Article Text

Abstract
Introduction An understanding of real-world predictors of abatacept retention is limited. We analysed retention rates and predictors of abatacept retention in biologic-naïve and biologic-failure patients in a 12-month interim analysis of the 2-yearAbataCepTIn rOutiNe clinical practice (ACTION) study.
Methods ACTION was an international, observational study of patients with moderate-to-severe rheumatoid arthritis (RA) who initiated intravenous abatacept. In this 12-month interim analysis, crude abatacept retention rates, predictors of retention and European League Against Rheumatism (EULAR) response were evaluated in both biologic-naïve and biologic-failure patients. Retention by rheumatoid factor (RF) and anti-cyclic citrullinated peptide (CCP) status was also assessed, in patients with or without baseline radiographic erosions, and by body mass index (BMI).
Results Overall, 2350/2364 enrolled patients were evaluable (674 biologic naїve; 1676 biologic failure). Baseline characteristics were largely similar in biologic-naïve and biologic-failure groups. Crude retention rates (95% CI) at 12 months were significantly higher in biologic-naїve (78.1%(74.7% to 81.2%)) versus biologic-failure patients (69.9%(67.6% to 72.1%); P<0.001). RF/anti-CCP double positivity predicted higher retention in both patient groups, and remained associated with higher retention in patients with erosive disease. BMI did not impact abatacept retention in either patient group, irrespective of RF/anti-CCP serostatus. Good/moderate EULAR response rate at 12 months was numerically higher in biologic-naїve (83.8%) versus biologic-failure (73.3%) patients. There were no new safety signals.
Conclusion High levels of intravenous abatacept retention in clinical practice were confirmed, particularly in biologic-naïve patients, including in those with poor RA prognostic factors. Retention was unaffected by BMI, regardless of RF/anti-CCP serostatus.
Trial registration number NCT02109666; retrospectively registered 8 April 2014.
- ant-ccp
- dmards (biologic)
- rheumatoid arthritis
- rheumatoid factor
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Rheumatoid factor (RF)-positive and/or anti-cyclic citrullinated peptide (CCP)-positive status are associated with greater efficacy of abatacept than seronegative status in biologic-naïve patients with rheumatoid arthritis (RA).
Positivity for both RF and anti-CCP is associated with a greater likelihood of abatacept retention than single positivity or double negativity in patients with previous exposure to one or more biologic.
What does this study add?
Seropositivity is associated with improved abatacept retention in both biologic-naïve and biologic-failure patients. There was an association between seropositivity and improved abatacept retention in those with erosive disease.
Body mass index did not affect abatacept retention in either biologic-naïve or biologic-failure patients, regardless of RF or anti-CCP serostatus.
How might this impact on clinical practice?
An increased knowledge of the combined effect of poor prognostic factors for RA and predictors of abatacept retention may support clinical decision-making and personalised treatment strategies.
Introduction
The treatment of rheumatoid arthritis (RA) has undergone significant evolution through optimisation of conventional and new biologic therapies. However, not all patients benefit; some discontinue treatment due to a lack of response, a change in initial response or intolerance. These challenges highlight the need to identify predictors of response to optimise treatment choice. The identification of real-world predictive factors of treatment retention in patients with RA could assist rheumatologists with therapeutic decision-making in clinical practice and support personalised medicine.
Several potential predictors of abatacept retention have been identified in real-world studies and include known poor prognostic factors in RA. Abatacept retention rates are higher for biologic-naïve patients than for those with previous failure of a biologic disease-modifying antirheumatic drug (DMARD).1 2 Abatacept retention is significantly associated with both the presence of anti-cyclic citrullinated peptide (CCP) and rheumatoid factor (RF), and seems to be unaffected by weight/body mass index (BMI).3–7 However, available real-world data on predictors of abatacept retention are derived from analyses of mostly biologic-failure patients, and data for biologic-naïve patients are limited to short-term analyses.4 7 This analysis was designed to compare 1-year retention rates for abatacept in both biologic-naïve and biologic-failure patients.
