Article Text

Abstract
Objective To evaluate long-term clinical, functional and radiographic outcomes in an open-label extension (OLE) study in patients with rheumatoid arthritis (RA) receiving adalimumab monotherapy or adalimumab+methotrexate following attainment of low disease activity (LDA) with adalimumab+methotrexate.
Methods Methotrexate-naive patients with early RA were randomised to adalimumab, methotrexate or adalimumab +methotrexate in a double-blind, 2-year study. Patients who completed the study and achieved LDA (28-joint Disease Activity Score using C reactive protein (DAS28(CRP)<3.2) could receive adalimumab monotherapy for up to 8 additional years in the OLE; open-label methotrexate could be added per investigator’s discretion. This post hoc analysis included data up to OLE year 3 (study year 5) from patients receiving adalimumab+methotrexate who achieved LDA at year 2 followed by adalimumab monotherapy or methotrexate reinitiation. Normal physical function was defined as Disability Index of the Health Assessment Questionnaire <0.5 and radiographic non-progression as change in modified total Sharp score ≤0.5.
Results Of 140 patients initiating adalimumab monotherapy, 84 (60%) received adalimumab only (methotrexate non-use) and 56 (40%) reinitiated methotrexate (methotrexate use) during OLE treatment. Median (IQR) time to first methotrexate use was 5.1 (0.1–31.4) weeks. Among methotrexate users, 61% retained LDA, 48% achieved DAS28(CRP) <2.6, 45% had normal physical function and 46% had no radiographic progression at year 5; for non-users, 63%, 50%, 58% and 50%, respectively, achieved these milestones. Adverse event rates were similar between methotrexate non-use and use patients.
Conclusions Adalimumab monotherapy effectively maintained good clinical, functional and radiographic outcomes for up to 3 additional years in ≥50% of patients who attained LDA after 2 years of adalimumab+methotrexate therapy.
Trial registration number NCT00195663; Post-results.
- anti-tnf
- methotrexate
- rheumatoid arthritis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
The combination of adalimumab and methotrexate demonstrated radiographic, clinical and functional superiority compared with adalimumab or methotrexate monotherapies in patients with early, aggressive rheumatoid arthritis in the 2-year PREMIER study.
Per the current treatment guidelines, if a patient achieves remission with combination therapy, the recommendation is to taper biologic therapy and continue with methotrexate monotherapy; however, personal preference or intolerance may necessitate discontinuation of methotrexate in some patients.
What does this study add?
Following attainment of low disease activity (LDA) after 2 years of adalimumab+methotrexate therapy, adalimumab monotherapy permitted ≥50% of the patients to retain LDA, normal physical function and minimal radiographic progression for up to 3 years.
Methotrexate was reinitiated in 40% of patients and comparison between groups who stopped or reinitiated methotrexate did not suggest significant differences during follow-up.
How might this impact on clinical practice?
Continuation of combination therapy or tapering of adalimumab may be suitable for many patients once clinical target has been achieved with initial adalimumab+methotrexate therapy; however, methotrexate withdrawal may be possible for some patients.
Introduction
Rheumatoid arthritis (RA) is a chronic systemic inflammatory disease that primarily affects the synovial joints. The current treatment guidelines recommend the use of conventional synthetic disease-modifying antirheumatic drugs (csDMARDs), such as methotrexate, as part of an initial treatment strategy, followed by an addition of a biologic DMARD if treatment target is not attained and poor prognostic factors are present.1 Furthermore, if a patient is in remission, tapering biologic DMARDs should be considered, especially if the treatment is combined with csDMARDs. However, although treatment recommendations indicate that biologic DMARDs, such as tumour necrosis factor (TNF) inhibitors, should be administered in combination with methotrexate because of increased efficacy1–4 and because patients reportedly prefer combination therapy,5 the proportion of patients in registries receiving biologic DMARDs as monotherapy is higher than the proportion expected to be intolerant to methotrexate.6 7
A combination treatment with a TNF inhibitor and methotrexate suppresses inflammation, reduces the risk of joint damage or progression and improves physical function more effectively than methotrexate alone.8–13 However, methotrexate may cause mild adverse events (AEs) such as diarrhoea, nausea and headache.14–17 As such, withdrawing methotrexate treatment may be desirable for some patients. Despite an increased interest in understanding whether TNF inhibitors can be safely withdrawn from patients with RA receiving combination therapy once a clinical target has been achieved,18 the ability of the TNF inhibitor to maintain the target as monotherapy following methotrexate withdrawal has received less consideration.
Analysis of the biologic register of the Dutch Rheumatoid Arthritis Monitoring Project indicated that in patients with RA receiving combination therapy consisting of a TNF inhibitor and methotrexate, disease activity decreased after methotrexate withdrawal.19 Additionally, the duration that patients were able to stay on TNF inhibitor therapy was comparable between those who had methotrexate withdrawn and those who continued on combination therapy. Similar results were found in a smaller observational extension study.20 Furthermore, in an open-label trial of patients receiving etanercept with or without methotrexate who had achieved low disease activity (LDA)/remission at 6 months, similar radiographic and clinical outcomes were observed between the treatment groups at 12 and 24 months.21 Together, these data suggest that in some patients, TNF inhibitor monotherapy can maintain LDA after the discontinuation of methotrexate.
