Article Text

Abstract
Objective To analyse whether early arthritis patients who do not fulfil the American College of Rheumatology/European League Against Rheumatism (ACR/EULAR) 2010 classification criteria for rheumatoid arthritis (RA) have a different course of the disease dependent on whether they can or cannot be classified as RA because of radiographic disease (EULAR task force) at diagnosis.
Methods For this observational study within the Swiss RA cohort SCQM, we included patients with early undifferentiated arthritis (disease duration ≤1 year), who had not received any previous disease-modifying antirheumatic drugs (DMARDs). 2010 ACR/EULAR criteria negative patients were separated into two groups (radiographic vs non-radiographic arthritis) depending on whether or not they had radiographic changes defined as erosive disease by a EULAR task force (≥3 joints with erosions). The primary outcome measure was the radiographic progression detected employing the Ratingen erosion score. Health Assessment Questionnaire (HAQ) and DAS-28 were used as secondary outcome measures. The average observation period was 4 years.
Results A total of 592 patients were analysed. 240 were not classifiable as RA by application of the 2010 ACR/EULAR criteria at baseline. In 57 patients, radiographs at the first visit were not available. 133 patients had radiographic arthritis and 50 non-radiographic arthritis. Treatment was initiated in all patients with DMARDs, mostly methotrexate. No differences in DAS-28 and HAQ scores were found during follow-up. The average erosion scores were higher among patients with initially radiographic arthritis throughout the study. The progression of erosion scores over time, however, was higher in patients with initially non-radiographic arthritis with less subsequent radiological progression (3.3 erosions/year vs 0.4, respectively, p<0.0001).
Conclusions The clinical and radiographic course of early undifferentiated arthritis under treatment was not dependent on the presence of erosions in three or more joints (ie, the definition of radiographic disease by the EULAR task force) at diagnosis in our cohort.
- rheumatoid arthritis
- radiographic
- criteria
- diagnosis
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
According to the European League Against Rheumatism (EULAR) task force, rheumatoid arthritis (RA) can be classified in American College of Rheumatology (ACR)/EULAR 2010 classification criteria negative patients as three or more joints that are erosive.
What does this study add?
The clinical and radiographic course in ACR/EULAR 2010 negative patients under treatment was not dependent on the presence of erosions in three or more joints at diagnosis in our cohort.
How might this impact on clinical practice?
All patients suspected of RA should be treated equally until the clinical course demonstrates whether clinical remission and radiographic non-progression can be achieved.
Introduction
A task force of specialists from both the European League Against Rheumatism (EULAR) and the American College of Rheumatology (ACR) have proposed the 2010 ACR/EULAR classification criteria for rheumatoid arthritis (RA).1 These 2010 ACR/EULAR classification criteria define RA in patients with a score of at least 6 of possible 10. In addition, ‘patients with erosions typical of RA’ were deemed to have ‘prima facie evidence of RA and can be classified as such’.1 However, the definition of ‘erosions typical for RA’ was not provided in the manuscript.
A definition of ≥2 erosions being typical for RA had been evaluated in 518 patients with undifferentiated arthritis of the Leiden cohort in 20092 showing that 53% of these patients will develop the full picture of RA. An analysis of the ESPOIR (Étude et Suivi des POlyarthritites Indifférencées Récentes) and Leiden cohorts3 employed as definition the start of methotrexate (MTX) or any other disease-modifying antirheumatic drug (DMARD) within the first year and persistency over 5 years. This analysis showed a specificity of 85%–95% for the definition of at least three joints with erosions depending on the outcome used in the patients who did not fulfil the 2010 ACR/EULAR criteria (ACR/EULAR negative). Based on these data, a EULAR task force has now defined erosive disease4 for the use in the 2010 ACR/EULAR rheumatoid arthritis classification criteria, as at least three erosions (defined as a cortical break) at three different sites of the proximal interphalangeal joints, MCP, MTP or the wrist (counted as one joint). The major issue with such an analysis is how to define an early arthritic disease to be severe enough to fulfil the requirements being a chronic inflammatory disease as RA.
