Article Text

Abstract
Objectives To evaluate the effect of certolizumab pegol (CZP) on work and household productivity, and on participation in family, social and leisure activities in patients with axial spondyloarthritis (axSpA), including ankylosing spondylitis (AS) and non-radiographic (nr-) axSpA.
Methods RAPID-axSpA (NCT01087762) was a phase III, double-blind, placebo-controlled trial to week (Wk) 24, dose-blind to Wk48 and open-label to Wk204. A total of 325 patients were randomised 1:1:1 to placebo, CZP 200 mg Q2W or CZP 400 mg Q4W. The validated arthritis-specific Work Productivity Survey assessed the impact of axSpA on work and household productivity and participation in social activities during the preceding month. Data are shown to Wk96, with responses compared between treatment arms (placebo vs CZP 200 mg and 400 mg dose groups combined) and subpopulations using a non-parametric bootstrap-t method.
Results At baseline, 63.2% of placebo and 72.0% of CZP patients were employed. By Wk24, CZP patients reported on average 1.0 fewer days of absenteeism and 2.6 fewer days of presenteeism per month, compared with 0.4 and 0.9 fewer days for placebo. At home, by Wk24, CZP patients reported on average 3.0 household work days gained per month versus 1.3 for placebo. CZP patients reported fewer days with reduced household productivity or days lost for social participation. Similar improvements were observed in AS and nr-axSpA subpopulations and improvements with CZP were maintained to Wk96.
Conclusions Compared with placebo, treatment with CZP significantly improved work and household productivity and resulted in greater social participation for patients with axSpA, which could lead to considerable indirect cost gains.
Trial registration number NCT01087762.
- ankylosing spondylitis
- anti-TNF
- autoimmune diseases
- TNF-alpha
- treatment
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Results from previous studies suggest that antitumour necrosis factor agents can improve work productivity in patients with axial spondyloarthritis (axSpA).
What does this study add?
Compared with placebo, patients treated with certolizumab pegol (CZP) improved productivity at the workplace and participation in household and social activities.
Similar improvements were seen in patients both with and without radiographic sacroiliitis.
Rapid improvements were seen from week 4 and maintained over 2 years.
How might this impact on clinical practice?
Consistent with the clinical improvements seen in response to CZP treatment in patients with axSpA, these results indicate that CZP is a valuable therapeutic option, and increased productivity and social participation may help to improve patients’ quality of life.
Introduction
Axial spondyloarthritis (axSpA) is a chronic inflammatory condition, characterised by axial joint inflammation, in particular the sacroiliac (SI) joints. Back pain is the primary symptom, often accompanied by peripheral and extra-articular manifestations.1 2 Within the broad spectrum of axSpA is ankylosing spondylitis (AS), defined by radiographic changes in the SI joints.3 Patients without definitive radiographic sacroiliitis, but with evidence of sacroiliitis from MRI or HLA-B27, combined with other SpA features, have been classified as having non-radiographic (nr-) axSpA.3 4
There is evidence of similar disease burden in AS and nr-axSpA,1 emphasising the need to treat both patient subpopulations.5–7 Employment status and work productivity are severely influenced by AS,8 and patients ranked ‘impact on work’ as the area of their life most affected by their condition.9 Work disability is one of the major outcomes of AS, with increased absence from work and reduced productivity at work.10 However, the impact of the entire spectrum of axSpA on employment status, workplace and household productivity is poorly researched,10–12 and there are only limited data available concerning how the disease affects specific aspects of daily living.13–16 Nevertheless, results from studies with antitumour necrosis factor (anti-TNF) agents have suggested that these biologic treatments can improve work productivity in patients with axSpA.17–19
The efficacy and safety of certolizumab pegol (CZP), an Fc-free, PEGylated anti-TNF agent, in patients with axSpA has been investigated and reported over 4 years in the RAPID-axSpA trial (NCT01087762).20–22 Here, we report the effects of CZP treatment on paid work and household productivity, and daily activities in patients with axSpA, including AS and nr-axSpA, to week 96.
Methods
Patient population
The RAPID-axSpA trial (NCT01087762) randomised 325 patients aged ≥18 years with chronic back pain of ≥3 months, fulfilling the Assessment of SpondyloArthritis International Society (ASAS) criteria for axSpA.3 Detailed inclusion and exclusion criteria have been reported previously.20 Patients were stratified according to the presence of radiographic sacroiliitis into AS (patients meeting the modified New York criteria) and nr-axSpA subpopulations. Recruited patients had active disease (Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) ≥4, with spinal pain ≥4 (0–10 Numerical Rating Scale), and C reactive protein above the upper limit of normal (>7.9 mg/L)) and must have been intolerant of, or responded inadequately to, ≥1 non-steroidal anti-inflammatory drug. Patients previously treated with >1 prior anti-TNF or who were primary anti-TNF failures (no response within the first 12 weeks of treatment) were excluded.
Study design
RAPID-axSpA was a phase III, multicentre study in patients with axSpA. Trial design details are reported elsewhere.20 In brief, the study was placebo-controlled to week 24, dose-blind to week 48 and open-label to week 204. Patients were randomised 1:1:1 to placebo or CZP 400 mg at weeks 0, 2 and 4 (loading dose), followed by either CZP 200 mg every 2 weeks (Q2W) or CZP 400 mg every 4 weeks (Q4W).20 The clinical primary outcome was ASAS20 response at week 12.20 23 In the current manuscript, we present data up to week 96.
