Article Text

Abstract
Objective Acute anterior uveitis (AAU) is the most common extra-articular manifestation of axial spondyloarthritis (axSpA). In this study, patients presenting with AAU were evaluated clinically and with MRI in order to estimate the prevalence of axSpA.
Methods Consecutive patients presenting to a university teaching hospital between February 2014 and March 2015 with AAU were invited to participate. Those with a history of chronic back pain (CBP) beginning <45 years were evaluated clinically and with MRI of thoracolumbar spine and sacroiliac joints.
Results Of 366 patients with AAU, 57 had a pre-existing diagnosis of axSpA; 77 others fulfilled the study eligibility criteria and 73 (95%) completed the study. Seventeen patients (23.3%) were diagnosed with axSpA by an experienced rheumatologist; of these, eight were human leucocyte antigen-B27 negative. Including those with a previous diagnosis, this equates to a minimum axSpA prevalence of 20.2%; one-quarter of patients were previously undiagnosed.
Conclusion This is the first study to actively search for the presence of axSpA in unselected patients presenting with AAU utilising MRI as an essential part of the assessment. There is a significant burden of undiagnosed axSpA in patients with AAU, but there does not appear to be a simple mechanism for screening. We recommend that ophthalmologists refer all patients with AAU with CBP, onset <45 years, to rheumatology for further evaluation.
- ankylosing spondylitis
- spondyloarthritis
- magnetic resonance imaging
- low back pain
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Acute anterior uveitis (AAU) is known to be the most common extra-articular manifestation of axial spondyloarthritis (axSpA).
What does this study add?
In this study, the minimum prevalence of axSpA in AAU was 20.2%, with nearly one-quarter of patients previously undiagnosed despite many years of back pain.
How might this impact on clinical practice?
There is no easy referral strategy; previously published pathways would have missed a significant amount of new diagnoses in our cohort.
We recommend that ophthalmologists refer all patients with AAU with chronic back pain, onset <45 years, to rheumatology for further evaluation regardless of human leucocyte antigen-B27 status, gender or number of episodes of AAU.
Introduction
Axial spondyloarthritis (axSpA) is a chronic inflammatory disease which primarily affects the axial skeleton. The prevalence is approximately 0.7% in the general population,1 and there is a strong genetic association with human leucocyte antigen (HLA)-B27.2 Symptoms usually begin in the second or third decade3 and can have a major impact on health and quality of life.4 The spectrum of axSpA as defined by the Assessment of Spondyloarthritis International Society (ASAS) includes non-radiographic axSpA and ankylosing spondylitis (AS).2
Acute anterior uveitis (AAU) is the most common extra-articular manifestation of axSpA5 6; its prevalence increasing with disease duration.7 Diagnostic delay is reported frequently in axSpA3 8 9 and is associated with worse outcomes.10 Given that spinal symptoms usually precede the first episode of AAU, targeted screening of patients presenting with AAU may enable an earlier diagnosis of axSpA.
In this study, patients with AAU were evaluated clinically by an experienced rheumatologist and underwent MRI in order to estimate the prevalence of axSpA and determine the hidden burden of disease.
Methods
Patients
Consecutive adult patients presenting to the ophthalmology department of a teaching hospital with a verified diagnosis of non-traumatic, non-infective AAU between February 2014 and March 2015 were invited by letter to participate. A further letter was sent to non-responders. Patients with a self-reported history of chronic back pain (CBP) beginning before the age of 45 years were included. Those with a pre-existing diagnosis of axSpA, sarcoidosis or Behçet’s disease, or in whom MRI was contraindicated, were not investigated further. The hospital notes of patients with a reported diagnosis of axSpA, including AS, were interrogated to confirm that the diagnosis had already been made by an experienced rheumatologist.
Clinical assessment
Patients who agreed to participate were reviewed by an experienced rheumatologist; clinical assessment included history, physical examination, patient-reported outcome measures and laboratory investigations.
MRI
MR examinations were performed using a standard protocol for imaging individuals with suspected axSpA, including spectral fat saturation images of the thoracolumbar spine and sacroiliac joints (SIJ). Images were reported by experienced musculoskeletal radiologists blinded to the clinical data and verified by an experienced rheumatologist (MS).