The international A bataCepT In rOutiNe clinical practice (ACTION) study aims to provide prospective, real-world data on abatacept retention in patients with RA and to identify predictors of abatacept retention. Three successive patient cohorts were recruited: biologic-naïve or biologic-failure patients (cohort A), biologic-naïve patients only (cohort B) and biologic-failure patients only (cohort C). Previous analyses of biologic-failure patients enrolled in ACTION found that predictors of higher abatacept retention included anti-CCP positivity, RF and anti-CCP double positivity, prior exposure to <2 anti-tumour necrosis factor (TNF) agents, cardiovascular comorbidity and residence in Greece or Italy versus Germany.5 8 In the current interim analysis of both biologic-naïve and biologic-failure patients enrolled in ACTION, we assessed the predictors of abatacept retention at 12 months in both patient groups, with particular focus on patients with poor prognostic factors of disease progression at baseline.
Methods
Study design and analysis population
Study design and ethics approvals for the ACTION study have been reported previously.9 Briefly, ACTION was a 2-year, international, multicentre, observational cohort study of patients who initiated intravenous abatacept in routine clinical practice across Europe (Austria, Belgium, Czech Republic, Denmark, France, Germany, Greece, Italy, Netherlands, Spain and Switzerland) and Canada (see online supplementary figure S1).9 Participating countries were required to have marketing authorisation for abatacept and a reimbursement policy. No product was provided to physicians or patients by the study sponsor.
Supplementary file 1
Enrolled patients provided informed consent (written or not, according to the local laws), were aged ≥18 years, and had moderate-to-severe RA as defined by the American College of Rheumatology 1987 revised criteria10 and consistent with the abatacept label in Europe and Canada.11 12 Any patients already enrolled in a randomised clinical trial were excluded. Patients were enrolled over three periods (cohorts A, B and C), either prospectively at initiation of intravenous abatacept or retrospectively within 3 months of initiation of intravenous abatacept (see online supplementary figure S2). In Europe, intravenous abatacept plus methotrexate (MTX) was initially approved for the treatment of moderate-to-severe RA in patients with insufficient response or intolerance to anti-TNF therapy (21 May 2007 to 30 June 2010). Approval was later extended to patients with inadequate response to MTX and/or anti-TNF agents (1 July 2010 onwards). In Canada, abatacept is approved as monotherapy or in combination with a DMARD in patients with an inadequate response to DMARDs and/or anti-TNF agents (29 June 2006 onwards).11 12 Cohort A included patients enrolled between May 2008 and December 2010 who were biologic naïve or had failed ≥1 prior biologic agent (see online supplementary figure S1,S2). Cohort B included patients enrolled between September 2010 and December 2013 who were biologic naïve (see online supplementary figure S1,S2). Cohort C included patients enrolled between October 2011 and December 2013 who had failed ≥1 prior biologic agent, and was included to investigate whether the change in abatacept approval led to its use in earlier lines of therapy (see online supplementary figure S1,S2).
Patients were followed for up to 2 years or, if the patient discontinued abatacept before the 2-year time point, up to 6 months after abatacept discontinuation. Follow-up visits were approximately every 3 months (according to clinical practice). The data cut-off date for this analysis was May 2015.
Abatacept retention
Abatacept retention over 12 months was evaluated in biologic-naïve patients (cohorts A and B), and in biologic-failure patients (cohorts A and C), including by number of previously failed biologics. Retention was defined as consecutive time on treatment. Biologic-failure patients were those in whom a previous biologic either was ineffective or had caused safety or tolerability concerns, patients in clinical remission or in whom there was a major improvement of symptoms following a previous biologic, or patients who had discontinued a previous biologic for any reason. The treating physician documented discontinuation from abatacept treatment at any follow-up visit. If patients discontinued abatacept, exposure to abatacept was defined as the time between the date of the first and the last infusion plus 30 days.
Clinical efficacy of abatacept
Clinical response to abatacept at 12 months, by treatment line, was assessed using the European League Against Rheumatism (EULAR) response criteria based on 28-joint Disease Activity Score (DAS28) (erythrocyte sedimentation rate (ESR) or C reactive protein (CRP), derived based on core components), and classified as good, moderate or no response.13 Remission was defined based on DAS28 (ESR or CRP derived based on core components) (<2.6), Clinical Disease Activity Index (CDAI) (≤2.8), Simplified Disease Activity Index (SDAI) (≤3.3) and Boolean criteria.14
Predictors of abatacept retention
Potential predictors of abatacept retention were assessed for both biologic-naïve and biologic-failure patients and included baseline demographic data (RF, anti-CCP and BMI), disease characteristics (including Patient Global Assessment (PtGA) of pain), comorbidities (including diabetes mellitus, chronic obstructive pulmonary disease (COPD), cardiac disorders, neoplasms (benign, malignant and unspecified) and psychiatric disorders), and previous and current treatments. To allow between-country effects to be explored appropriately, only patients from countries that recruited ≥10 patients were included in the analyses; Germany was the reference country as it was where the highest number of study participants was enrolled.