The combination of adalimumab, a fully human IgG1 antibody specific for TNF-α, and methotrexate demonstrated radiographic, clinical and functional superiority compared with adalimumab or methotrexate monotherapies in patients with early, aggressive RA in the 2-year PREMIER study.2 Furthermore, the results from the 8-year open-label extension (OLE) of PREMIER supported the long-term favourable benefit–risk profile of initial adalimumab and methotrexate therapy in patients with RA.22 23 The objective of this post hoc analysis was to evaluate the ability of adalimumab to maintain treatment target as monotherapy following methotrexate withdrawal by assessing the long-term clinical, functional and radiographic outcomes up to year 3 of PREMIER OLE (year 5 of the study) after withdrawal of methotrexate in patients with RA who attained LDA with adalimumab and methotrexate combination therapy. An additional objective was to identify patient or disease characteristics associated with methotrexate reinitiation after methotrexate withdrawal.
Patients and methods
Study design
The methods and results of the 2-year, randomised, double-blind, multicentre, phase III PREMIER study (NCT00195663) have been published.2 The study was in compliance with the Helsinki Declaration. Briefly, patients with early RA were randomised 1:1:1 to three cohorts to receive monotherapy with adalimumab 40 mg subcutaneously (SC) every other week, monotherapy with oral methotrexate initiated at 7.5 mg weekly and rapidly increased up to 20 mg by week 8 or a combination of adalimumab 40 mg every other week and oral methotrexate up to 20 mg weekly. At year 2, all patients who completed the PREMIER study were eligible to enter the OLE to receive open-label adalimumab 40 mg SC every other week for up to an additional 8 years.22 Open-label methotrexate up to 20 mg weekly could be added to the treatment regimen at any time at the investigator’s discretion. This analysis evaluated long-term clinical, functional and radiographic outcomes up to year 3 of the OLE (year 5 of the study); this time point was chosen as the cut-off due to low patient numbers remaining in the study beyond OLE year 3, irrespective of methotrexate use.
Patients
Adult patients (≥18 years old) were enrolled at 133 sites in Australia, Europe and North America. The PREMIER inclusion and exclusion criteria have been previously reported.2 The main inclusion criteria were a diagnosis of RA as defined by the 1987 revised American College of Rheumatology criteria and a disease duration <3 years, plus a swollen joint count ≥8 out of 66 assessed joints, a tender joint count ≥10 out of 68 assessed joints, an erythrocyte sedimentation rate ≥28 mm/hour or C reactive protein (CRP) ≥1.5 mg/dL. Patients were also required to be either rheumatoid factor positive or have at least one joint erosion. Patients were excluded if they had received prior treatment with methotrexate, cyclophosphamide, ciclosporin, azathioprine, >2 other DMARDs or a prednisone equivalent >10 mg/day within 30 days of screening.
Efficacy assessments
Clinical and functional responses were assessed at regular intervals throughout the OLE (every 12 weeks during OLE year 1 and every 16 weeks between OLE years 1 and 3). Clinical outcomes were assessed using the 28-joint Disease Activity Score using C reactive protein (DAS28(CRP)). Patients were considered to have reached LDA if they achieved a DAS28(CRP) score <3.2; achievement of DAS28(CRP) score <2.6 was also assessed. Physical function was determined through the Disability Index of the Health Assessment Questionnaire (HAQ-DI). Normal physical function was defined as HAQ-DI score <0.5. Joint damage was assessed via radiography by independent readers who were blinded to patient, treatment and sequence; readers scored images for joint damage at study baseline and years 2, 3 and 5 of the study using the modified total Sharp score (mTSS; range, 0–398). Radiographic non-progression was defined as mean change from year 2 through 5 (OLE years 0 through 3) in mTSS (ΔmTSS) of ≤0.5 units. Joint erosion, joint space narrowing, Patient Global Assessment and Physician Global Assessment (PGA) from year 2 through 5 (OLE years 0 through 3) were also measured.
Safety
Treatment-emergent AEs were defined as any AE with an onset on or after the first dose of open-label study drug up to 70 days after the last dose or 1825 days from the first dose (ie, from OLE years 0 through 3).
Statistical methods
This post hoc analysis included data from patients treated with adalimumab+methotrexate during the 2-year blinded study who reached at least an LDA state at year 2 of the study and either received open-label adalimumab as monotherapy up to OLE year 3 (methotrexate non-use) or reinitiated methotrexate therapy at some point between OLE years 0 and 3 (methotrexate use). LDA rather than DAS28(CRP) <2.6 was selected as a measure of clinical response to allow for sufficient numbers of patients achieving a favourable outcome from which to evaluate methotrexate withdrawal. Mean DAS28(CRP) as well as the percentages of patients with scores <3.2 (LDA) or <2.6 were summarised by visit. Mean HAQ-DI and the percentage of patients having normal physical function (HAQ-DI <0.5) were summarised by visit.