The study was approved by a national, regional or independent ethics committee or institutional review board at participating sites, and was conducted in accordance with applicable regulatory and International Conference on Harmonisation Good Clinical Practice requirements, based on the declaration of Helsinki and local laws. All patients provided written informed consent prior to any protocol-specific procedures being performed.
Work Productivity Survey
The Work Productivity Survey (WPS) is a validated questionnaire assessing the impact of arthritis on patient productivity in the workplace and at home, and on participation in family, social and leisure activities.24 The WPS has demonstrated discriminant validity, responsiveness to clinical changes and reliability in rheumatoid arthritis (RA),24 psoriatic arthritis (PsA)25 and axSpA.15
The WPS is self-reported, but interviewer administered, with a 1-month recall period. The first question addresses employment status and provides information on job type for employed patients (non-manual, manual with no supervisory duties or mixed) and on the status of those not employed. For employed patients, three questions relate to work productivity outside the home. These assess, over the past month, absenteeism (full days of work missed due to axSpA); presenteeism (days with work productivity reduced by ≥50% due to arthritis); and the level of arthritis interference on work productivity (0–10 scale; 0=no interference, 10=complete interference).
All patients, regardless of employment status, answer five questions about household work and daily activities. These questions assess, over the previous month, the number of days with no household work performed due to arthritis; days with household productivity reduced by ≥50% due to arthritis; days with outside help hired; days with family, social or leisure activities missed; and the level of arthritis interference with household productivity (0–10 scale; 0=no interference, 10=complete interference). The WPS was completed at the study baseline and every subsequent 4 weeks.
Statistical analysis
Data for the initial 24-week double-blind, placebo-controlled period were analysed using the Full Analysis Set (FAS) to align with the reporting of clinical data over the same study period.20 The FAS included all randomised patients who received ≥1 dose of study medication and had valid baseline and post-baseline measurements for the primary outcome. The FAS consisted of all patients randomised, minus one placebo patient.
Data for the dose-blind and early open-label treatment periods (week 24 to week 96) were analysed using all patients randomised to receive CZP from week 0, as aligned with the reporting of week 96 clinical outcomes.21 All analyses were conducted in the overall axSpA, AS and nr-axSpA populations. Data from the CZP 200 mg Q2W group and CZP 400 mg Q4W group were combined.
The WPS questions relating to workplace productivity were analysed only for patients who were employed at the respective visit, whereas questions assessing household productivity were analysed for all patients. Mean WPS responses to week 24 were compared between treatment arms using a non-parametric bootstrap-t method (a 5% statistical significance level was used). Missing data were imputed using last observation carried forward.
Additional post hoc analyses were conducted to calculate the frequency distribution of the WPS scores at specific visits and the cumulative gains over the placebo-controlled 24-week period. Cumulative productivity scores were derived for each treatment group by summing productivity scores to week 24, starting at week 4. Cumulative gains were derived as the total difference in gains between the CZP treatment and placebo groups and are presented over the 6-month period.
Results
Baseline characteristics
A total of 325 patients were randomised to placebo (n=107), CZP 200 mg Q2W (n=111) or CZP 400 mg Q4W (n=107); 298 (91.7%) patients completed the 24-week, double-blind phase of the RAPID-axSpA study. Of the 218 CZP-randomised patients, 203 (93.1%) completed to week 24, 191 (87.6%) to week 48 and 174 (79.8%) to week 96.
Baseline characteristics for the overall axSpA population were generally similar between treatment groups. For AS and nr-axSpA subpopulations, expected differences were observed in age, gender and disease duration: mean (SD) age of the patients with AS was 41.5 (11.6), of patients with nr-axSpA 37.4 (11.8), 72.5% of patients with AS and 48.3% of patients with nr-axSpA were men, median symptom duration was 9.1 years in patients with AS (range 0.3–50.9) and 5.5 years in patients with nr-axSpA (0.3–41.5).20
Burden of disease on workplace and household productivity at baseline
A total of 63.2% of the patients in the placebo group and 72.0% of patients in the CZP treatment groups were employed at study baseline (online supplementary figure S1A). Employment outside the home was 69.1% for the overall axSpA population, with 12.3% unable to work due to arthritis (online supplementary figure S1B). More patients with nr-axSpA than AS (71.2% vs 67.4%, respectively) were employed outside the home, whereas more patients with AS (15.7%) than nr-axSpA (8.2%) were unable to work due to arthritis. Also, 5.6% of all patients with axSpA were retired (online supplementary figure S1B).
Supplementary file 1
The burden of disease at study baseline was high for all patients with axSpA. On average, patients with axSpA reported more than 1 week of paid work (absenteeism and presenteeism) affected by axSpA over the previous month (table 1). The burden of axSpA on household productivity was even greater, with on average more than 2 weeks of household duties and social activities affected over the previous month. The burden of disease on workplace absenteeism and presenteeism, household productivity and social activities was generally higher for patients with nr-axSpA than for patients with AS (table 1).