The impact of RF/anti-CCP on abatacept retention was assessed in patients with and without erosions. Similarly, BMI impact was assessed in patients who were RF/anti-CCP double positive or double negative (BMI: underweight/normal: <25 kg/m2, overweight: 25–<30 kg/m2 and obese: ≥30 kg/m2).
Safety
Safety was assessed in accordance with local regulations, and registered with the drug manufacturer’s global pharmacovigilance department. The relationship between the study drug and any serious adverse event (SAE) was evaluated by the treating physician. An SAE was defined as an AE that was fatal or life threatening, required or extended hospitalisation (except pregnancy), resulted in persistent or significant disability or incapacity, induced a congenital anomaly or birth defect, or was considered an important medical event. All deaths were documented whether or not they were treatment related. Safety data are presented for the full study population, regardless of prior biologic treatment.
Statistical analyses
Baseline characteristics and demographic data were reported using descriptive statistics including sample size, proportions or mean and SD. For each treatment line, crude abatacept retention rates over 12 months with corresponding 95% CIs were estimated by Kaplan-Meier analysis and compared using log-rank tests. Right censoring at the time of last information available was used for patients lost to follow-up without documented abatacept discontinuation and with follow-up <12 months.
To identify significant predictors of abatacept retention, clinically relevant variables, known risk factors and potential predictive factors for discontinuation with significance in univariable models (P≤0.20) and no collinearity were entered into multivariable Cox proportional hazards regression models. Factors with P≤0.10 after backward selection were retained in the models. Analyses were performed separately on biologic-naïve and biologic-failure patients, and additional subgroup analyses were also performed. The impact of RF/anti-CCP double-positive versus double-negative status was tested separately in patient subgroups with and without joint erosions at baseline. In addition, the impact of BMI (forced into the multivariable model) was tested after stratification by RF/anti-CCP status. Results are presented as HRs with corresponding 95% CIs and P values. The HRs were statistically significant when the 95% CIs did not cross 1.
Results
Patients
In total, 2364 patients were enrolled, of whom 2350 were evaluable (online supplementary figure S1,S3). Between May 2008 and December 2010 (cohort A, biologic naїve/biologic failure), 1137 patients were enrolled from nine countries, and 1131 of whom were evaluable (see online supplementary figure S1). Between September 2010 and December 2013 (cohort B, biologic naïve only), 555 patients were enrolled from eight countries, and 552 of whom were evaluable (see online supplementary figure S1A). Between October 2011 and December 2013 (cohort C, biologic failure only), 672 patients were enrolled from eight countries, and 667 of whom were evaluable (see online supplementary figure S1B).
Biologic-naïve patients from cohorts A and B were pooled, as were biologic-failure patients from cohorts A and C. Among all evaluable patients, 674 (28.7%) were biologic naїve and 1676 (71.3%) had failed ≥1 prior biologic: 728 (43.4%) had failed 1 biologic agent and 948 (56.6%) had failed ≥2 biologic agents; 1605 (95.8%) had failed an anti-TNF agent (online supplementary figure S3).
Overall, the biologic-naïve and biologic-failure groups represented a typical population of patients with RA who have long-standing, erosive and moderate-to-severe disease. The two patient groups had similar baseline demographic data and clinical characteristics; however, biologic-naïve patients had shorter disease duration, a lower proportion of women, fewer patients with joint erosions overall and in combination with RF/anti-CCP positivity, fewer patients who received previous RA treatments (other than MTX) and a higher proportion of patients with certain comorbidities (cardiac disorders, COPD and neoplasms; table 1).