The percentages of patients who remained in LDA, achieved DAS28(CRP) <2.6 or had normal physical function at OLE year 3 were summarised using non-responder imputation (NRI) based on the population entering the OLE (normalised NRI analysis) and as observed for patients with data available at OLE year 3. The mean ΔmTSS was summarised as observed; the proportion of patients with radiographic non-progression from OLE years 0 through 3 was summarised by NRI and as observed. Kaplan-Meier analysis was used to assess the time to first methotrexate dose during the OLE. Propensity score matching method was used to identify variables significantly associated with methotrexate reinitiation during the OLE while accounting for patient characteristics at the start of OLE. A logistic regression analysis, with methotrexate use (yes/no) as the response and demographic and year 2 (OLE year 0) disease characteristics (eg, gender, RA duration, study duration, year 2 DAS28(CRP) and year 2 PGA) as the predictors, was used to calculate a propensity score for each patient, which represents the predicted probability of reinitiating methotrexate for each patient given the characteristics at the start of OLE. For each patient who reinitiated methotrexate (ie, ‘case’), corresponding ‘control(s)’ (ie, patients who did not reinitiate methotrexate) with similar propensity scores (ie, within 0.01) were identified. Disease characteristics at the time of methotrexate initiation were compared between the propensity score matched ‘cases’ and ‘controls’, and a logistic regression analysis was performed on these matched patients to identify variables at the time of methotrexate initiation that were significantly associated with methotrexate reinitiation during the OLE.
For the safety analysis, the number and percentage of patients with treatment-emergent AEs and events per 100 patient-years (PYs) were reported for patients in the methotrexate use and methotrexate non-use groups.
Results
Patient disposition
Of the 183 patients treated with adalimumab+methotrexate who enrolled in the OLE, 140 (77%) were in an LDA state at year 2 and initiated adalimumab monotherapy in the OLE (figure 1). Of these patients, 84 (60%) continued to receive adalimumab as monotherapy (methotrexate non-use) and 56 (40%) reinitiated methotrexate (methotrexate use) during the OLE. A total of 60 patients in the methotrexate non-use (71%) and 44 in the methotrexate use (79%) groups completed 3 years in the OLE. At OLE year 3, 32 patients (73%) in the methotrexate use group were still receiving methotrexate. In both groups, AEs were the most frequently cited reason for study discontinuation (figure 1); no single AE leading to discontinuation was reported in more than one patient. No patients in the methotrexate non-use group (through OLE year 3) withdrew from the study because of loss of efficacy (figure 1).
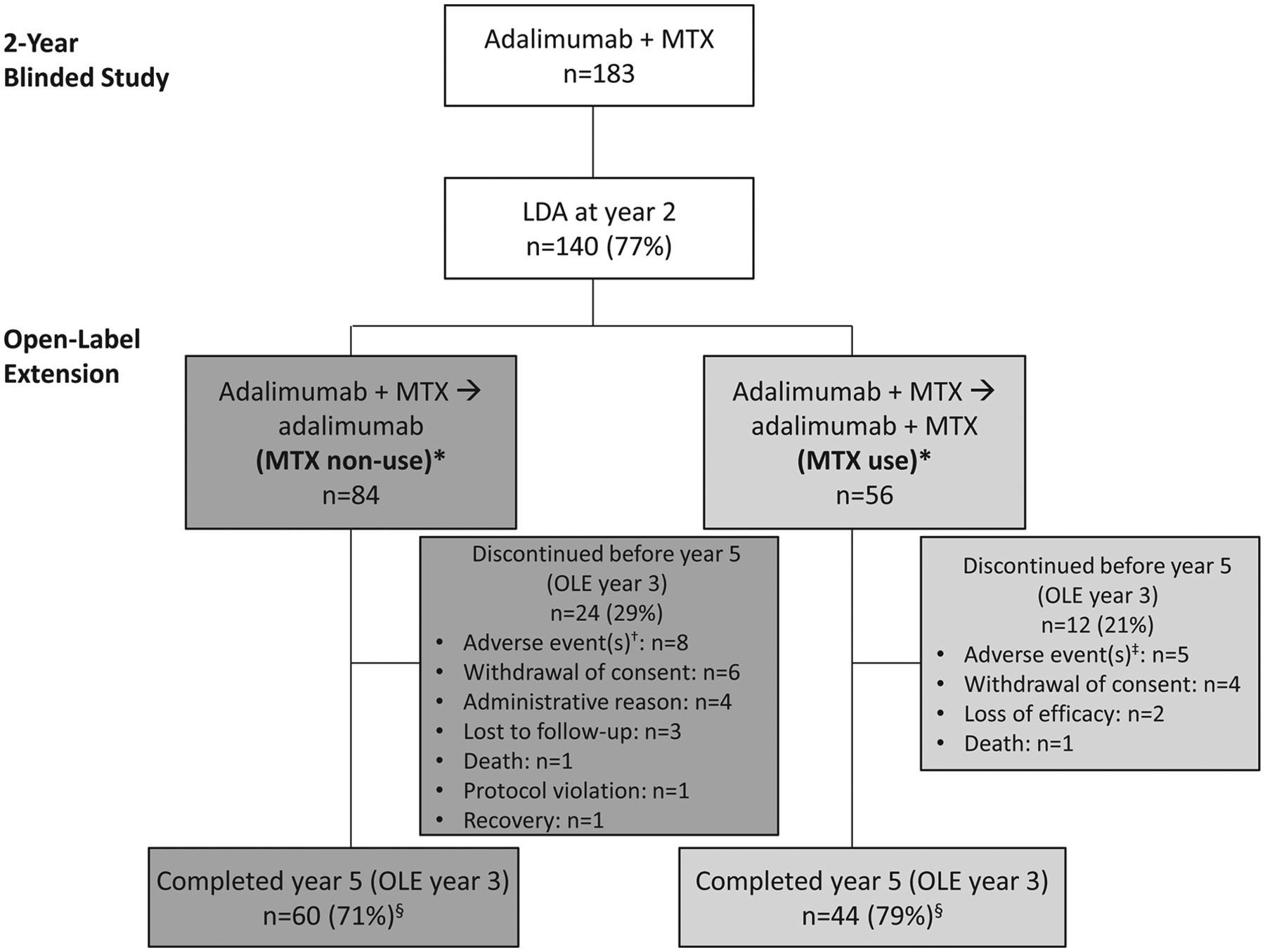