RAPID-axSpA: burden of axSpA on workplace and household productivity, and employment status at study baseline (Full Analysis Set, observed cases)
Improvements in workplace productivity
Overall axSpA
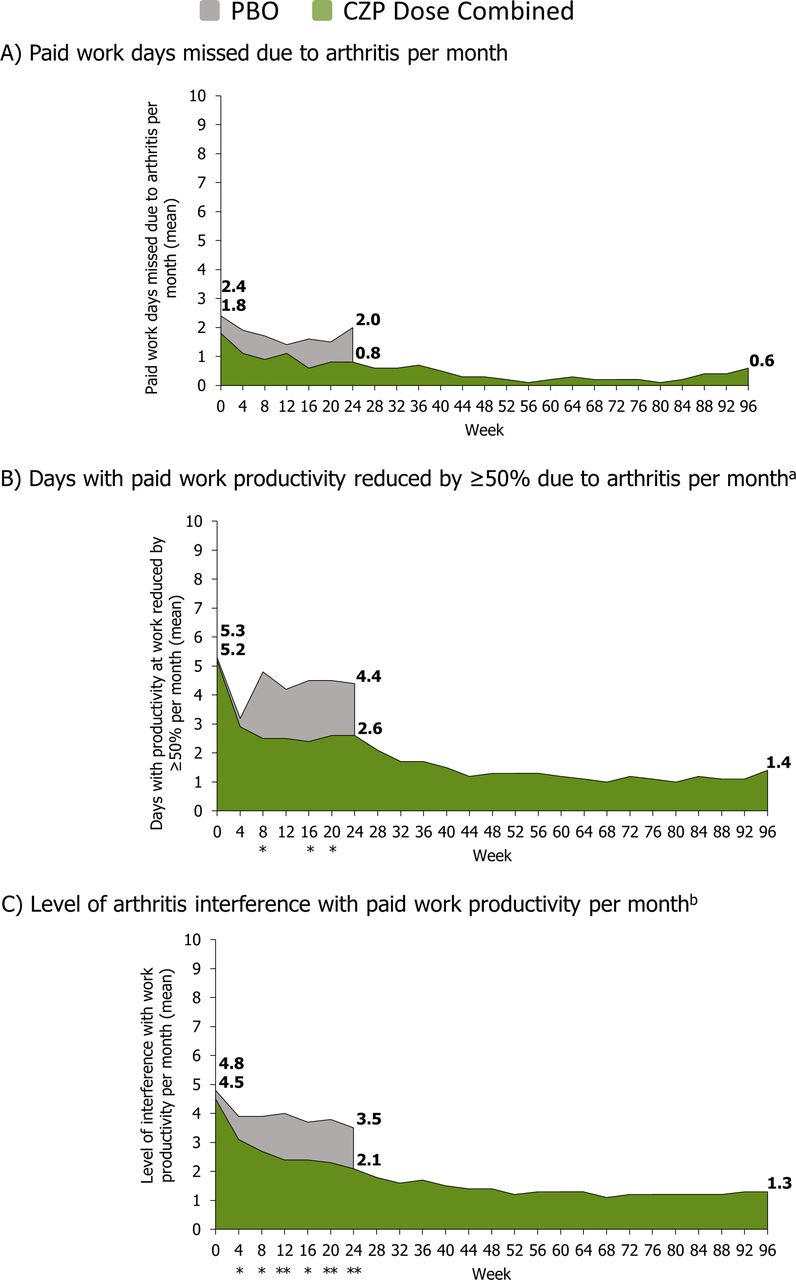
In CZP patients, improvements in workplace productivity were reported as early as week 4 and maintained throughout the placebo-controlled period to week 24 (figure 1). At week 24, CZP patients gained on average 1.0 additional full days of paid work per month and had 2.6 fewer days per month with reduced productivity (figure 1A,B). A significant reduction of axSpA interference with paid work productivity of 2.4 (on a 0–10 scale) was also reported (figure 1C). By comparison, placebo patients gained on average 0.4 work days per month, 0.9 days per month with reduced productivity, and axSpA interference with work decreased by 1.3 (figure 1).
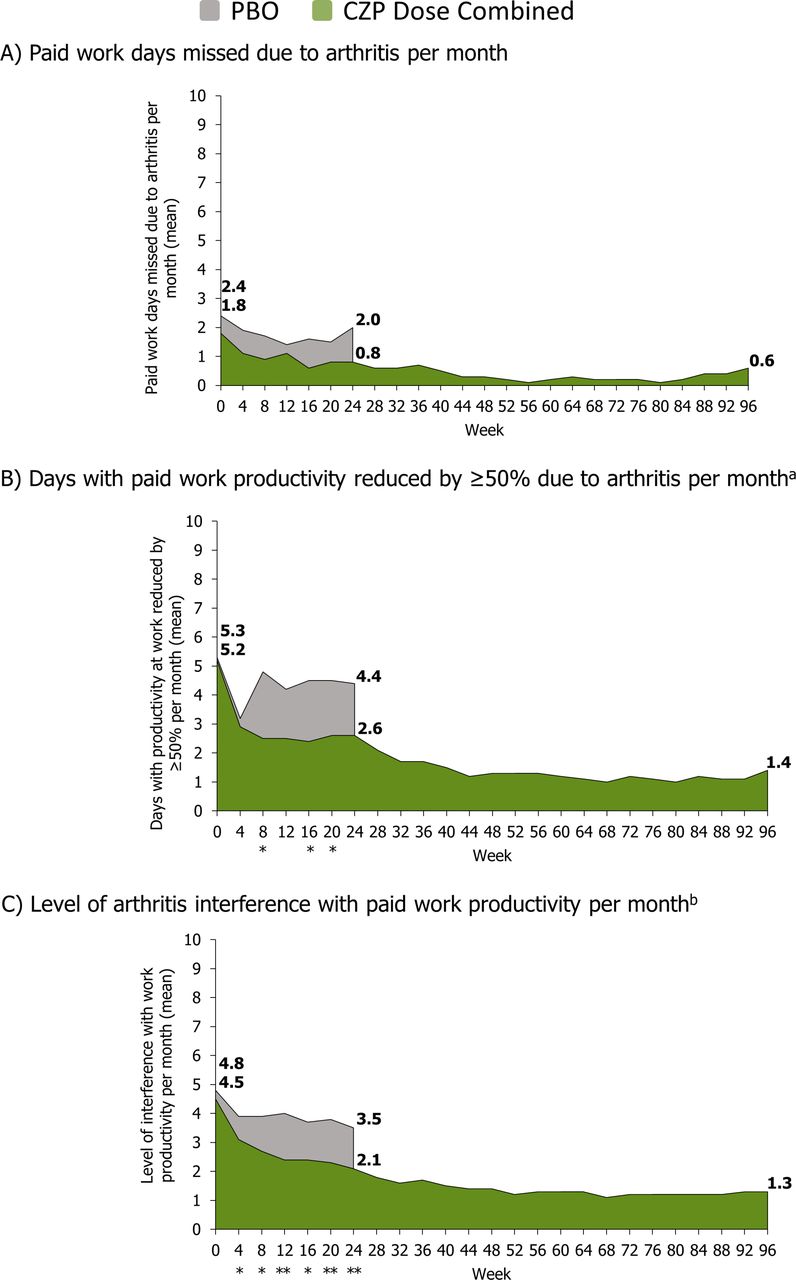
Monthly improvements in paid work productivity: overall axial spondyloarthritis population (employed patients only; last observation carried forward imputation). Assessed using the arthritis-specific Work Productivity Survey. Certolizumab pegol (CZP) data shown for patients randomised to CZP at week 0. *CZP versus placebo (PBO) P<0.05; **CZP versus PBO P<0.001. Non-parametric bootstrap t-test. aDoes not include days counted in previous question (full days missed); b0–10 point scale (0=no interference, 10=complete interference). Number of patients employed: week 0: PBO n=67, CZP n=157; week 96: CZP n=171.
The number of employed patients in the CZP group who did not miss any full days of paid work due to axSpA increased from 68.2% at baseline to 82.0% at week 24 (an increase of 13.8%) compared with an increase from 70.1% to 74.2% (4.1%) in the placebo group. By 96 weeks, a further increase was seen in the CZP group with 90% of employed patients reporting no full days of paid work missed (online supplementary figure S2A).