The definition of this consensus statement has, so far, not been applied in another study population. The aim of the study presented here was to evaluate if ACR/EULAR negative early arthritis patients have a different course of the disease dependent on whether they can be classified as RA because of radiographic disease at diagnosis or not, with regard to development of new joint erosions (primary end point), disease activity (DAS-28 and Health Assessment Questionnaire (HAQ)) and the therapeutic strategy.
Methods
Study population and design
The Swiss Clinical Quality Management in rheumatoid arthritis (SCQM) is a population-based and hospital-based RA cohort, which has been described in detail elsewhere.5 6 In brief, the SCQM is a population of patients with RA and patients with undifferentiated arthritis (UA). The diagnosis, independent on whether it was RA or UA, was established by the treating rheumatologist.
In this study, we restricted our analysis to patients with early arthritis. The analysis included data collected between January 1998 and November 2011. Inclusion criteria for the analysis were a diagnosis of early arthritis by a rheumatologist, defined as less than 1 year of duration after the first symptoms and at least one follow-up visit. Patients treated with glucocorticoids, synthetic or biological DMARDs for more than 31 days before the first visit were excluded from the analysis. Other exclusion criteria were missing 28 joint counts or radiographs at baseline.
Retrospective assessment of the ACR/EULAR 2010 classification criteria
Patients with RA and UA were retrospectively classified employing the 2010 ACR/EULAR criteria at the time of the first data entry. Joint counts were assessed according to the 2010 ACR/EULAR criteria resulting in different scores for either tender and/or swollen joints: a score of 0 meant no joint involvement, a score of 2: 1–3 joints, a score of 3: 4–10 joints and a score of 5: >10 joints. Positive acute-phase reactants were equivalent to a score of 1. C reactive protein (CRP)/erythrocyte sedimentation rate (ESR) was positive if greater than 9 mg/L or 27 mm/h, respectively. Disease duration scored for 1 if ≥6 weeks. For anti-citrullinated peptides antibodies (ACPA) and rheumatoid factor, a score of 0 was attributed to double-negative patients and a score of 2 to single-positive patients. If a patient was double positive, a score of 3 was assigned. This adaptation has been validated before in the same patient population.7 The cumulative score for joint count, acute phase reactants, disease duration and rheumatoid factor/ACPA was calculated for every patient. Patients were defined as 2010 ACR/EULAR positive if the cumulative score was higher than 5 and as ACR/EULAR negative if below 6.1 For this analysis, we selected for 2010 ACR/EULAR negative patients. In these patients, the Ratingen score was evaluated for the presence or absence of ≥3 joints at disease onset. In the Ratingen score, up to 5 points can be obtained per joint or erosion. Therefore, radiographs from patients at disease onset were re-evaluated by two experienced rheumatologists (RBM and JvK, both with >15 years of experience) to set the definition of radiographic disease as erosions in ≥3 joints at disease onset. This analysis was restricted to radiographs of hands and feet. In the event of disagreement between the readers with regard to the classification as radiographic or non-radiographic disease, a consensus was found.
Outcome parameters
The primary endpoint was the radiographic progression during follow-up. The radiographic outcome was analysed on serial radiographs according to the number and the size of bone erosions. Erosions were measured prospectively using a validated scoring system (Ratingen score), based on the amount of joint-surface destruction for each joint. The Ratingen score is a validated scoring method to analyse radiographs of patients with arthritis.8 It scores 28 joints for erosions, from 0 to 5 (maximum score 190) depending on the destructed surface area of the individual joint. The joints analysed are the same as in the publication of van der Heijde et al.4 There is no evaluation of joint space narrowing. The interobserver agreement and test–etest reliability are high, as published.8
Secondary endpoints were clinical disease progression and functional disability. Change of DAS-28 scores were analysed in the different patient groups. The DAS-28 scores were calculated employing the swollen and tender joint count, ESR and/or CRP as available. If both ESR-DAS and CRP-DAS were available, the average of both scores was used as described before.9 10 Functional disability was assessed with the HAQ.
