Article Text

Statistics from Altmetric.com
Key messages
What is already known about this subject?
Nail involvement is part of the clinical spectrum of psoriatic arthritis and responds to tumour necrosis factor (TNF) inhibitors.
What does this study add?
This small study assessed patients with psoriatic arthritis with nail disease and active distal interphalangeal (DIP) arthritis before and after 6 months of TNF inhibitor treatment.
Persistent inflammatory changes in and around the DIP joint were seen on follow-up MRI scans despite a good clinical response.
How might this impact on clinical practice?
Further studies are needed to see whether these inflammatory changes resolve with a longer duration of treatment or relate to radiographic progression of the arthritis.
Nail involvement is part of the clinical spectrum of psoriatic disease and is microanatomically associated with distal interphalangeal joint (DIPJ) entheses.1 Tumour necrosis factor (TNF) inhibitors have shown efficacy for psoriasis, arthritis, enthesitis, dactylitis and nail disease.2 Given the intimate links between psoriatic arthritis (PsA) and nail disease, it might be expected that nail disease improvement would be associated with resolution of the underlying arthropathic features.
All participants gave written consent. All cases fulfilled the Classification Criteria for Psoriatic Arthritis (CASPAR) criteria for PsA.3 All cases were due to start TNF inhibitor therapy for active PsA. A clinical and MRI assessment was performed at baseline and after 6 months of treatment.
High-resolution MRI was performed on one finger, with gadolinium contrast and Vaseline applied to the nail.4 The target finger for imaging was selected for current nail disease and active DIPJ arthritis. The MRIs were scored as previously reported.5 Seven patients were recruited. All patients had tenderness and swelling of the target finger’s DIPJ at baseline. TNF inhibitor prescription was made according to the National Institute for Health and Care Excellence guidelines. Four patients received etanercept and three adalimumab.
Marked improvements were seen in clinical parameters at 6 months. No patients had residual clinical swelling in the target DIPJ and one had persistent tenderness (table 1). Onycholysis and pitting were the most frequent abnormalities at baseline. Two patients had completely normal nails in the target finger at 6 months, with no difference in nail clearance between nail matrix features and nail-bed abnormalities.
Clinical assessments
Baseline MRI scans showed DIPJ enthesitis, bone marrow oedema (BMO) or synovitis in all patients (86%, 71% and 100%, respectively) (table 2). Collateral ligament enthesopathy was seen in 86%, flexor tendon enthesopathy in 71% and extensor tendon enthesopathy in 86%. Three patients with purely nail-bed nail disease at baseline also had marked underlying BMO, synovitis and enthesitis on MRI.
MRI scores for each patient
Follow-up MRI scans surprisingly showed persistent inflammatory changes in the DIPJ, distal phalanx and soft tissues around the nail (table 2, figure 1). No patient with baseline BMO showed complete resolution, and four of the five had no change in BMO score. All seven patients had synovitis at baseline; this resolved in two, improved in one, was unchanged in three and worsened in one patient. No patient had complete resolution of extensor tendon abnormalities. Collateral ligament abnormalities were largely unchanged. No relationship was seen between the MRI changes and clinical response to treatment.