The number of CZP-treated patients who reported no days with reduced productivity due to axSpA increased from 51.6% to 70.2% (18.6%) from baseline to week 24, compared with 46.3% to 51.5% (5.2%) in the placebo group (online supplementary figure S2). By 96 weeks, 80% of CZP-treated patients reported no days with reduced productivity (online supplementary figure S2B).
In terms of axSpA interference with paid work productivity, 62% of employed patients in the CZP group reported an interference level smaller than 2 (on a 0–10 scale) by week 24, compared with 22% at baseline, a proportion which further increased to 81% by 96 weeks (online supplementary figure S2C). The monthly improvements in workplace productivity reported by CZP-treated patients resulted in mean cumulative gains over the 24 weeks equivalent to a mean 4.8 full days gained of paid work and an additional mean 10.1 days with increased work productivity gained for CZP-treated patients over placebo patients.
The initial improvements observed to week 24 were further continued in CZP-treated patients to week 96, with further reductions seen in the absenteeism and presenteeism due to axSpA, and lower interference of axSpA with work productivity (figure 1A–C).
AS and nr-axSpA subpopulations
Similar improvements in workplace productivity were observed in the AS and nr-axSpA subpopulations by week 24 in CZP-treated patients (figure 2). For patients with AS receiving CZP, absenteeism and presenteeism were reduced on average by 1.0 day and 2.1 days per month at week 24 compared with baseline (placebo: mean decrease of 0.5 and 1.2 days), respectively. For CZP-treated patients with nr-axSpA, absenteeism and presenteeism were reduced on average by 1.0 day and 3.3 days per month compared with baseline (placebo: mean decrease of 0.4 and 0.6 days), respectively (figure 2A,B). The levels of axSpA interference on work productivity decreased on average by 2.4 for CZP patients in both subpopulations, compared with 1.2–1.4 (nr-axSpA; AS) for placebo (figure 2C). Improvements with CZP in both subpopulations were further continued to week 96 (figure 2).