Baseline characteristics
Abatacept retention
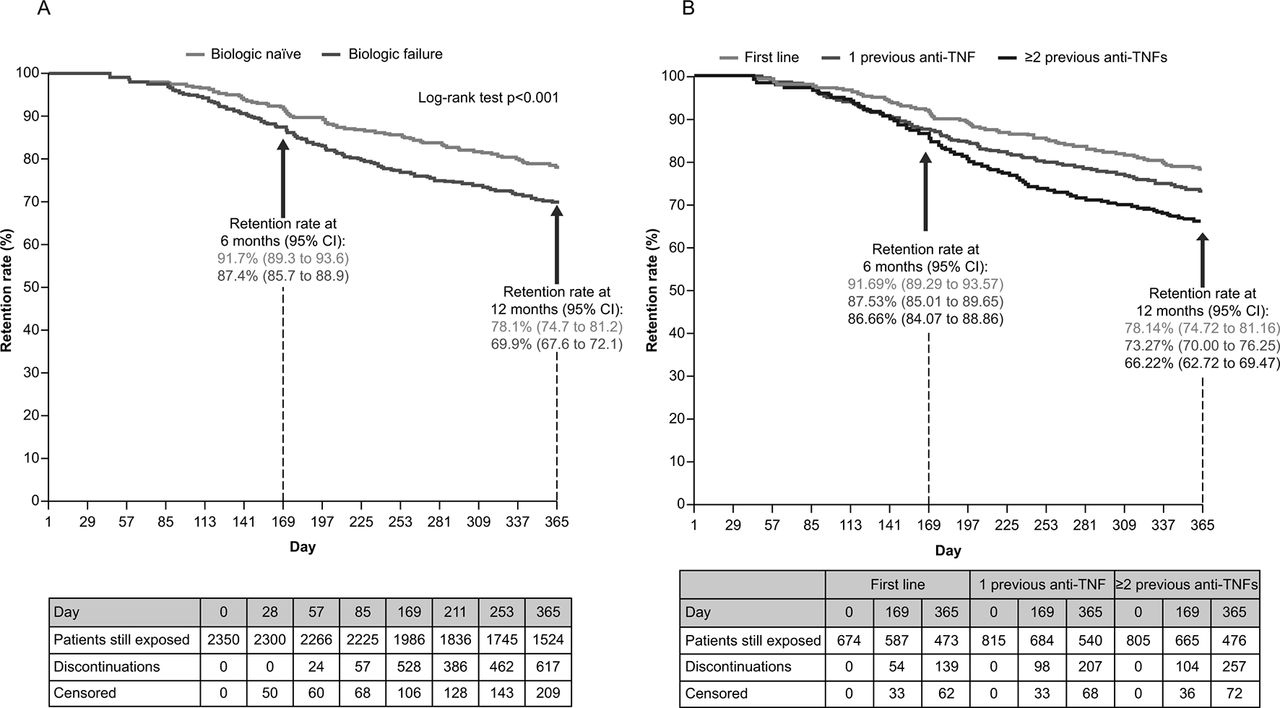
Over the 12-month follow-up, 139/674 (20.6%) biologic-naïve and 478/1676 (28.5%) biologic-failure patients discontinued therapy. The main reasons for discontinuation over 12 months were similar in biologic-naïve and biologic-failure patients, with 69.2% of discontinuations due to lack of efficacy in both groups, and 24.8% and 23.1% due to intolerance, respectively (online supplementary table S1). Crude retention rates (95% CIs) over 12 months were significantly higher in biologic-naïve versus biologic-failure patients (78.1% (74.7% to 81.2%) vs 69.9% (67.6% to 72.1%), respectively; P<0.001; figure 1A). In most cases, the biologic that failed was an anti-TNF agent. Crude retention rates over 12 months were higher in biologic-naïve patients versus patients who had failed 1 and ≥2 previous anti-TNF(s) (figure 1B).

(A) Crude retention rate over 12 months of abatacept treatment and (B) crude retention rate over 12 months of abatacept treatment by line of treatment. TNF, tumour necrosis factor.
Predictors of retention
Overall, 2201/2350 (93.7%) evaluable patients were considered for the multivariable analysis. In total, 18 clinically relevant variables, known risk factors and potential predictive factors for discontinuation in biologic-naïve patients, and 31 in biologic-failure patients, were identified from the univariable analysis and entered into the multivariable models.
