 months was higher than in our longer-term follow-up: 75% and 63%, respectively. Conversely, in DRESS, only 9 out of 59 patients in the ‘usual care’ group (dose reduction or discontinuation discouraged but allowed) had spaced injections because of LDA.10 These data indicate that sustained remission despite treatment tapering remains challenging.
The dose quotient we found was about 70% of the full-dose regimen; in other words, the progressive spacing strategy enabled only a 30% reduction of the bDMARD regimen. This was less than the regimen reduction observed in the two short-term DAS-driven tapering trials (DRESS and STRASS) and was less than the half dose tested in two dose-reduction trials.8 18 PRESERVE8 is a large randomised, blinded, three-armed, placebo-controlled clinical trial of patients with established RA who had achieved a stable LDA state after an initial open-label period with ETA plus methotrexate: one-third continued with unchanged medication, one-third received a reduced dose of ETA (50%; ie, 25 mg per week) and one-third continued on methotrexate alone. After 52 weeks, patients with the half dose and full dose of ETA did not differ: 79% and 82.6% achieved LDA. However, our results are consistent with a previous observational study of infliximab in the Netherlands.6 Infliximab was down-titrated with 25% of the original dose (ie, 3 mg/kg) every 8–12 weeks without interval change until discontinuation. At 1 year, infliximab could be down-titrated in 45% of patients, and the mean infliximab dose decreased significantly from 224 mg per infusion at start to 130 mg (ie, 42% reduction).
The treatment switch rate we found for inefficacy or relapse may be considered substantial (18.7%), which raises the legitimate question of loss of response after a down-titration strategy. A first answer is given by the DOSERA (Dose Reduction or Discontinuation of Etanercept in Methotrexate-Treated Rheumatoid Arthritis Patients Who Have Achieved a Stable Low Disease Activity-State) study,18 comparing full-dose (50 mg/week) and half-dose (25 mg/week) ETA. At 1 year, 91% of patients considered treatment failures showed response when resuming full-dose ETA under open-label conditions, which provides a measure of reassurance on this point. As well, Kaine et al 19 showed that the 3-month discontinuation of subcutaneous abatacept was well tolerated, with no significant impact on immunogenicity. However, many factors may influence immunogenicity of bDMARDs, including the treatment regimen. Bendtzen et al,20 showed that patients with low trough levels of infliximab after two infusions were prone to subsequent positivity for anti-infliximab antibodies. Moreover, risk of immunogenicity is not exactly identical between bDMARDs. Indeed, more than 40% to 60% of patients receiving infliximab show antidrug antibodies,21 22 and 20% receiving ADA.22 23 Other TNF-blockers and bDMARDs seem less immunogenic.19 24–26 Hence, a tapered regimen could in theory be more appropriate for the least immunogenic molecules. However, no published data support such a conclusion.
Relapse appeared to be an earlier and more common event in patients from the initial S-arm than M-arm and occurred from the very beginning of the follow-up. A forced and fast spacing (as in the S-arm during the STRASS trial) may increase the risk of relapse in a real-life setting as compared with a more progressive and slower tapering strategy.
Among 43 patients with an X-ray evaluation at 3 years, about 30% showed structural damage progression. Although this is a non-validated qualitative assessment of joint damage made by the ‘local’ rheumatologist, this result is consistent with some studies.10 14 Lillegraven et al found that 30% of patients with RA in DAS28-CRP remission showed radiographic progression at 2 years.27 Thus, the composite scores (association of clinical and biological criteria) do not seem to be an optimal tool to detect patients who could safely benefit from a tapered strategy.
This study has some limitations: first this was a relatively small observational survey based on usual care assessments. Second, although we included more than 75% of the completer STRASS population, the substantial number of patients lost to follow-up might have caused a bias not in favour of patients who were able to remain bDMARD free. Third, we had limited radiographic data, which did not allow for robust conclusions. Fourth, results regarding the comparison between the two groups should be interpreted with caution because of the differences at the start of the extension study in terms of disease activity and experience of injection spacing failure for some patients in the spacing arm and differences in the therapeutic strategies implemented in the two arms that were not protocolised. Finally, we had no formal assessment of utilities and health resource use during the long-term observational study, and we cannot demonstrate the long-term economic benefit of such DAS-driven tapering strategies to society.
This retrospective observational study conducted as a follow-up to the STRASS trial shows that complete discontinuation of TNF-blockers during 3 years is rare and feasible for only a few patients. bDMARD tapering seems a common and reliable strategy in clinical practice. Additional studies are needed to define optimal disease activity-steered tapering strategies and to identify patients who could benefit from such strategies with minimal risk of relapse.
Acknowledgments
The authors thank all patients who participated in the trial and the following physicians who contributed to the data collection in their respective institution: Dr E. Dernis (Rheumatology Department, Le Mans Hospital, Le Mans); M. Trabelsi (Rheumatology Department, Joseph Fourrier University, Sud Hospital, Grenoble); Dr O. Brocq (Rheumatology Department, Princess Grace Health Centre, Monaco); Dr J-M. Berthelot (Rheumatology Department, Hotel-Dieu Hospital, Nantes); Dr J-C. Balblanc (Rheumatology Department, Belfort-Montbeliard Health Center, Belfort).
References
Footnotes
Contributors All persons who meet authorship criteria are listed as authors, and all authors certify that they have participated sufficiently in the work to take public responsibility for the content, including participation in the concept, design, analysis, writing or revision of the manuscript. Specific contributions made by each author. JS and FB contributed equally to this paper. JS, FB, BF and LG conceived the project, organised the study and wrote the paper. JS, FB, FT and DH conducted the statistical analyses. All authors participated in the project construction and realisation, as well as the discussion and interpretation of results.
Competing interests The authors declare a potential conflict of interest having received grant support and/or honoraria for consultations and/or for presentations as indicated: JS: BMS, MSD; XM: BMS, Celgene, GSK, Lilly, MSD, Novartis, Pfizer, Sanofi, UCB; JM: Abbvie, Pfizer, MSD, UCB; FT: research grants from Abbvie, Pfizer, Janssen, MSD, AstraZeneca, Lundbeck; LG: Abbvie, BMS, Celgène, Chugai, Janssen, MSD, Novartis, Pfizer, Roche, UCB; BF: AbbVie, BMS, Celgène, Hospira, Janssen, Lilly, MSD, Nordic, Novartis, Pfizer, R-Pharm, Roche-Chugai, UCB.
Ethics approval CPP, Ile de France VI.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.