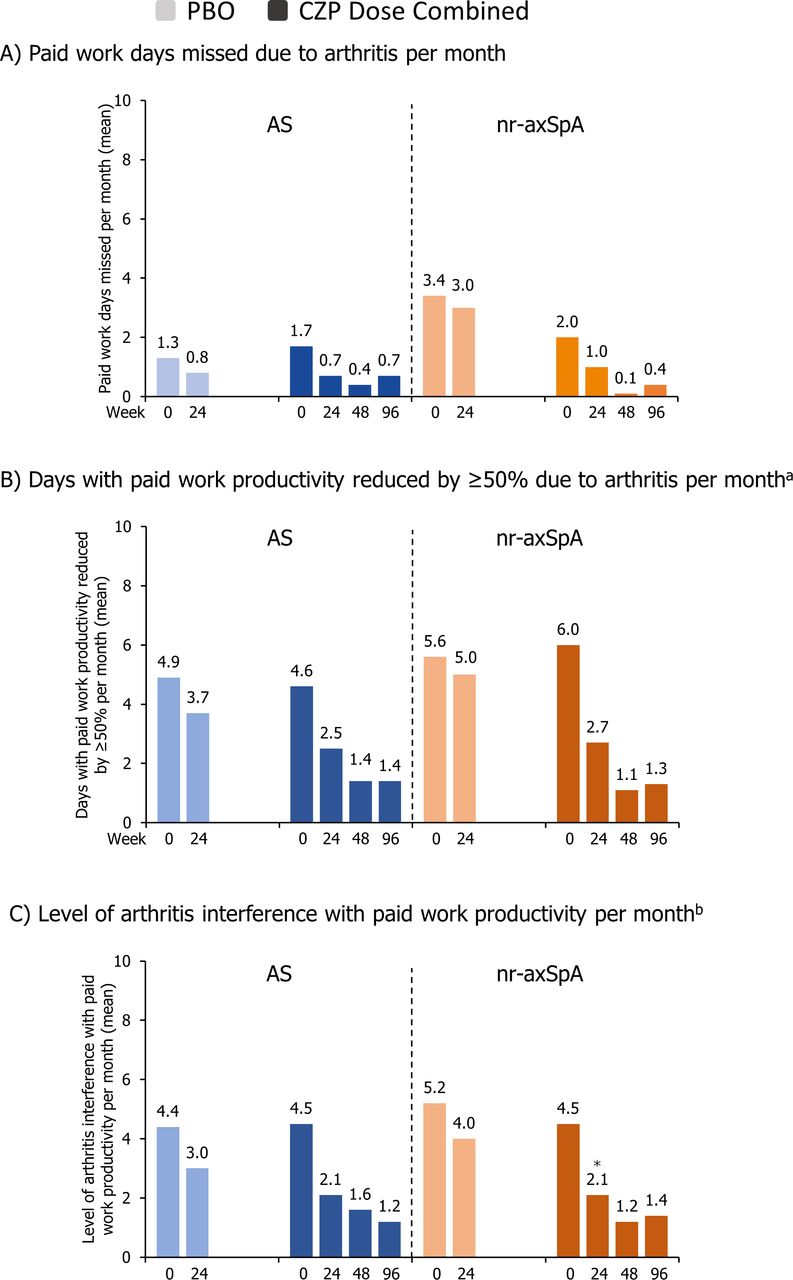
Monthly improvements in paid work productivity: ankylosing spondylitis (AS) and non-radiographic axial spondyloarthritis (nr-axSpA) subpopulations (employed patients only; last observation carried forward imputation). Certolizumab pegol (CZP) data shown for patients randomised to CZP at week 0. *CZP versus placebo (PBO) P<0.05. Non-parametric bootstrap t-test. aDoes not include days counted in previous question (full days missed); b0–10 point scale (0=no interference, 10=complete interference). Number of patients employed: week 0: AS: placebo (PBO) n=31, CZP n=89; nr-axSpA: PBO n=36, CZP n=68; week 96: AS: CZP n=93; nr-axSpA: CZP n=78.
Improvements in household productivity
Overall axSpA
A significant reduction of the impact of arthritis on productivity within the home was achieved in CZP patients as early as week 4 and maintained to week 24 (figure 3). At week 24, CZP-treated patients with axSpA reported on average 3.0 household work days gained per month and 4.2 fewer days per month with reduced household productivity, compared with 1.3 and 1.8 days, respectively, for placebo patients (figure 3A,B). Generally, CZP patients required fewer days of household help per month at week 24 than placebo patients (figure 3C). CZP also significantly reduced the level of interference of axSpA with household activities by 2.5 (on a 0–10 scale) at week 24 in the treatment groups, compared with 0.8 in the placebo group (figure 3D).

Monthly improvements in home productivity: overall axial spondyloarthritis population (last observation carried forward imputation). Assessed using the arthritis-specific Work Productivity Survey. Certolizumab pegol (CZP) data shown for patients randomised to CZP at week 0. Non-parametric bootstrap t-test; *CZP versus placebo (PBO) P<0.05; **CZP versus PBO P<0.001. aDoes not include days counted in previous question (full days missed); b0–10 point scale (0=no interference, 10=complete interference). PBO n=107, CZP n=218.
At week 24, the number of CZP-treated patients with axSpA who did not lose any days of household work increased from 47.2% at baseline to 70.2% by Week 24 (23.0% incremental), compared with an increase from 42.5% to 49.1% (6.6%) in the placebo group. The number of patients who reported fully productive household work days in the CZP group rose from 37.6% at baseline to 61.5% at Week 24 (23.9% incremental), compared with an increase from 34.9% to 38.7% (3.8%) in placebo patients (online supplementary figure S3B). By 96 weeks, further increases were seen, with 78.0% and 73.4% of CZP-treated patients reporting no days of household work missed and fully productive household work days, respectively (online supplementary figure S3A,B). In terms of axSpA interference with household productivity, 61.0% of CZP-treated patients reported an interference level of 2 or less (on a 0–10 scale) by week 24, compared with 24.3% at baseline, a proportion which further increased to 71.5% by week 96 (online supplementary figure S2C). The frequency distribution patterns observed for the number of days with outside help hired was similar (online supplementary figure S3).
The monthly improvements in household productivity reported by CZP-treated patients result in mean cumulative gains in full days of household work and more productive days of household work over placebo were equivalent to 17.4 and 15.4 days, respectively, over the 24-week period.