Diagnosis
The diagnosis of axSpA was made by an experienced rheumatologist following review of the clinical history, examination, laboratory and MRI findings.
Statistics
Results are reported as means (compared using the two-tailed Student’s t-test) or percentages (compared using the Χ2 test or Fisher’s exact probability test).
Results
Recruitment through the study is shown in figure 1. Of 366 patients who presented with non-traumatic, non-infective AAU, 241 (66%) responded to the invitation; 57 subjects were already diagnosed with axSpA (verified from clinical notes); 77 others were eligible for the study and 73 (95%) completed the study, including undergoing MRI. Responders were older than non-responders (P<0.0001) and were more likely to be female (P=0.006).

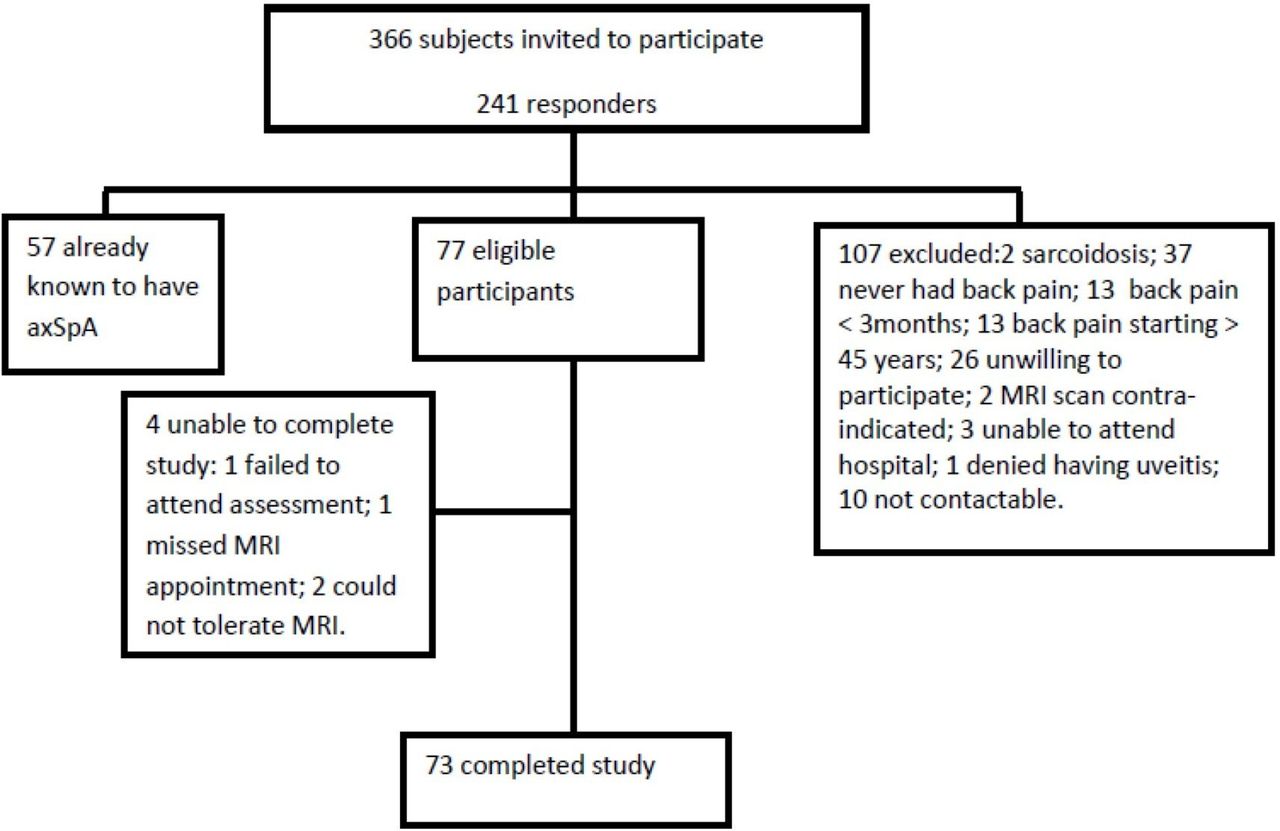{kind=link}
Consort diagram. AxSpA, axial spondyloarthritis.