For biologic-naïve patients, predictors of higher abatacept retention were RF and anti-CCP double positivity versus double negativity, and residence in Canada, Greece or Italy versus Germany as reference (figure 2). Neoplasms (mainly endocrine and breast) and psychiatric disorders (mainly depression) were associated with lower retention (figure 2).
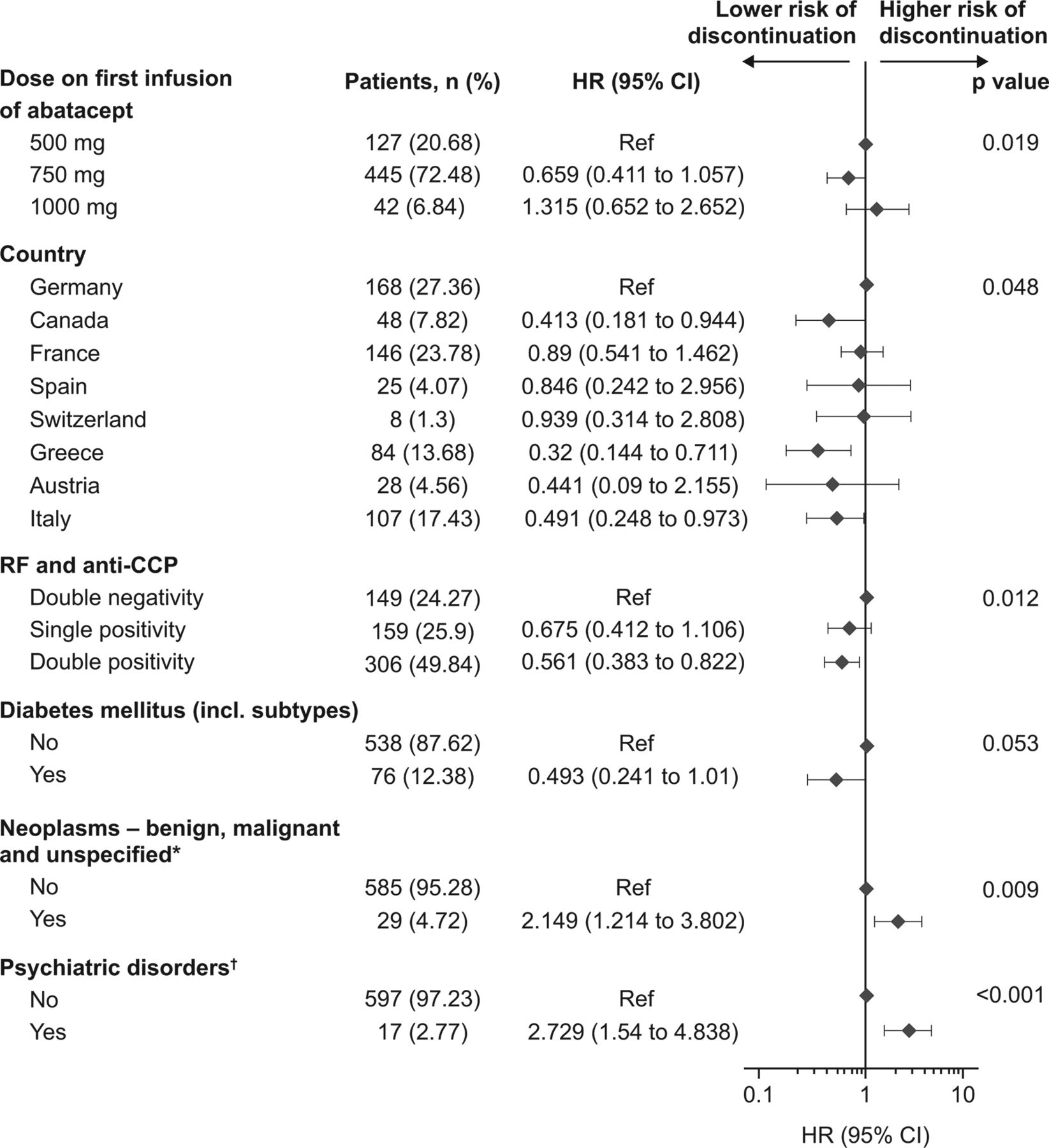
Multivariable model of abatacept retention in biologic-naïve patients. P values are pooled across each category. HRs are significant when the 95% CIs do not overlap 1. *Neoplasms were mainly endocrine and breast cancer. †Psychiatric disorders were mainly depression. CCP, cyclic citrullinated peptide; RF, rheumatoid factor.
