Article Text

Statistics from Altmetric.com
Polymyalgia rheumatica (PMR) is an elderly onset syndrome characterised by aching and stiffness in the shoulders and the pelvic girdle associated to increased levels of acute phase reactants and rapid response to glucocorticoids.1 Although the cause of PMR remains unknown, most of the evidence suggest a multifactorial aetiology inducing an immunomediated pathogenesis.1 2
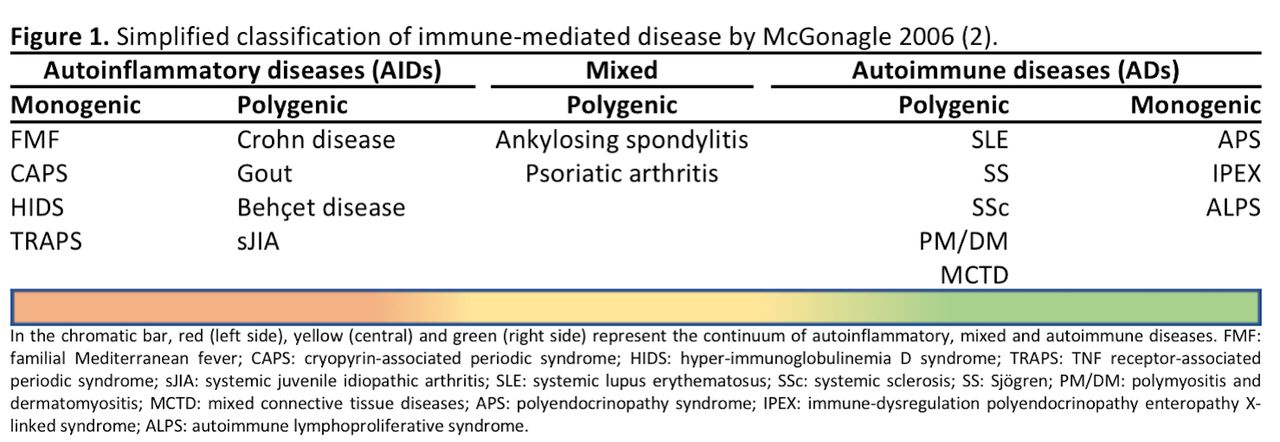
According to the ‘immunological continuum model’ proposed by McGonagle in 2006, all immune-mediated diseases can be conceptualised as predominantly autoinflammatory, predominantly autoimmune or mixed, on the basis of the relative contributions of innate and adaptive immune responses.3 Autoinflammatory diseases (AIDs) are characterised by tissue inflammation mainly due to aberrant activation of innate immune system without autoantibodies production and autoreactive T lymphocyte activation. In contrast, autoimmune diseases (ADs) are typically depicted by an abnormal activation of the adaptive immune system.4 However, the emerging understanding of the close linkage between innate and adaptive immunity led to consider the rare monogenic AIDs and ADs as the two opposite ends into a continuum of immune-mediated disorders, where middle entities are recognised (figure 1).3
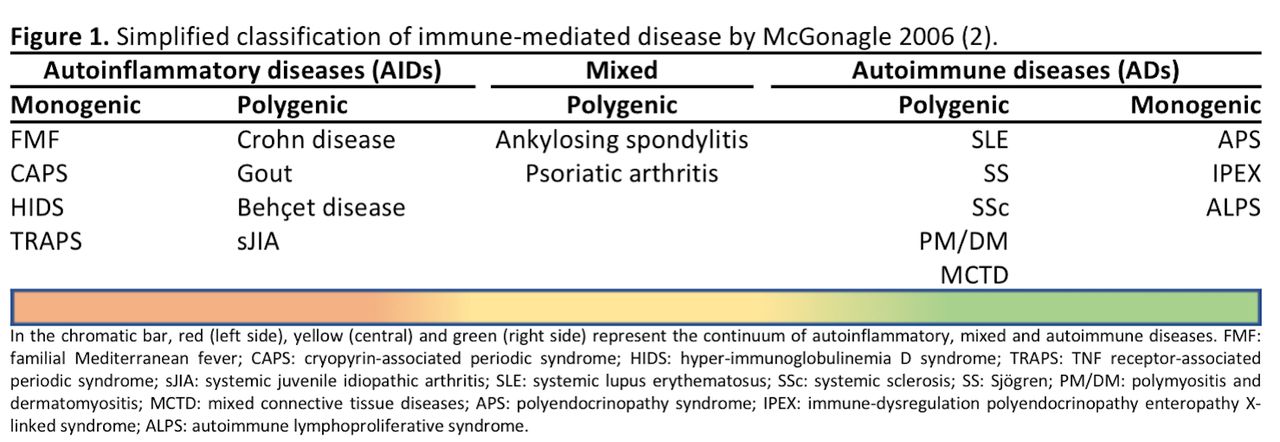
Simplified classification of immune-mediated disease by McGonagle and McDermott.3
In the view of this background, we tried to envisage the most suitable place for PMR into the spectrum of the autoinflammatory/autoimmune disorders by reviewing and interpreting current evidence.