Seventeen subjects (23.3%) were diagnosed with axSpA by an experienced rheumatologist. Of these, 13 fulfilled the ASAS classification criteria2 (12 imaging and one clinical). Of the four remaining patients, three had widespread entheseal oedema on spinal MRI, consistent with the ASAS definition of a positive spinal MRI,11 and although the fourth patient had an equivocal SIJ MRI, the clinical phenotype was typical of axSpA in view of prominent inflammatory-type back pain (IBP) and Crohn’s disease which was already being treated with infliximab. Twelve additional patients fulfilled the clinical arm of the ASAS classification criteria but were not considered to have axSpA when assessed by an experienced rheumatologist.
Table 1 summarises the MRI findings in the patients newly diagnosed with axSpA.
MRI findings in patients diagnosed with axial spondyloarthritis
Findings in the 56 patients not diagnosed with axSpA were: degenerative/mechanical spinal changes (including prolapsed intervertebral discs, dehydrated intervertebral discs, lumbar spondylosis, spondylolisthesis, scoliosis and facet joint osteoarthritis) in 40 patients; of these, five had a single ‘inflammatory’ corner lesion at one level, associated with mechanical disc disease; two had Scheuermann’s disease; six had osteoarthritis of the SIJs with a small area of secondary bone marrow oedema (BMO) in two of these patients; osteitis condensans ilii in one patient and fibrous dysplasia in the iliac bone in one patient. Some patients had more than one of these findings and there were 10 entirely normal scans.
Including those with a previous diagnosis verified by an experienced rheumatologist (57 patients), this equates to an estimated minimum axSpA prevalence of 20.2% (95% CI 16.1 to 24.3). Of these, 22.9% were previously undiagnosed.
Table 2 outlines the demographics and clinical characteristics of study participants.
Clinical characteristics of subjects
Those diagnosed with axSpA were more likely to be have a raised C-reactive protein (P=0.014), have a prior diagnosis of inflammatory bowel disease (P=0.009) and have a higher Bath Ankylosing Spondylitis Metrology Index (P=0.001). A larger proportion of patients diagnosed with axSpA were HLA-B27 positive, but this did not reach statistical significance. IBP did not predict a physician diagnosis of axSpA.
Five patients (29.4%) were diagnosed following a single episode of uveitis. Two of these patients were HLA-B27 negative.
Discussion
This is the first study to actively search for the presence of axSpA in unselected patients presenting with AAU utilising MRI as an essential part of the assessment. Including patients with a prior diagnosis, the minimum prevalence of axSpA is 20.2%, with nearly one-quarter of patients previously undiagnosed despite years of back pain. This represents a significant hidden burden of disease.
Two other studies have recently investigated axSpA prevalence in patients with AAU.12 13 However, as known cases were excluded, neither study could report the overall prevalence of axSpA in the group. Juanola et al 12 also excluded HLA-B27 negative patients with a single episode of AAU, but in our cohort, 12% of patients newly diagnosed with axSpA met those exclusion criteria. Haroon et al 13 reported that 40% of patients presenting with AAU had undiagnosed SpA, although it is unclear how many of these patients underwent MRI.
Although this is a relatively small single-centre study, the sample size was sufficient to calculate the prevalence with a reasonable degree of precision. The main risk of bias is in the self-selection of responders to the initial invitation; responders were significantly more likely to be older and female. We have made the assumption that non-responders did not have back pain, or by extension axSpA, and have presented our results as minimum estimated prevalence. However, we accept this could have led to an underestimate of the overall prevalence. We also based our calculations on diagnoses made by an experienced rheumatologist; it is not always clear how other studies arrived at their figures and, for example, had we included all patients who met the ASAS classification criteria within the ‘positive diagnoses’ (which we are very clear is not how classification criteria should be used), 40% patients assessed would have been assigned a ‘diagnosis’ of axSpA.