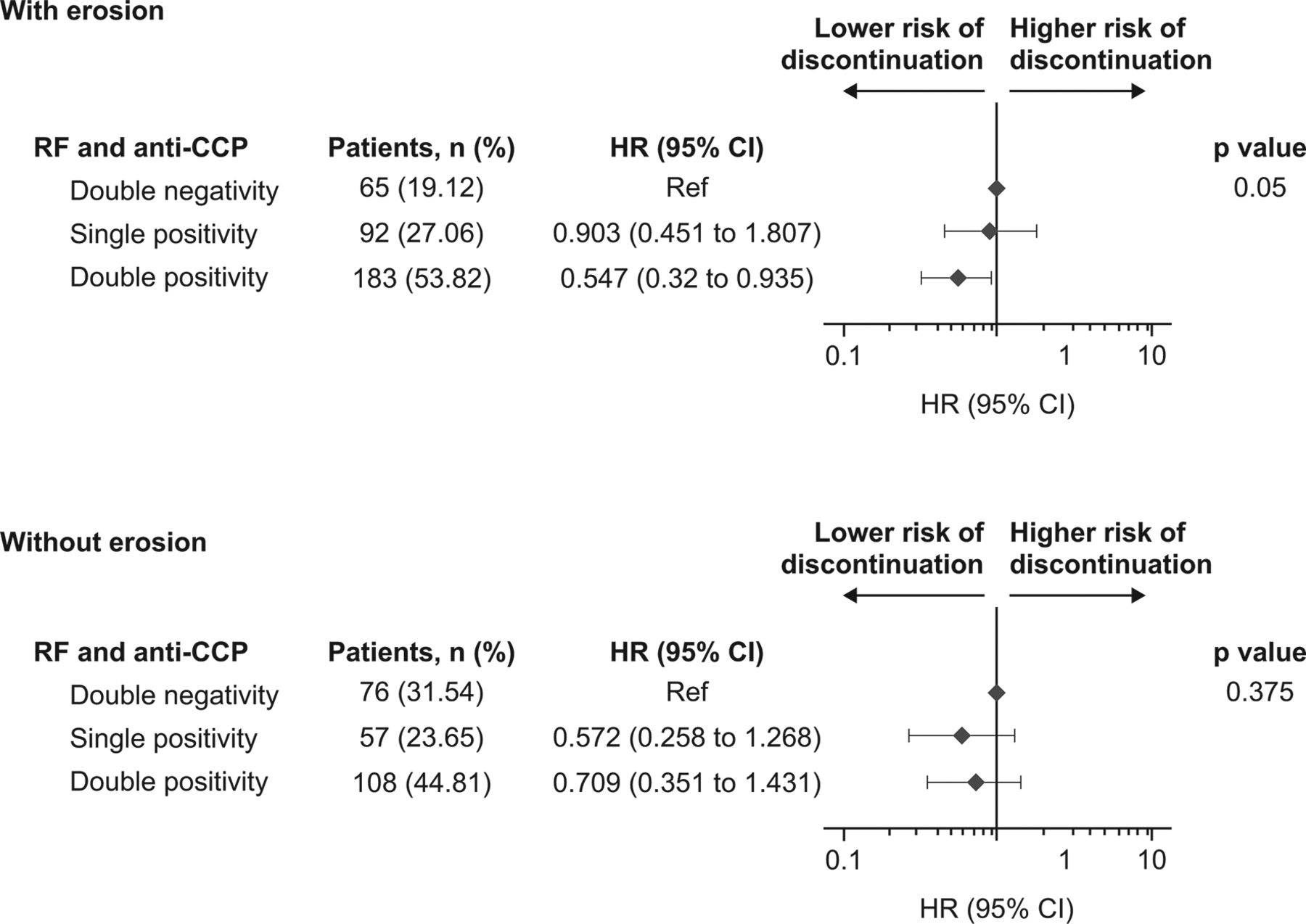
In an exploratory analysis, the known poor disease prognostic factors of seropositivity and joint erosions were also investigated. After stratification of biologic-naïve patients by baseline erosion status, RF and anti-CCP double positivity versus double negativity remained associated with higher retention only in patients with erosive disease at baseline (single positivity: HR (95% CI) 0.90 (0.45 to 1.81); double positivity: 0.55 (0.32 to 0.94); P=0.05; figure 3). When forced into the multivariable model, BMI did not significantly impact abatacept retention in the subgroups of biologic-naïve patients who were RF/anti-CCP double positive (BMI 25–<30 kg/m2: HR (95% CI) 0.49 (0.24 to 2.03); BMI≥30 kg/m2: 0.62 (0.28 to 1.38); P=0.142) or double negative (BMI 25–<30 kg/m2: 1.55 (0.45 to 3.00); BMI≥30 kg/m2: 0.64 (0.23 to 1.75); P=0.518) at baseline (online supplementary figure S4).