As with work productivity, improvements in household productivity observed with CZP treatment continued through to week 96 (figure 3). There were sustained improvements in the number of household work days gained per month (week 24: 3.0; week 96: 3.8; figure 3A) and in the number of days with reduced productivity (figure 3B).
AS and nr-axSpA subpopulations
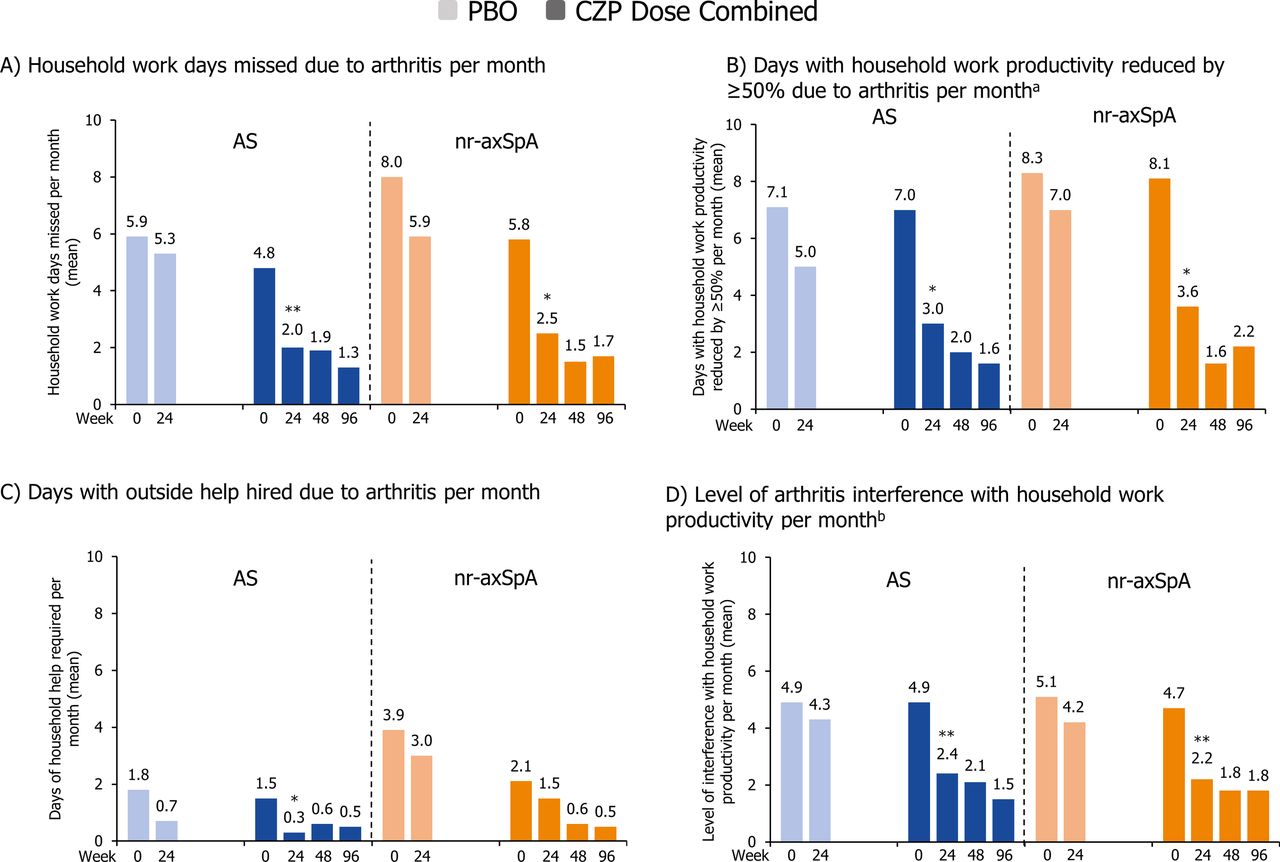
Similar improvements in household productivity were observed in the AS and nr-axSpA subpopulations (figure 4). By week 24, CZP-treated patients with AS reported more household work days gained (on average 2.8 days; placebo: 0.6 days), fewer days with reduced household productivity (on average 4.0 days; placebo: 2.1 days), fewer days with outside help required (1.2 fewer days; placebo: 1.1 days) and a reduction in the level of arthritis interference by 2.5 (placebo: 0.6; on a 0–10 point scale) over the past month (figure 4). Similar improvements were observed in patients with nr-axSpA (on average 3.3 days gained of household work vs 2.1 days for placebo; 4.5 fewer days with reduced household productivity vs 1.3 days for placebo; levels of arthritis interference reduced by 2.5 vs 0.9 for placebo). In both subpopulations, sustained improvements were observed to week 96 (figure 4).