Patient disposition of responders to adalimumab+methotrexate at year 2 (OLE entry) from the primary study who were in methotrexate non-use or use groups during the OLE. AE, adverse event; ELISA, enzyme-linked immunosorbent assay; LDA, low disease activity; MTX, methotrexate; OLE, open-label extension. *Patients entering the OLE received open-label adalimumab 40 mg every other week and could receive MTX at the investigator’s discretion. †In the MTX non-use group, eight patients discontinued because of AEs (stage III malignant melanoma (n=1); squamous cell carcinoma of the tongue (n=1); mycobacterium marinum skin infection (n=1); mycobacterium avium complex infection (n=1); cholecystitis and gastric adenocarcinoma (n=1); alternations of cardiac rhythm (n=1); psoriasis-like eczema and severe bone marrow puncture due to lymphocytosis (n=1) and anaemia, fever and aortic valve endocarditis (n=1). ‡In the MTX use group, five patients discontinued because of AEs (cognitive impairment and a positive ELISA test (n=1); neutropenia (n=1); dyspnoea on exertion (n=1); nasal ulcer (n=1) and atrial fibrillation, encephalopathia, Gram-negative sepsis, septic shock, multiorgan failure, haemophagocytic syndrome, respiratory insufficiency, melena and Epstein-Barr virus infection (n=1). §Reflects the percentages of year 2 LDA responders who were in MTX non-use or use groups during the OLE and completed OLE year 3 (year 5 of the study).
Baseline demographics and clinical characteristics
Baseline demographics and disease characteristics at the time of randomisation were generally similar between patients in the methotrexate use and non-use groups (table 1). A higher proportion of methotrexate non-use patients had prior DMARD and baseline corticosteroid use compared with methotrexate use patients, whereas a higher percentage of methotrexate use patients were women. Although numeric differences existed in disease characteristics at year 2 (OLE entry) between the methotrexate use and non-use populations (table 1), none of the year 2 characteristics examined predicted methotrexate use during the OLE. However, when patients were stratified by age, older patients were more likely to use methotrexate than younger patients. For example, while methotrexate use was similar for patients <50 years versus those ≥50 years (28/70 (40%) vs 28/70 (40%)), those <65 years were less likely to use methotrexate than those ≥65 years (40/112 (36%) vs 16/28 (57%)). Among the methotrexate non-use patients, the last mean methotrexate weekly dose during the double-blind period was 17.5 mg (range 7.5–20 mg). Similarly, among the methotrexate use patients, the last mean methotrexate weekly dose during the double-blind period was 17.3 mg (range 7.5–20 mg); whereas the mean dose at reinitiation was 12.4 mg (range 2–20 mg).
Baseline and year 2 (OLE entry) demographic and disease characteristics in the randomised PREMIER study for patients in the adalimumab+methotrexate cohort who achieved LDA at year 2 and enrolled in the OLE study
Long-term outcomes for the methotrexate use population
Nearly half of the 56 methotrexate use patients (46%; n=26) reinitiated methotrexate within 4 weeks of entry into the OLE study (online supplementary figure 1). The median (IQR) time to first methotrexate use was 5.1 (0.1–31.4) weeks. Among patients who reinitiated methotrexate at some point during the study, disease activity characteristics before reinitiation were worse for patients who reinitiated at later time points versus those who reinitiated within 4 weeks of entry into the OLE (table 2).