Statistical analysis
The baseline disease characteristics of patients in the two groups were compared using standard descriptive statistics. Continuous variables were compared using Student’s t-test and categorical variables with χ2 test. Curves showing changes in DAS-28 and HAQ scores over time were created using loess smoothing of the raw data. The effect of a positive erosion score (cut-off ≥3 joints) was analysed in ACR/EULAR negative patients for DAS-28 and HAQ scores using linear mixed models with random slope and random intercept, and adjusted for various baseline factors (time since diagnosis, gender, age, medication, positivity for rheumatoid factor, DAS-28 at baseline, Ratingen score at baseline, GAQ-DI at baseline, ESR at baseline, ACPA positivity at baseline) in a univariate fashion. Slopes of the Ratingen score after diagnosis were compared between groups using analysis of variance (ANOVA). All statistical analyses were two-sided at the 0.05 significance level. The analyses were performed using Excel (V.14.2.2), the GraphPad Prism 5 software and the lme4 package in R (V.3.0.1; R Core Team (2013). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. URL http://www.R-project.org/).
Results
Patients
Of the 9627 patients in the database, 1345 had a disease duration of less than 1 year at baseline and 947 patients were not pretreated with any glucocorticoids or DMARD for more than 31 days at baseline, of which 756 patients were diagnosed as RA or UA, of which 609 patients had at least one follow-up in the database and of which 592 patients in the database had valid 28-joint counts at baseline. The new 2010 ACR/EULAR criteria were applied to these patients. In total, 240 patients were not classifiable as RA according to the 2010 ACR/EULAR criteria (<6 out of 10, 40.5%). We selected 183 of the 240 ACR/EULAR negative patients with available radiographs at the first visit. Fifty of these patients had <3 (referred to as non-radiographic UA, ‘nr-UA’) and 133 patients with ≥3 joints with erosions (referred to as radiographic UA, ‘rad-UA’) at the baseline visit. The inter-reader reliability was 92.3% (data not shown).
Baseline demographical data
The analysis of the demographical data revealed no significant differences for age, gender and symptom duration at disease onset. The analysis of parameters indicative of disease activity demonstrated no significant differences for swollen and tender joint count, CRP, ESR and DAS-28 scores in patients with nr-UA versus patients with rad-UA. Only rheumatoid factor was significantly more frequent in patients with nr-UA (χ2 test: 4.408; p=0.036), whereas positivity for ACPA did not differ significantly between the two groups (table 1).
Demographical data at baseline
Initial treatment
One hundred twenty-five patients were initially treated with MTX (74%, 66% of rad-UA and nrUA, respectively), 23 with sulfasalazine (16%, 11% of rad-UA and nrUA, respectively), 15 with leflunomide (8% for both rad-UA and nrUA) and 15 with hydroxychloroquine (10%, 8% of rad-UA and nrUA, respectively). Glucocorticoids were employed as an initial treatment in 123 patients (figure 1B, 64%, 68% of rad-UA and nrUA, respectively). There were no major differences in the initial treatment with DMARDs and glucocorticoids between the two patient groups (figure 1C).

Treatment strategy. For every patient, changes of treatment were analysed per change, for up to five subsequent therapeutic changes. Treatment changes are depicted numerically from 1 to 5. Med. 1 is equal to the first treatment initiated at disease onset. Med. 2 represents an alternative medication used at a subsequent visit, if Med. 1 was changed to another drug, independent of the reason for change. The total number of patients is shown who underwent a treatment change independent on the particular change (A), change of corticosteroid regimen (B), synthetic DMARD therapy (C), TNF antagonist treatment (D) and non-anti-TNF biological treatment (E). Therapeutic decisions for parts B–E of the figure are depicted as percentages of decisions taken in the different groups. All patients groups undergoing treatment changes are shown separately for non-radiographic (black) and radiographic (white) patients. ACR, American College of Rheumatology; DMARD, disease-modifying antirheumatic drug; EULAR, European League Against Rheumatism; TNF, tumour necrosis factor.