Multivariable model of abatacept retention by RF and anti-CCP status in biologic-naïve patients with or without radiographic erosion at baseline. P values are pooled across each category. HRs are significant when the 95% CIs do not overlap 1. CCP, cyclic citrullinated peptide; RF, rheumatoid factor.
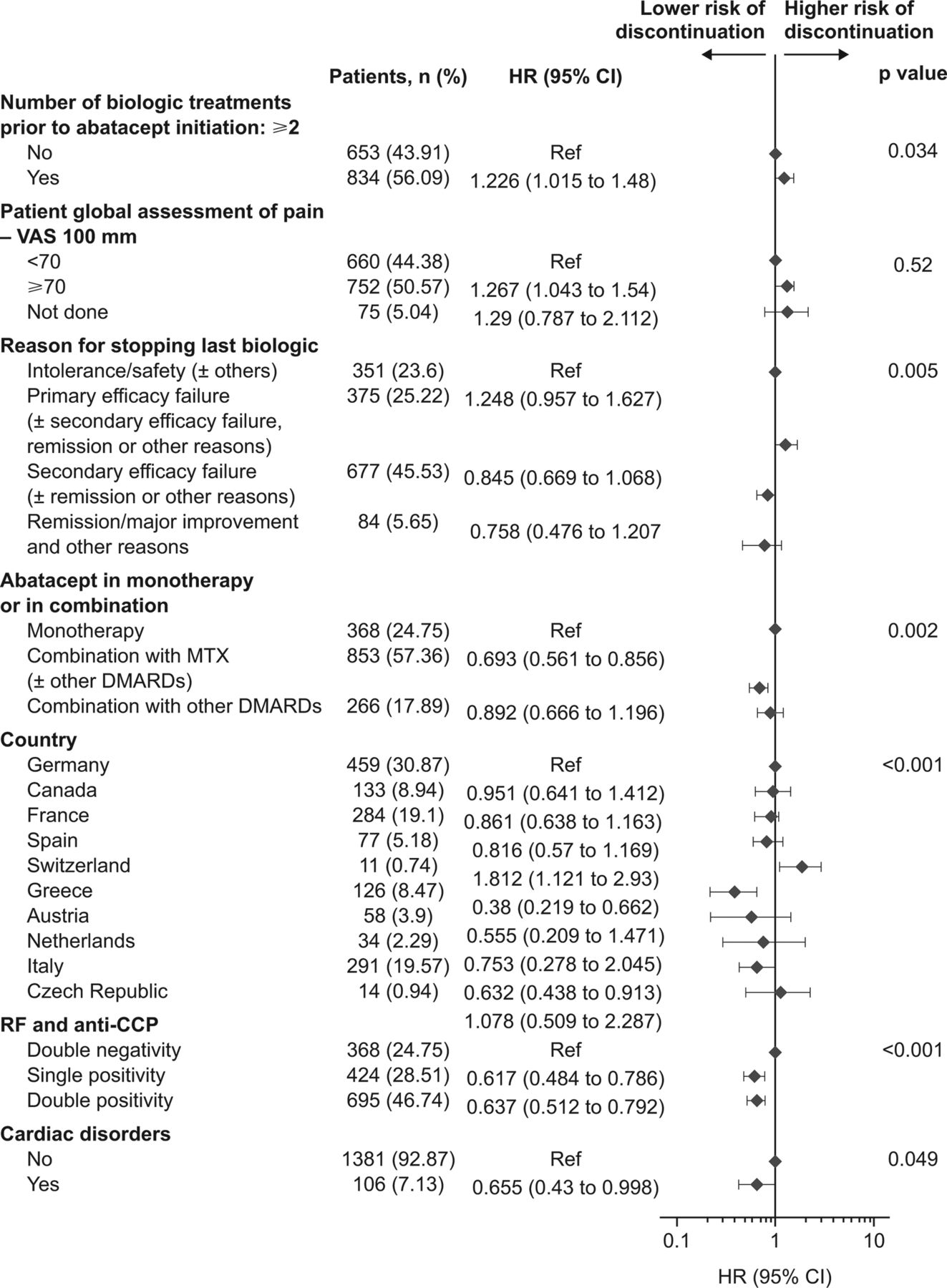
In biologic-failure patients, predictors of higher abatacept retention were RF and anti-CCP single and double positivity versus double negativity (P<0.001), country of residence (P<0.001), with residence in Greece (HR (95% CI) 0.38 (0.22 to 0.66)) or Italy (0.63 (0.44 to 0.91)) predicting higher retention versus Germany as a reference, MTX combination therapy with or without other conventional synthetic DMARDs versus abatacept monotherapy (0.69 (0.56 to 0.86); P=0.002) and cardiac disorders (0.66 (0.43 to 1.00); P=0.049; figure 4). Lower retention was associated with exposure to ≥2 prior biologics (HR 1.23; 95% CI 1.02 to 1.48; P=0.034), higher PtGA of pain score (≥70 mm on a Visual Analogue Scale; HR 1.27 (95% CI 1.04 to 1.54); P=0.520) and residence in Switzerland (HR 1.81; 95% CI 1.12 to 2.93) (figure 4). After stratification of biologic-failure patients by baseline erosion status, RF and anti-CCP double positivity versus double negativity remained associated with higher retention only in patients with erosive disease at baseline (single positivity: HR (95% CI) 0.55 (0.40 to 0.76); double positivity: 0.54 (0.40 to 0.73); P<0.001; online supplementary table S2). In the exploratory analysis, testing the impact of BMI on abatacept retention by RF/anti-CCP serostatus in biologic-failure patients generated similar results to those observed for biologic-naïve patients: no significant impact of BMI on abatacept retention was observed (data not shown).