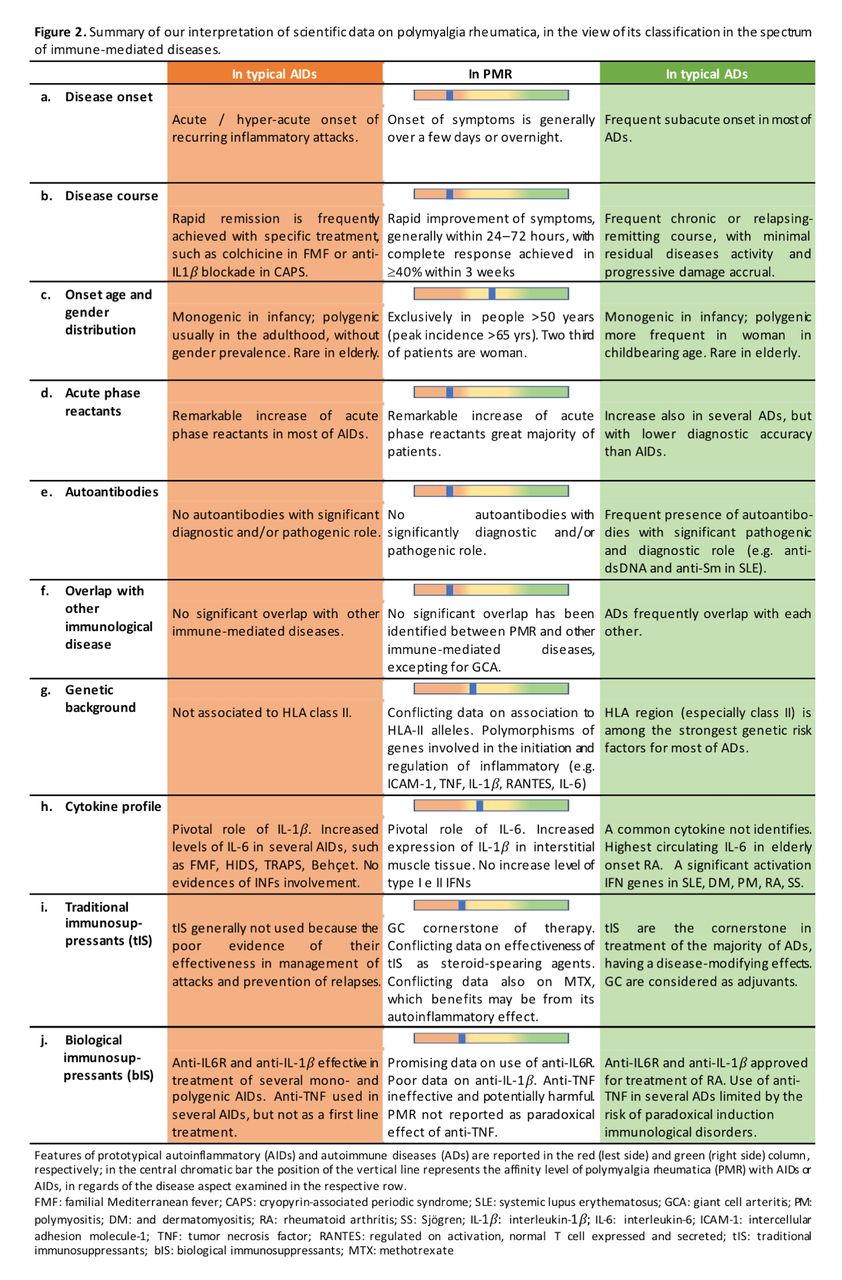
Clear indication for a prevalent autoinflammatory background of PMR is related to the disease onset and course. Actually, starting of symptoms is generally over a few days or overnight in PMR,1 as well as in inflammatory periodic-recurring occurrence of AIDs,5 but in contrast to classic polygenic ADs where a subacute onset is frequently recorded (figure 2A).6 Further, after low-dose glucocorticoid therapy initiation, patients with PMR experience a rapid improvement of symptoms, generally within 24–72 hours, and more than 40% of them achieve complete response within 3 weeks.1 Similarly, in rare monogenic AIDs, a rapid remission of symptoms and significant reduction in frequency of inflammatory attacks is rapidly achieved with specific treatment, such as colchicine in familial Mediterranean fever (FMF) and interleukin-1β (IL-1β) blockade in cryopyrin-associated periodic syndrome.7 Conversely, a chronic or relapsing-remitting course, with a minimal residual disease activity and progressive damage accrual, is frequently recorded in ADs (figure 2B).8
{kind=link}
{kind=link}
Summary of our interpretation of scientific data on polymyalgia rheumatica, in the view of its classification in the spectrum of immune-mediated diseases.