Change of treatment
The analysis of treatment changes was limited to a maximum of five. The data demonstrated that the number of patients whose treatment needed adaption decreased continuously in both patients groups (figure 1A). In detail, the number of newly prescribed glucocorticoids and DMARDs decreased with every visit for both patient groups (figure 1B and C). The number of patients with a newly initiated tumour necrosis factor antagonist treatment reached a maximum at the second treatment change and decreased thereafter (figure 1D). No differences in the therapeutic strategy between patients with rad-UA and nrUA were detected.
Radiographic data
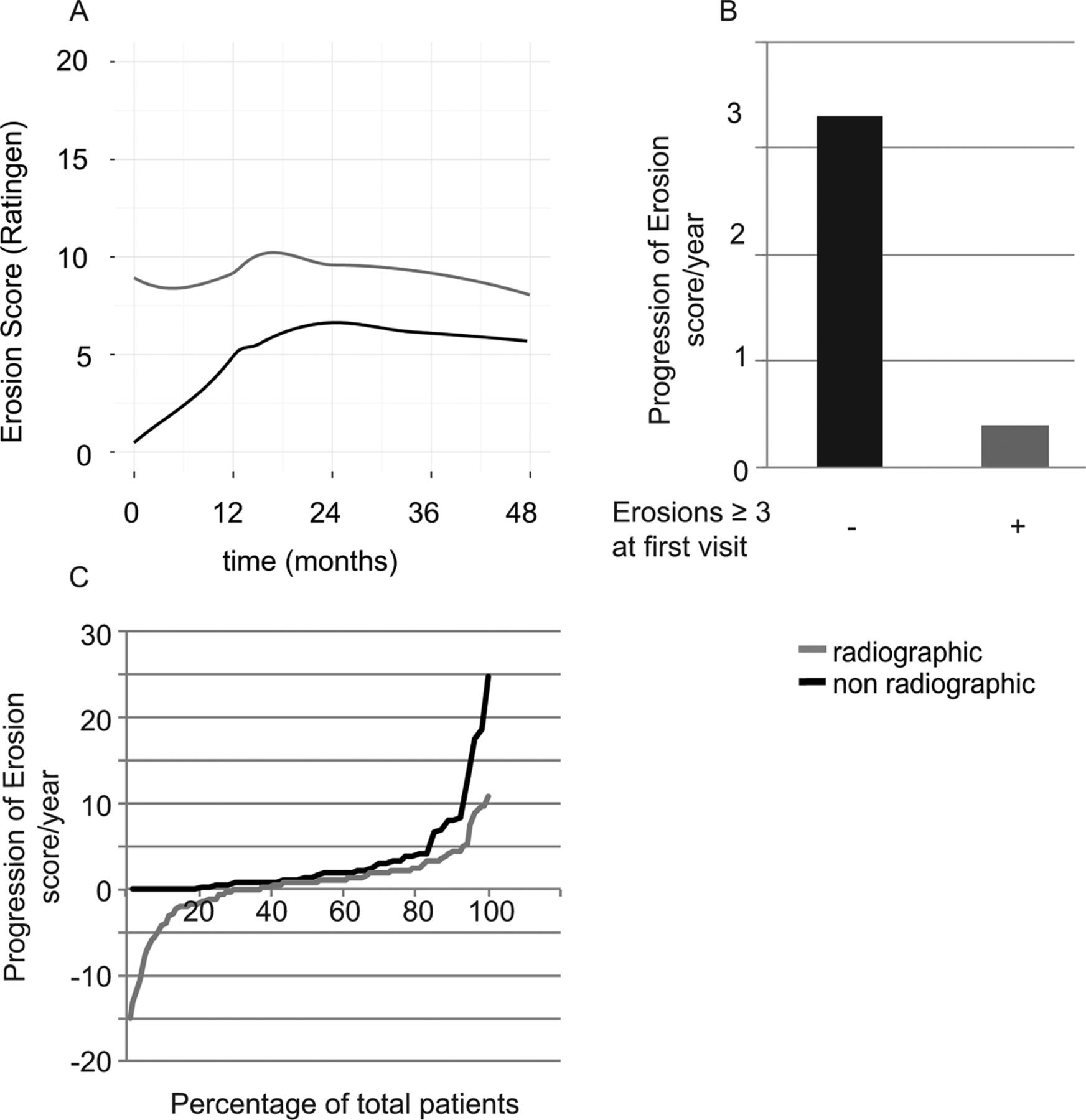
The radiographic progression was analysed employing an erosion score (Ratingen). It was assessed separately for patients with rad-UA and nr-UA. At disease onset (p<0.0001) and continuously during follow-up, the mean erosion scores were significantly higher in patients with rad-UA as compared with patients with nrUA (figure 2A). In contrast, the average yearly progression of erosion scores was 3.3 for nrUA and 0.4 for rad-UA (ANOVA, p<0.0001, figure 2B).