{kind=link}
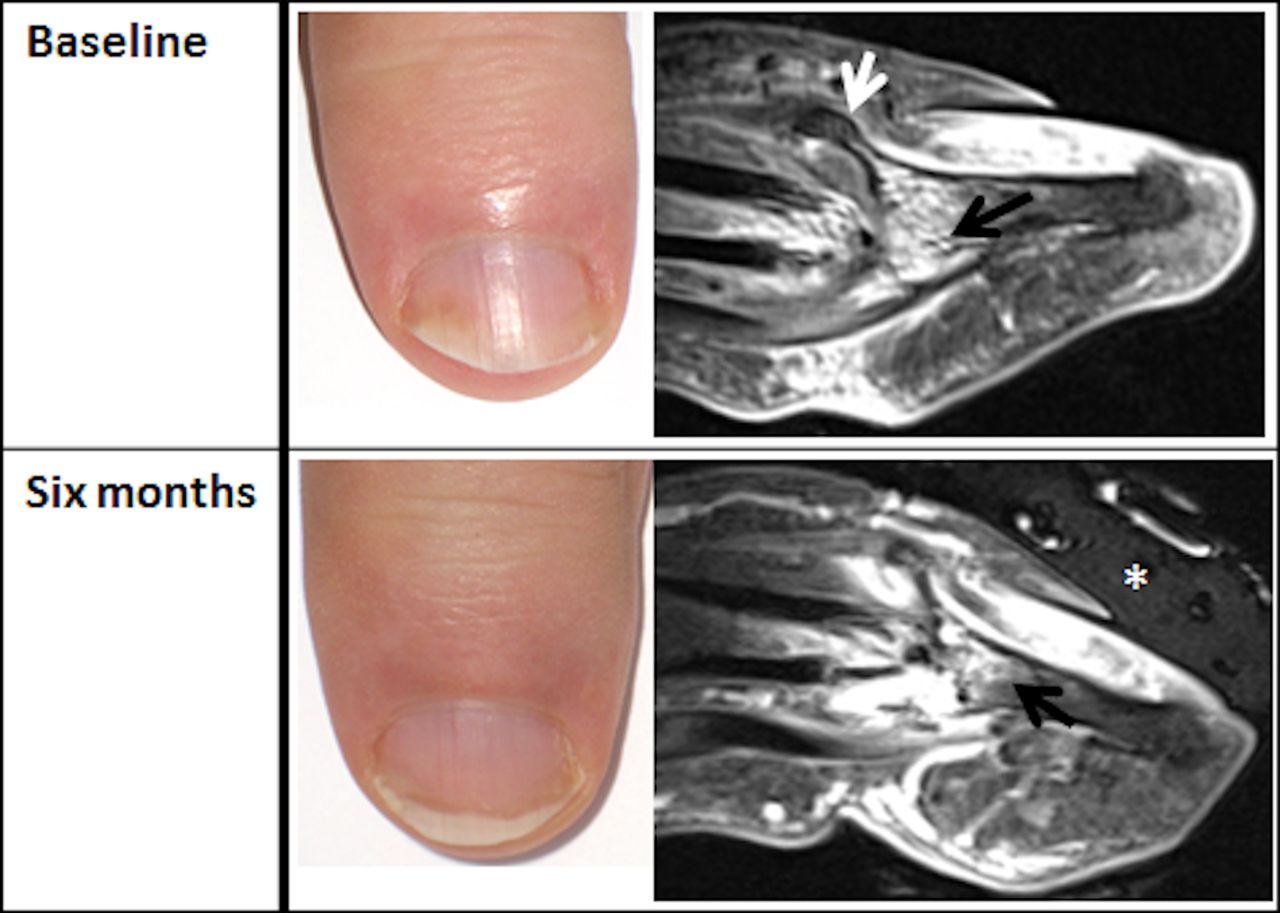
Nail photographs and MRI scans of a patient with psoriatic arthritis. Improvements in the nail appearances are seen on the photograph. Vaseline (asterisk) is seen overlying the nail on MRI. At baseline, a large enthesophyte is seen at the extensor tendon enthesis (white arrow) with diffuse bone marrow changes (black arrow). After 6 months of treatment with etanercept, persistent bone marrow changes are seen (black arrow), with a greater degree of synovitis.
Previous PsA MRI studies have shown conflicting data regarding the resolution of inflammation with TNF inhibitors, some reporting improvements or resolution, others finding persistent inflammation.6–10 In one study, greater reductions in BMO volume were seen at 18 months than 6 months.10 Our data are limited by the small number of patients and short duration of follow-up. In conclusion, our study demonstrated persistent subclinical musculoskeletal inflammation on MRI despite a good clinical response. Further imaging in larger cohorts with a longer duration of follow-up is needed to demonstrate the natural history of inflammatory lesions under therapy and the potential link to disease progression.
References
Footnotes
Contributors All authors contributed to the design and data collection and analysis.
Funding This research is supported by the National Institute for Health Research (NIHR) Leeds Biomedical Research Centre. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health. ZA was supported by an unrestricted educational grant from Merck Sharp & Dohme.
Competing interests ZA: unrestricted educational research grant from Merck Sharp & Dohme, and funding to attend conferences and/or speaking fees from Abbott, Chugai, Pfizer and MSD. HM-O: honoraria and/or speaking fees from AbbVie, Celgene, Janssen, Lilly, MSD, Pfizer and UCB. DGM: honoraria and/or speaking fees from Abbott, MSD, Pfizer, UCB and Janssen.
Ethics approval Ethical approval for this small pilot study was obtained from Leeds Ethics.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.
Presented at This paper has been previously published online as part of a Doctor of Medicine Thesis, University of Leeds Ethos. ID: uk.bl.ethos.589288.