Supplemental material
Demographic and disease characteristics from visit immediately before methotrexate reinitiation in patients who reinitiated methotrexate within 4 weeks of entry into the OLE and those who reinitiated at a later time point
Comparing methotrexate users with non-users (matched controls), both objective and subjective measures of inflammation and disease activity were generally higher for the methotrexate users at the time of methotrexate reinitiation (figure 2A). Of these measures, a higher PGA appeared to be associated with methotrexate use during the OLE (p<0.01; figure 2B). When the propensity score analysis was repeated using the same model but with the subset of patients who either did not reinitiate methotrexate or who reinitiated at or after week 4 (patients who reinitiated methotrexate before week 4 were excluded), the results were similar, with PGA still the only variable significantly associated with methotrexate use (online supplementary figure 2).

Association of disease parameters at the time of methotrexate reinitiation during the OLE based on propensity score matching. (A) Mean values for the indicated disease parameters at the time of MTX reinitiation (MTX use) versus matched controls (MTX non-use); (B) ORs (95% CIs) of MTX reinitiation for the indicated disease parameters. CRP, C reactive protein; MTX, methotrexate; OLE, open label extension; PGA, Physician Global Assessment; PtGA, Patient Global Assessment; SJC66, swollen joint count based on 66 joints; TJC68, tender joint count based on 68 joints. *One case (MTX use) could have multiple matched controls (MTX non-use); two of 56 MTX use patients had no matches, so total cases=54. †P<0.01.
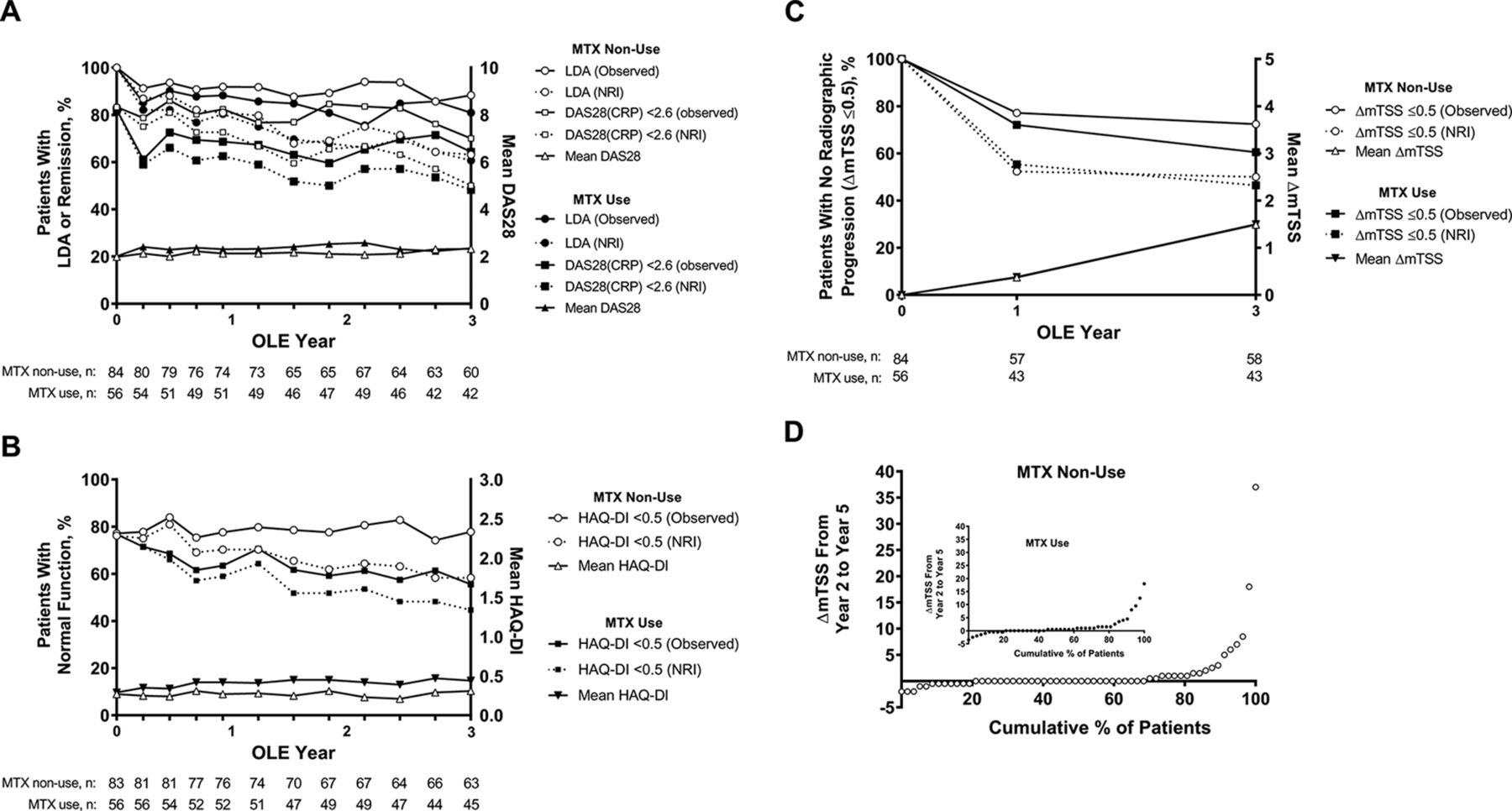
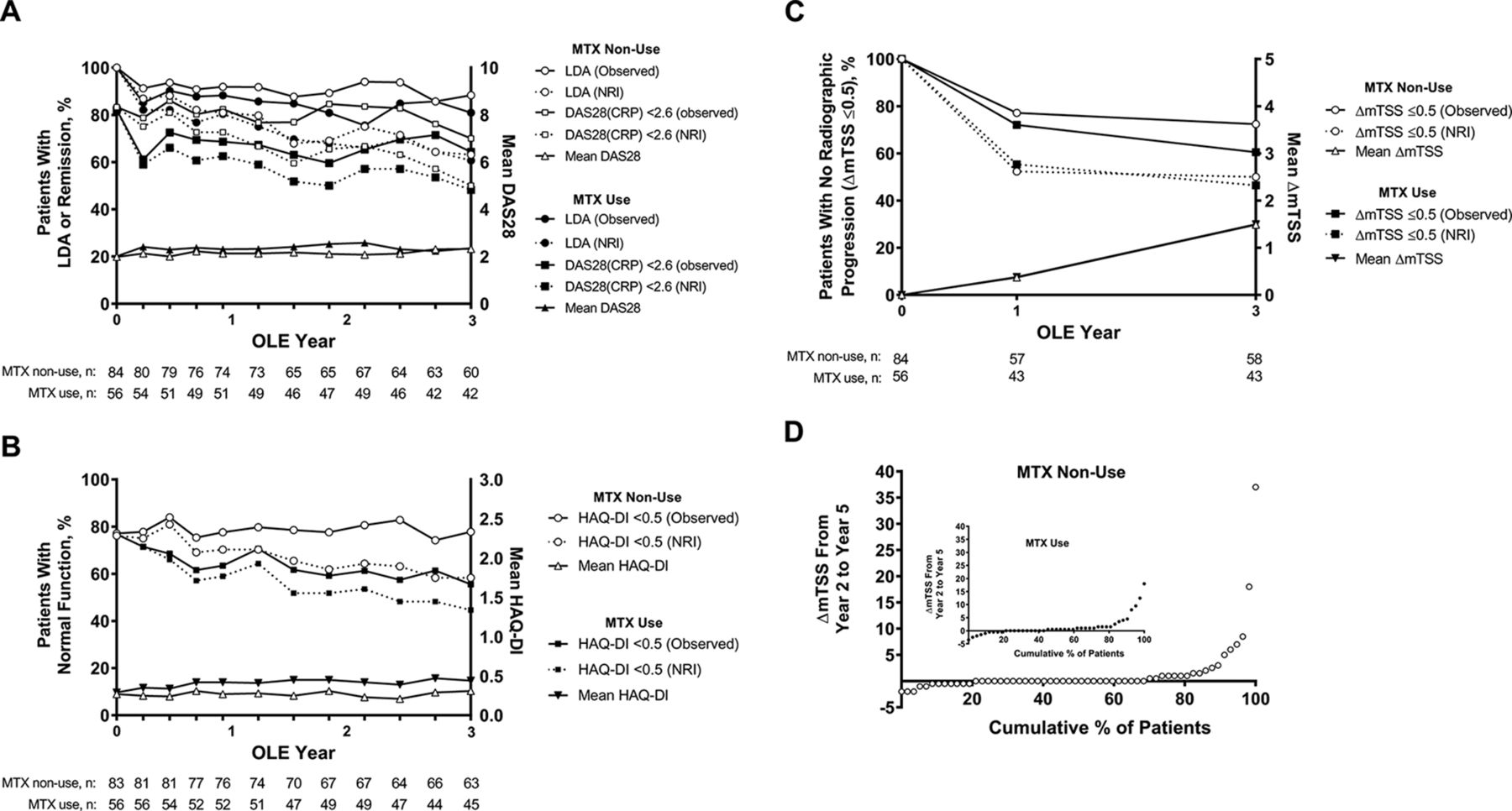
Of the methotrexate use patients, 61% (34/56) retained LDA status at OLE year 3 and 48% achieved DAS28(CRP) <2.6 (27/56; NRI data), as did 81% (34/42) and 64% (27/42) of patients, respectively, with year 3 OLE data available (observed data; figure 3A). In addition, 45% (25/56) of methotrexate use patients had normal physical function, and 46% (26/56) had no radiographic progression at OLE year 3 (NRI data; figure 3B,C). Radiographic outcomes were evaluated with cumulative probability plots of ΔmTSS from OLE years 0 through 3 (years 2 through 5); the cumulative probability for the methotrexate use population is shown in figure 3D.