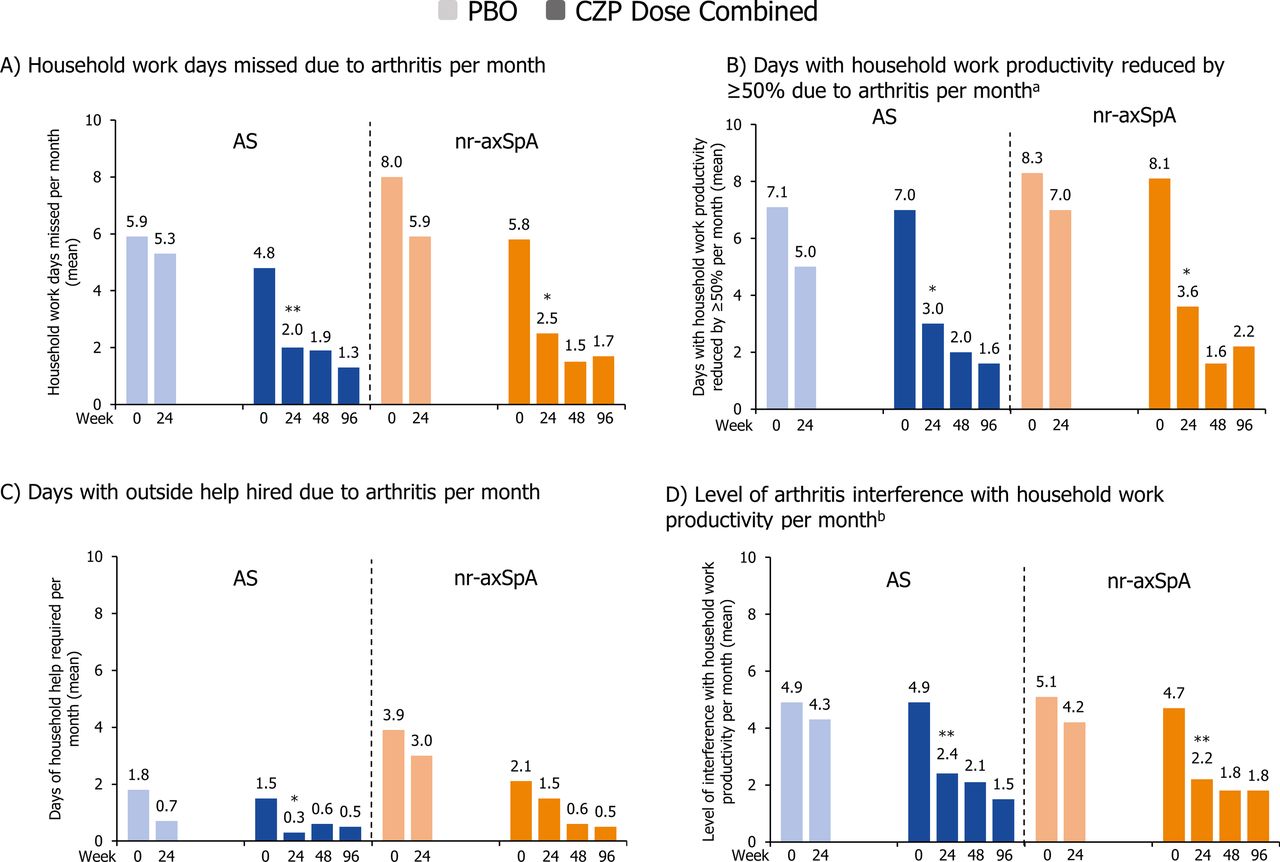
Monthly improvements in home productivity: ankylosing spondylitis (AS) and non-radiographic axial spondyloarthritis (nr-axSpA) subpopulations (last observation carried forward imputation). Assessed using the arthritis-specific Work Productivity Survey. Certolizumab pegol (CZP) data shown for patients randomised to CZP at week 0. *CZP versus placebo (PBO) P<0.05; **CZP vs PBO P<0.001. Non-parametric bootstrap t-test. aDoes not include days counted in previous question (full days missed); b0–10 point scale (0=no interference, 10=complete interference). AS: PBO n=58, CZP n=121; nr-axSpA: PBO n=49, CZP n=97.
Improvements in participation in social, family and daily activities
Overall axSpA
Patients treated with CZP missed significantly fewer days of family, social and leisure activities due to axSpA compared with placebo patients from week 4, improvements which were sustained through the double-blind phase to week 24 and on to week 96 (figure 5). By week 24, CZP patients in the overall axSpA population gained an average of 2.5 days of family, social and leisure activities per month compared with 2.3 days with placebo; for CZP-treated patients, this initial improvement was sustained to 3.2 days by week 96 (figure 5A). The number of CZP-treated patients who did not miss any days of family, social and leisure activities increased from 48.6% at baseline to 76.6% at week 24 (28.0% incremental), compared with an increase from 42.5% to 56.6% (14.1%) in the placebo arm (online supplementary figure S4). In the CZP-treated group, the percentage of patients who did not miss any days of social activities reached 83.0% by 96 weeks of treatment.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Monthly improvements in family, social and leisure activities to week 96 (last observation carried forward imputation). Assessed using the arthritis-specific Work Productivity Survey. Certolizumab pegol (CZP) data shown for patients randomised to CZP at week 0. *CZP versus placebo (PBO) P<0.05; **CZP versus PBO P<0.001. Non-parametric bootstrap t-test. Overall axial spondyloarthritis (axSpA): PBO n=107, CZP n=218; ankylosing spondylitis (AS): PBO n=58, CZP n=121; non-radiographic axSpA (nr-axSpA): PBO n=49, CZP n=97.
Overall, the monthly improvements in social activities reported by the CZP patients resulted in cumulative gains over the 24 weeks of 9.3 full days of social, family or leisure activities over placebo.
AS and nr-axSpA subpopulations
Similar results were observed in patients with AS and nr-axSpA by week 24 of CZP treatment: patients with AS gained on average 2.0 days of social activities per month, compared with 1.9 days in the placebo group. Patients with nr-axSpA gained on average 3.2 days month, compared with 2.8 days in the placebo group. Treatment responses in both subpopulations were further continued to week 96 (figure 5B).