Radiological progression. The disease progression was analysed employing the Ratingen erosion score. (A) Average Ratingen scores per group are shown. The Ratingen scores were calculated separately for patients with radiographic (solid grey) and non-radiographic (solid black) disease. The average yearly progression over the whole follow-up period is depicted per patient group as absolute values (B) and a cumulative probability blot (C). For the cumulative probability blot, radiographic patients are shown as a solid grey line and non-radiographic patients as a solid black line.
Follow-up of disease activity
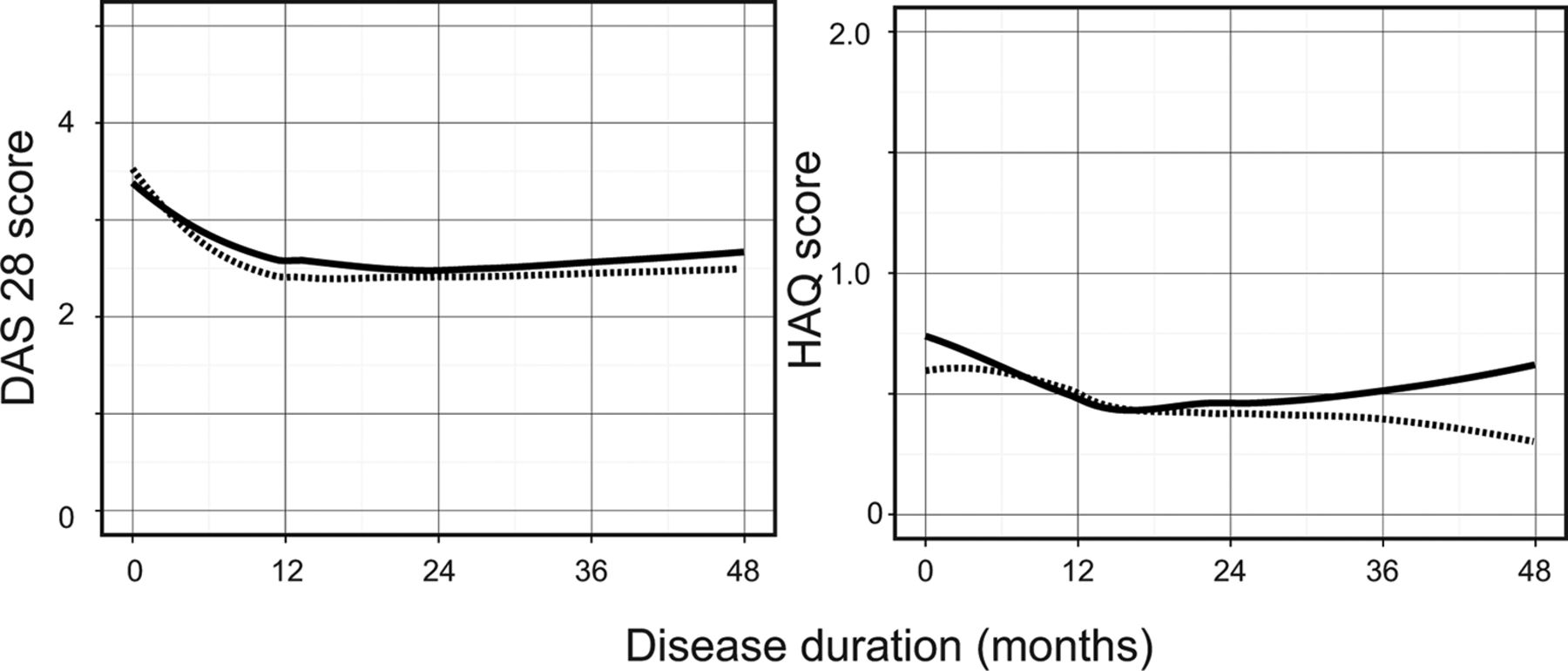
The development of disease activity was analysed separately for patients with rad-UA and nrUA employing the development of DAS-28 scores over time. At disease onset and during follow-up, no differences in DAS-28 levels could be detected comparing the two patient groups (figure 3A).