{kind=link}
{kind=link}
{kind=link}
Clinical, functional and radiographic outcomes following up to 3 years of open-label adalimumab as monotherapy after 2 years of adalimumab+methotrexate. (A) Percentages of MTX non-use and MTX use patients with remission (DAS28(CRP)<2.6) and LDA (left y-axis) and mean DAS28(CRP) score (right y-axis); (B) percentages of MTX non-use and MTX use patients with normal physical function measured as HAQ-DI <0.5 (left y-axis) and mean HAQ-DI score (right y-axis); (C) percentages of MTX non-use and MTX use patients with radiographic non-progression (ΔmTSS ≤0.5; left y-axis) and mean ΔmTSS score (right y-axis); (D) cumulative probability of ΔmTSS from OLE entry to OLE year 3 (study years 2–5) for the MTX non-use and MTX use (inset) populations. Percentage of patients reported for each time point as observed (solid lines) or NRI (dashed lines). Due to missing assessments, the change in mTSS from OLE entry to year 3 was calculated for only 58 and 43 patients in the methotrexate non-use and use groups, respectively. CRP, C reactive protein; DAS28(CRP), 28-joint Disease Activity Score using CRP; HAQ-DI, Disability Index of the Health Assessment Questionnaire; LDA, low disease activity; ΔmTSS, change in modified total Sharp score; MTX, methotrexate; NRI, non-responder imputation; OLE, open-label extension.
Long-term outcomes for methotrexate non-use patients
Similar to methotrexate use patients, the majority of methotrexate non-use patients (63%; 53/84) who entered the OLE from an LDA state retained this state at OLE year 3 (NRI data), as did 88% (53/60) of patients with OLE year 3 data available (observed data; figure 3A). Furthermore, 50% (42/84) of the methotrexate non-use patients achieved DAS28(CRP) <2.6 at the end of year 5, as did 70% (42/60) of patients with year 3 OLE data available. In addition, 58% of methotrexate non-use patients (49/84) had normal physical function, and 50% (42/84) had no radiographic progression at OLE year 3 (NRI data; figure 3B,C). The cumulative probability of ΔmTSS from OLE years 0 through 3 for the methotrexate non-use population is shown in figure 3D.
Safety
In general, the incidence of treatment-emergent AEs (89.3% and 92.9%) and the rates of AEs (255.9 and 267.1 PYs) were similar between the methotrexate non-use and use groups, respectively (table 3). The rate of AEs leading to discontinuation and infectious AEs were numerically higher in the methotrexate use group. Three malignancies (other than lymphoma, leukaemia, non-melanoma skin cancer or melanoma) were reported in the methotrexate non-use group, whereas none were reported in the methotrexate use group. Three non−treatment related deaths occurred during the study (methotrexate non-use, n=1 (coronary artery occlusion); methotrexate use, n=2 (Epstein-Barr virus infection and myocardial infarction)). There were no cases of tuberculosis (active or conversion), reactivation of hepatitis B, progressive multifocal leucoencephalopathy, demyelinating disorder, hepatosplenic T-cell lymphoma, lupus-like reaction or systemic lupus erythematosus, Stevens-Johnson syndrome or erythema multiforme reported in either group.
Overview of treatment-emergent AEs and rates of AEs per 100 PYs between OLE entry and year 3 (years 2 and 5 of the study)
Discussion
Combination therapy with a TNF inhibitor and methotrexate in patients with RA is effective in suppressing inflammation, reducing disease progression and improving physical function compared with methotrexate monotherapy.8–13 Ideally, once clinical goals are achieved with combination therapy, the number of medications should be reduced to promote adherence and reduce the risk of AEs. Treatment recommendations suggest first tapering corticosteroids, then tapering biologic DMARDs before considering the discontinuation of csDMARDs; however, patient preference or intolerance may necessitate discontinuation of csDMARDs.1
This post hoc analysis of the PREMIER extension study aimed to evaluate the ability of a TNF inhibitor to maintain treatment target as monotherapy following methotrexate withdrawal. Our results indicated that adalimumab monotherapy was effective in maintaining clinical, functional and radiographic outcomes for up to 3 years after withdrawal of methotrexate in the majority of patients who attained LDA with adalimumab+methotrexate therapy at year 2. Of the patients with OLE year 3 data available, 88% retained LDA and 70% achieved DAS28(CRP) <2.6 with adalimumab monotherapy. Similar rates of retaining LDA status and achieving DAS28(CRP) <2.6 were observed in methotrexate use and non-use patients. However, more methotrexate non-use patients had normal physical function and radiographic non-progression than patients who reinitiated methotrexate. Rates of AEs were similar between the methotrexate non-use and use patients.