Establishing a diagnosis of axSpA is difficult; consequently, there is often a considerable delay to diagnosis and a potential to ‘over diagnose’ based on subtle or non-specific MRI changes.14 The gold standard is ‘physician-verified diagnosis’, which is based on clinical assessment including interpretation of laboratory tests and imaging. Classification criteria should only be applied following diagnosis and have been developed to ensure homogeneity in groups of patients for research purposes,15 although the positive predictive validity of the ASAS axSpA classification criteria to forecast an expert’s diagnosis of ‘SpA’ after more than 4 years is good.16 The imaging arm of the ASAS axSpA classification criteria requires the presence of sacroiliitis on MRI or X-ray and the ASAS/Outcome Measures in Rheumatology definition of a positive spinal MRI11 is not currently included in the formal ASAS classification system and so potentially patients with spinal inflammation in the absence of sacroiliac inflammation could be overlooked. This observation has been well described especially in patients with longstanding disease.17 One of the potential limitations of an MRI-based study is the potential to over or misinterpret MRI findings. Three of our B27-negative patients diagnosed as axSpA did not fulfil the ASAS definition of a positive SIJ MRI; however, we consider any potential ‘over diagnosis’ unlikely by virtue of them having a typical axSpA clinical phenotype verified an experienced rheumatologist including IBP onset <45 years, recurrent AAU and extensive spinal inflammatory lesions seen on MRI. Conversely, there were many more patients (12) who fulfilled the ASAS classification criteria who we considered not to have the disease.
Other potential limitations include the fact that only a single MRI was undertaken, so potentially fluctuating BMO could have been missed18 19 and that plain radiographs were not undertaken. This was due to the fact that ethics approval was not forthcoming as it was considered that this would expose too many patients to unnecessary radiation, and MRI was being undertaken as a more comprehensive imaging modality. As a result of a lack of plain radiographs, we cannot state how many patients met the modified New York Criteria for AS. Many patients had chronic changes on MRI which may reflect the long average delay to diagnosis of over 20 years. Had these patients been screened for axSpA following their first episode of AAU, the diagnostic delay could have been reduced by 7 years on average. Given the high prevalence of axSpA among patients with AAU, targeted screening may offer a unique opportunity to identify undiagnosed axSpA especially as AAU may prompt the first interaction with secondary care.20
In clinical practice, HLA-B27 positivity is often the trigger for a rheumatology referral in patients with AAU. Indeed, the Dublin Uveitis Evaluation Tool (DUET) algorithm proposed by Haroon et al prompts referral if a patient is HLA-B27 positive (or has co-existing psoriasis or peripheral arthritis), with high reported sensitivity and specificity of 96% and 97%, respectively.13 This may reflect the status of HLA-B27 as the anchor criterion for the clinical arm of the ASAS criteria. In our cohort, the sensitivity and specificity of the DUET algorithm were 52.9% (95% CI 27.8 to 77.0) and 67.9% (95% CI 54.0 to 79.7), respectively. Nearly half of new diagnoses were HLA-B27 negative (none of whom had psoriasis or a recent history of joint pains requiring a GP visit). By applying the DUET algorithm, these HLA-B27 negative patients would have been overlooked. Similarly, the presence of IBP did not predict the diagnosis of axSpA or a positive MRI. Had we relied on IBP rather than CBP before age 45 as a referral strategy, nearly two-thirds of new diagnoses would have been overlooked.
In summary, there is a high prevalence of undiagnosed axSpA in patients presenting to secondary care with AAU. There does not appear to be a simple mechanism for screening these patients, so given the significant burden of ‘hidden’ axSpA, we recommend that ophthalmologists refer all patients with AAU with CBP, onset <45 years, to rheumatology for further evaluation regardless of HLA-B27 status, gender or number of episodes of AAU. Close collaboration between rheumatology and ophthalmology is necessary in order to facilitate this targeted approach to patient care.
Acknowledgments
None
References
Footnotes
Contributors All authors were involved in the data collection and had input into the final report.
Funding This study was funded by AbbVie Ltd.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Ethical approval was provided by NRES Committee East of England – Norfolk (reference number 13/EE/0442).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Additional data may be available by contacting the corresponding author.