{kind=link}
{kind=link}
{kind=link}
Disease activity. The disease activity, depicted by DAS-28 (left panel) and Health Assessment Questionnaire (HAQ) score (right panel), was analysed for every patient. The data are shown as averages for radiographic (dashed line) and non-radiographic patients (solid line) for every group over 48 months.
Patient-related outcome parameter
Personal outcome analysed by HAQ scores revealed no differences in patients with rad-UA and nrUA at disease onset. After 2 years, the average HAQ scores did not differ between patients with rad-UA and nrUA. After 3 years, the average HAQ sores increased for patients with rad-UA as compared with patients with nrUA (0.17 vs 0.64 nrUA vs rad-UA, Student’s t-test: p=0.10, figure 3B).
Discussion
The new ACR/EULAR criteria were used at the time of diagnosis for the classification of 592 patients with early arthritis of the Swiss national cohort SCQM. Moreover, 41.4% of these patients were not classifiable according to the new ACR/EULAR criteria at disease onset. The definition of RA depending on the presence of joint erosions defined by a EULAR task force4 was applied in patients of the SCQM cohort who did not fulfil the 2010 ACR/EULAR criteria. Seventy-three per cent of the ACR/EULAR negative patients displayed ≥3 joints with erosions at disease onset.
No differences in clinical activity (DAS-28) and patient-related outcomes (HAQ) were observed between these two groups. In addition, changes in the therapeutic regimen were comparable. In general, we think that the therapeutic regimen in these patients reflects the common practice in Switzerland since patients are recruited into the SCQM cohort from academic hospitals as well as from private practices in Switzerland. It is, however, not known whether the patients fulfilled the 2010 ACR/EULAR criteria during follow-up because retesting of ACPA and RF was generally not recorded in the database, most probably because it was not performed.
The presence of ACPA in both patient groups of our cohort may seem rare. Our selection for patients negative for the 2010 ACR/EULAR criteria may, however, be a likely explanation because positivity for rheumatoid factor and/or ACPA increases the score by 2–3. Selecting for patients with less than a score of 6 needed for classification of RA leads, subsequently, to a lower frequency of patients achieving a higher score in the four subcategories including ACPA.
Despite the similarities in clinical outcome, patients with rad-UA showed on average continuously higher erosion scores, but a lower slope of radiographic progression as compared with patients with nrUA during the observation period.
Initial radiographic disease is understood as a positive predictor for evolving other joint erosions.11–13 In our cohort, however, the rate of progression in initially nrUA was higher than in patients with rad-UA. In both groups, erosion scores reached a plateau within the second year after disease onset. In ACR/EULAR positive patients with RA, erosion scores did, in contrast, continuously increase despite treatment (data not shown). Thus, treatment that did not differ between the two groups as shown in figure 1 may eliminate the differences in radiographic progression after 1 year in patients with UA independently of the radiographic status at disease onset. Progression within the first year may be predetermined in the phase prior to diagnosis when therapy is not yet initiated. Early, aggressive treatment might influence this radiographic progression. Furthermore, it has to be taken into consideration that as opposed to other cohort data,14 15 non-erosive disease at baseline did not correlate with less erosions during follow-up. A significant difference between the SCQM and the ESPOIR and Leiden cohorts may be that patients are included into the SCQM database not by classification criteria but by clinical diagnosis of the rheumatologist based on his experience. Clinical judgement and experience rather than application of classification criteria may explain why the development of erosions within the first year of therapy in patients with nrUA was anticipated by the treating rheumatologist. Furthermore, this may explain why such a high rate of patients with an erosive disease was detected among patients with UA.