Age of onset and gender distribution are inconclusive in discriminating the prevalent autoinflammatory or autoimmune nature of PMR (figure 2C). Indeed, both in ADs and AIDs elderly onset is rare, and the main determinant of the onset age is the monogenic (childhood) or polygenic (adulthood) nature of the disease.4 9 Further, the preferential involvement of woman in PMR (female to male ratio=2:1) seems related to a different and currently unknown mechanism than the arise in oestrogen production reported as one of the main determinants of the female prevalence in typical ADs, such as systemic lupus erythematosus (SLE) (female to male ratio=9:1).1 9
Laboratory findings lean towards a predominant role of innate immune response in PMR. Indeed, a remarkable increase of inflammatory markers is one of the most consistent features in patients with both PMR and AIDs, so that it is included into the diagnostic criteria and monitoring parameters for both conditions.1 7 Increase of acute phase reactants can also occur in ADs, but with lower frequency and diagnostic accuracy (figure 2D).4 Further, autoantibodies carrying a significant pathogenic and/or diagnostic role have not been identified in PMR, as well as in AIDs,4 whereas they are frequently associated to prototypical ADs (eg, anti-double-stranded DNA in SLE, anti-citrullinated peptide in rheumatoid arthritis (RA)) (figure 2E).4 10 Noteworthy, lack of pathogenetic autoantibodies is typically recorded in other immune-mediated diseases, such as the major histocompatibility complex class I (MHC-I)-pathies (eg, ankylosing spondylitis, psoriatic arthritis) that are reported as prototypical mixed autoinflammatory/autoimmune disorders in the immunological continuum.3
Similar to AIDs and in contrast to what is reported for typical ADs, not significant overlap has been identified between PMR and other immunological disorders, excepting for giant cell arteritis (GCA).11 However, it is still unclear whether GCA represents a separate condition from PMR or a potential expression of the same disease (figure 2).3 12 Further, a mixed contribution of innate and adaptive immunity, supported by the bringing function of Th17 cells, has been recognised in the GCA.1
Despite the widely incomplete knowledge on pathogenesis of PMR, some suggestions for a predominant autoinflammatory nature of the disease arise from the genetic background and cytokine profile. Indeed, a clear association between human leukocyte antigen (HLA) class II alleles (especially HLA-DRB1*0401) and isolated PMR has not been definitely demonstrated due to conflicting data from different populations.1 On the other hand, HLA class II alleles have been found to associate with GCA susceptibility and GCA with PMR symptoms, as well as in most of ADs (figure 2G).13–15 Polymorphisms of additional genes involved in initiating and regulating inflammatory response, such as intercellular adhesion molecule-1, tumour necrosis factor (TNF), interleukin 6 (IL-6) and interleukin 1 (IL-1) receptor antagonist (IL-1RN) have also been identified as possible susceptibility factors for PMR.16 Interestingly, Alvarez-Rodriguez reported that the IL-1RN*2 polymorphism in a homozygous state associated to higher susceptibility to PMR when compared with healthy controls and GCA, as well as to elderly onset RA (EORA) when compared with young-onset RA.15
Regarding the cytokine profile, evidence of a IL-6 central pathophysiological role in PMR has been provided. Remarkably, among rheumatic diseases, the highest serum levels of IL-6 were found in patients affected by PMR and GCA17 as well as in EORA.18 The latter presents some not canonical features compared with traditional ADs (eg, lower prevalence of autoantibodies, reduced prevalence in females, less straight association with HLA-II) and might be part of an autoinflammatory–autoimmune mixed subtype of RA.19 Further, in contrast to several ADs, increased levels of serum interferon-γ (IFN-γ) were not found in PMR. Moreover, IFN-γ was observed in the temporal artery biopsy (TAB) specimens of GCA patients, while it was not seen in TAB of patients with isolated PMR, suggesting a key role of this cytokine in the progression to overt arteritis.20 Finally, increased level of circulating type I IFN has not been reported neither on PMR and GCA21 and no data are currently available on type I IFN signature, which is considered an hallmark of several ADs (figure 2H).