Discussion
Patients with AS often experience a substantial impact on the ability to work, as well as significant restrictions on work productivity.10 14 26–28 However, there is a shortage of research exploring the impact of disease on work productivity in the overall axSpA population, which includes both patients with AS and nr-axSpA. The typical age of disease onset, in the third or fourth decade, is when many patients are in the midst of their working careers,29 30 and the resulting limitations in work productivity are likely to have substantial consequences for career progression. Loss of productivity also affects patients’ lives outside work, and patients with AS and nr-axSpA report significant reductions in their ability to participate in social and leisure activities, and general health-related quality of life.12 16 31 In order to fully quantify the impact of an intervention on productivity, it is crucial to consider the entire productivity continuum both at work and at home.32
The financial burden associated with axSpA is significant, and it has been suggested that costs associated with loss of productivity constitute the largest part of the total cost of illness of AS.11 Patients with AS and, consequently, society are affected by substantial costs related to medications and healthcare provider expenses.10 11 33 Therefore, there is interest in understanding the impact of the entire spectrum of axSpA and potential axSpA treatments on work and household productivity.
The impact of treatment of axSpA on employment and household productivity has not been widely described. A review of the effects of anti-TNF treatment in patients with AS showed improvements in work absenteeism and presenteeism,34 and a number of studies have reported that that treatment with anti-TNF agents enabled patients with RA and AS with severe disease to return to work or work more productively.8 19 35 36 It was also indicated that there is less future work disability in patients who responded to anti-TNF therapy.8 19 35 CZP and methotrexate (MTX) combination therapy has previously been found to improve productivity within and outside the home in patients with RA, where improvements were seen relative to placebo plus MTX.37 Similarly, CZP treatment resulted in increased work and household productivity in patients with PsA.38
RAPID-axSpA is the first large, randomised controlled trial enabling a comprehensive evaluation of the baseline characteristics, burden of disease and treatment efficacy of an anti-TNF, allowing direct comparison of nr-axSpA and AS subpopulations in terms of economic burden.
In general, a higher burden of disease at study baseline was seen in patients with nr-axSpA than AS. This may be due to demographic differences in the two populations: in RAPID-axSpA, there were expected differences in age, gender and disease duration between AS and nr-axSpA subpopulations, consistent with previous reports.39 40 On average, patients with nr-axSpA were younger, with a shorter disease duration and a higher proportion of women. Baseline data suggest that axSpA has a substantial impact on work productivity, both at paid work outside home and within the home. These findings are consistent with previous reports of work disability and loss of productivity in patients with AS, indicating that the disease has a significant impact on employment status, ability to work and is associated with a high risk of premature retirement.8 10 19 41 Of note, a difference was observed in the proportion of patients employed at baseline between the CZP and placebo treatment arms due to chance in randomisation as patients were not stratified by employment status at baseline. These differences were seen prior to any study treatment being administered.
CZP treatment resulted in rapid and sustained improvements in workplace and household productivity. Significant reductions in absenteeism, presenteeism and axSpA interference with work, as well as improvements in household productivity and increased participation in social, family and leisure activities were observed as early as week 4 and maintained through to week 96. Similar improvements were reported in AS and nr-axSpA subpopulations. These results are consistent with the clinical improvements seen in response to CZP treatment in patients with axSpA20 21 and indicate that CZP is a valuable therapeutic option. Increases in productivity may also contribute to improvements in patients’ health-related quality of life.35
A limitation of the current report is that the use of the clinical trial population, composed of patients with active disease, may not accurately represent the entire spectrum of patients with axSpA.
In summary, the results of the RAPID-axSpA trial demonstrate that treatment with CZP is efficacious in patients with axSpA, including the AS and nr-axSpA subpopulations, resulting in significant improvements in work and home productivity as well as increased participation in family, social and leisure activities over 96 weeks.
Acknowledgments
The authors thank the patients and their caregivers in addition to the investigators and their teams who contributed to this study. The authors acknowledge Joseph Burgon, PhD, PGCert from Costello Medical Consulting, Cambridge, UK, for medical writing and editorial assistance in preparing this manuscript for publication based on the authors’ input and direction. All costs associated with the development of this manuscript were funded by UCB Pharma.
References
Footnotes
Contributors All authors made a substantial contribution to the conception or design of the work, or the acquisition, analysis or interpretation of data for the work. All authors revised the work critically, provided final approval of the version for publication and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding This work was supported by UCB Pharma, who funded this study and manuscript. UCB Pharma reviewed only for scientific and legal accuracy.
Competing interests DvdH: consulting fees: AbbVie, Amgen, Astellas, AstraZeneca, Bristol-Myers Squibb, Boehringer Ingelheim, Celgene, Daiichi, Eli Lilly, Galapagos, Gilead, Janssen, Merck, Novartis, Pfizer, Regeneron, Roche, Sanofi, UCB Pharma, Director of Imaging at Rheumatology BV. JB: research grants and/or consulting fees: Abbott, Bristol-Myers Squibb, Celgene, Celltrion, Chugai, Johnson & Johnson, MSD, Novartis, Pfizer, Roche, UCB Pharma. MR: consulting fees: Abbott, BMS, Janssen, MSD, Pfizer, Roche, UCB Pharma. OP: employee of UCB Pharma. AFK: research grants: Abbott, Amgen, Bristol-Myers Squibb, Pfizer, Roche, Janssen, UCB Pharma.
Patient consent Obtained.
Ethics approval Body varied by participating site.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.