There are limited data regarding patient outcomes after withdrawing methotrexate from combination therapy with TNF inhibitors. In one randomised non-inferiority study, patients who received initial etanercept+methotrexate combination therapy for 6 months were then randomised to etanercept monotherapy or etanercept+methotrexate therapy. Patients who achieved LDA at 6 months maintained LDA to month 12 whether they received etanercept monotherapy or etanercept+methotrexate.24 Our findings are supported by those of Keystone et al, in which patients who had achieved LDA at 6 months with initial etanercept+methotrexate combination therapy and then received etanercept monotherapy or etanercept + methotrexate therapy had similar radiographic and clinical outcomes at 12 and 24 months.21 These findings support the discontinuation of methotrexate in patients treated with a TNF inhibitor+methotrexate combination who achieve LDA or DAS28(CRP) <2.6. The findings from the Combination of Methotrexate and Etanercept in Active Early Rheumatoid Arthritis (COMET) study were less consistent. No statistically significant differences were observed in clinical remission (DAS28 <2.6) between patients receiving combination etanercept+methotrexate treatment for 2 years compared with patients receiving combination treatment in the first year followed by etanercept monotherapy in the second year; however, a significantly greater proportion of patients in the combination group achieved radiographic non-progression compared with patients in the etanercept monotherapy group.25
Nearly half of methotrexate use patients in the present OLE study reinitiated methotrexate within 4 weeks of starting adalimumab monotherapy after methotrexate withdrawal. This could be due to methotrexate postcessation flares or investigator/patient to reinitiate therapy preference (including possible nocebo effect) and not necessarily due to failure of adalimumab monotherapy. Tapering methotrexate in some of the patients treated with adalimumab+methotrexate during the 2-year blinded study may have improved outcomes in the methotrexate non-use group.
The ability of the PGA, but not disease parameters, such as tender joint count and swollen joint count, to associate with the use of methotrexate was of significance. An analysis of data from the Canadian Early Arthritis Cohort (CATCH) cohort study indicated that in patients with RA, PGA scores at 3 months were a predictor of DAS28(CRP) <2.6 at 12 months; however, so were tender joint counts and swollen joint counts.26
A limitation of the current study was that observations were based on low patient numbers analysed in an open-label setting. Furthermore, methotrexate reinitiation was up to the physician’s discretion, and thus, patients in the methotrexate use group could have been treated with methotrexate for variable amounts of time and for a variety of reasons. Owing to the study design, the results of the methotrexate use group may be affected by indication bias. Additionally, all patients with LDA were required to receive monotherapy at the end of 2 years. This includes patients with DAS28(CRP) <2.6, who might be less likely to add methotrexate.
In conclusion, following attainment of an LDA state at year 2 with the combination of adalimumab+methotrexate treatment, adalimumab monotherapy for up to 3 years permitted at least half of the patients to retain LDA with normal physical function and minimal radiographic progression. Methotrexate withdrawal appears possible for some patients once clinical target has been achieved; however, continuation of combination therapy or tapering of adalimumab may need to be considered for others.
Acknowledgments
The authors thank Shufang Liu for contributing to the statistical analysis. Medical writing assistance was provided by Katie Groschwitz, PhD, and Maria Hovenden, PhD, of Complete Publication Solutions, LLC (North Wales, Pennsylvania, USA), a CHC Group company and was supported by AbbVie. This manuscript was based on work previously presented at the 2012 American College of Rheumatology (ACR) and Association of Rheumatology Health Professionals (ARHP) Annual Meeting and published as a conference abstract.
References
Footnotes
Contributors All authors participated in the interpretation of data, the preparation, review and approval of the manuscript and the decision to submit for publication.
Funding AbbVie funded the study (NCT00195663); contributed to the design; was involved in the collection, analysis and interpretation of the data and in the writing, review and approval of the publication.
Competing interests ECK has received consulting fees or other remuneration from, and served on advisory boards on behalf of, Abbott Laboratories, AstraZeneca Pharma, Biotest, Bristol-Myers Squibb Company, Crescendo Bioscience, F. Hoffmann-La Roche Inc., Genentech Inc., Janssen Inc., Lilly Pharmaceuticals, Merck and Pfizer Pharmaceuticals; has received research grants from Abbott Laboratories, Amgen Inc., AstraZeneca Pharmaceuticals LP, Bristol-Myers Squibb, F. Hoffmann-La Roche Inc., Janssen Inc., Lilly Pharmaceuticals, Novartis Pharmaceuticals, Pfizer Pharmaceuticals and Sanofi-Aventis and has speaker honoraria agreements with Abbott Laboratories, Amgen, AstraZeneca LP, Bristol-Myers Squibb Canada, F. Hoffmann-La Roche Inc., Janssen Inc., Pfizer Pharmaceuticals and Sanofi Genzyme. FCB has received consulting fees or other remuneration from Centocor, Schering-Plough, Amgen/Wyeth and Abbott. HK, YL, IS and SF are employees of AbbVie and may own AbbVie stock and/or stock options.
Patient consent Not required.
Ethics approval A central institutional review board or independent ethics committee approved the study at each participating site.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.