In our study, 73% of the ACR/EULAR negative patients displayed ≥3 joints with erosions as compared with 11.7% in the Leiden cohort, 17.4% in the ESPOIR cohort3 and 5.4% published from a Norwegian Very Early Arthritis Clinic.16 In the SCQM cohort, patients with early arthritis were included at the discretion of the treating rheumatologist. All were then treated with DMARDs. In the ESPOIR cohort, patients were diagnosed by a rheumatologist as RA-like or RA17 while in the Leiden early arthritis cohort and the Norwegian Very Early Arthritis Clinic, all patients with ≥1 joint, symptom duration <2 years18 were included. In contrast to the publications of Knevel et al 3 and Thabet et al,2 our study focused on the evolving disease. Clinical parameters and erosions over the subsequent 5 years and not on the percentage of patients fulfilling the ACR/EULAR criteria over time2 or requiring DMARD treatment3 were analysed.
However, the importance of erosive disease at disease onset4 as a predictor for disease progression cannot be confirmed in our cohort of patients with undifferentiated arthritis.
To exclude confounding factors for radiographic progression, multivariate analyses were performed. No influence of either time to diagnosis, gender, age or initial DAS, HAQ, ESR or CRP was detected.
The low rate of ACPA in both patient groups may seem low. We think that this low rate is not surprising as we selected for patients negative for the 2010 ACR/EULAR criteria. In these criteria, positivity for rheumatoid factor and/or ACPA contributes to 2–3 out of 10 possible points. Selecting for patients not achieving 6 or more points needed for classification of RA leads, subsequently, to a lower frequency of patients achieving higher points in the four subcategories including ACPA.
In conclusion, these data strongly suggest that in the SCQM cohort, presence of three or more joints with erosions at disease onset does not reliably select patients with more clinical activity or radiographic progression during the further course of the disease.
In consequence, all patients suspected of RA should be treated equally until the clinical course demonstrates whether clinical remission and radiographic non-progression can be achieved.
Acknowledgments
We thank the participating rheumatologists and patients who made this study possible, Sabine von Kaenel, Hans A Schwarz and Adrian Forster (SCQM general manager, past and present presidents, respectively) for unrestricted support and the entire SCQM staff for data management. The authors acknowledge and thank Désirée van der Heijde and Michael Schiff for their critical revision of the manuscript. A list of rheumatology private practices and hospitals that are contributing to the SCQM registries can be found online (http://www.scqm.ch/institutions).
References
Footnotes
Funding The study was conducted without special funding. SCQM has received grants from the Swiss Health authorities (BAG), the Swiss Academy for Medical Sciences (SAMW) and private companies (Pfizer, AbbVie, MSD, Aventis, Bristol-Myers, Mepha, Merck, Novartis and Roche).
Competing interests None declared.
Ethics approval Ethics approval for the collection of patient data for the SCQM Cohort was given by the regional review boards.
Provenance and peer review Not commissioned; externally peer reviewed.
Presented at ‘R B Mueller, T Kaegi, S Haile, and J von Kempis. The clinical and radiographic course of early undifferentiated arthritis under treatment is not dependent on the amount of erosions at diagnosis. Results from the Swiss prospective observational cohort, EULAR 2014, Paris, EULAR14-SCIE-2034’. ‘R Mueller, T Kaegi, S Haile and J von Kempis. The clinical and radiographic course of early undifferentiated arthritis under treatment is not dependent on the amount of erosions at diagnosis. Results from the Swiss Prospective Observational Cohort. Abstract 2914, ACR 2014, Boston, USA’.
Patient consent Obtained.
Contributors RBM: set-up of the study, interpretation of data, writing of the manuscript. SRH: statistical analysis, writing of the manuscript. TK: interpretation of data, writing of the manuscript. MS: interpretation of data, writing of the manuscript. HS-K: interpretation of data, writing of the manuscript. JvK: set-up of the study, interpretation of data, writing of the manuscript.
Data sharing statement No additional data are available.