Further pathobiological findings supporting the key role of innate immunity in PMR pathogenesis are represented by the increased expression of toll-like receptor (TLR)-7 and TLR-9 in peripheral blood monocytic cells and the emerging involvement of Th17 cells.22
To date, glucocorticoids remain the cornerstone of treatment for PMR, whereas poor evidence is available on the effectiveness of traditional immunosuppressants. Methotrexate (MTX) is the most used glucocorticoid-sparing agent in PMR, although randomised controlled trials data on relapse rate and cumulative glucocorticoid dose reduction are conflicting.23 Potential benefit of MTX may be related to antinflammatory effects, resulting from reduced monocytic cell activation, decreased IL-1 and IL-6 secretion, as well as from inhibition of cyclo-oxygenases synthesis, neutrophil chemotaxis and adhesion molecules expression.24 Traditional immunosuppressants are generally not used in AIDs because of the poor effectiveness in the management of attacks and prevention of relapse.7 25 Conversely, traditional immunosuppressants are the first-line treatment in most of ADs, while glucocorticoids can be associated as adjuvant therapy, especially in the induction phase of the treatment (figure 2I).26
Experience from patients with PMR symptoms in GCA and data from an open-label uncontrolled study on 20 subjects with isolated PMR suggest anti-IL-6R therapy as an effective option in reducing Disease Activity Score and reducing cumulative exposition to glucocorticoids (glucocorticoid-sparing effect at 24 weeks is 70.2%).27 Anti-IL-6R also showed promising results in several AIDs, such as systemic juvenile idiopathic arthritis, Behçet disease, FMF and TNF receptor-associated periodic syndrome.28 Most of current data on anti-TNFα treatment suggest it is ineffective, expensive and potentially harmful in patients with PMR.1 Positive results in terms of effectiveness were detected for connective tissue diseases and other ADs, but its use is limited by the observation of several cases of anti-TNFα-induced autoimmune disorders.29 Interestingly, PMR is not reported among the immune-mediated paradoxical effect of anti-TNFα (figure 2J). Data on anti-IL-1β are limited to a single blind study, where canakinumab was administered to three patients with new-onset PMR, with not conclusive results in terms of effectiveness.30 Therefore, further data from large trial on anti-IL-1β in PMR would be warranted.
In summary, despite the incomplete knowledge of PMR pathophysiology and the lack of validate discriminative criteria for polygenic AIDs, current evidence suggests that PMR does not easily fit into any of the two pure ends in the spectrum of the immune-mediated disorders, but a greater affinity for AIDs seems to emerge.
In our opinion, this interpretation of the available scientific data might represent an insight with a significant practical implication. Indeed, among the unmet needs in PMR, there is the availability of effective and safety therapeutic options for patients not adequately responsive or requiring longer exposition to glucocorticoids or with an unfavourable risk profile of steroid-related adverse effects. In this view, the recognition of predominantly autoinflammatory nature of PMR should address future research aimed to develop targeted therapies.
References
Footnotes
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent Not required.
Contributors AM: conceived of the present idea. AF and MP: equally contributed to perform the literature review and draft the manuscript. All authors contributed to the interpretation of the recorded evidence. AC, CS and AM: critically reviewed the manuscript. All Authors approved the final version.