Multivariable model of abatacept retention in biologic-failure patients. P values are pooled across each category. HRs are significant when the 95% CIs do not overlap 1. CCP, cyclic citrullinated peptide; DMARD, disease-modifying antirheumatic drug; MTX, methotrexate; RF, rheumatoid factor; VAS, Visual Analogue Scale.
Clinical efficacy of abatacept
At 12 months, a significantly greater proportion of biologic-naïve versus biologic-failure patients achieved a good or moderate EULAR response (83.8% vs 73.3%, P<0.001; figure 5). Remission, as defined by DAS28 (ESR or CRP)<2.6, CDAI, SDAI and Boolean criteria, was also achieved in a greater proportion of biologic-naïve versus biologic-failure patients (30.8% vs 21.9%, P=0.003; 44.5% vs 35.0%, P=0.004; 18.9% vs 12.6%, P=0.006; 18.4% vs 12.2%, P=0.01; and 15.0% vs 9.4%, P=0.01, respectively).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Percentage of patients achieving EULAR response* at 12 months by treatment line. n represents the number of patients with available data. *EULAR response was based on 28-joint Disease Activity Score, erythrocyte sedimentation rate or C reactive protein (collected). †Biologic-naïve versus biologic-failure patients who achieved a good or moderate EULAR response (83.8% vs 73.3%, P<0.001). EULAR, European League Against Rheumatism.
Safety
At the time of this 1-year interim analysis of ACTION, a total of 376 SAEs had been reported in 198 of 2364 patients evaluated (8.4%), leading to the discontinuation of abatacept in 95 (4.0%) patients. Overall, 26 deaths were reported during the treatment period (online supplementary table S3). Two deaths were due to an opportunistic infection (Pneumocystis jirovecii and Candida). Serious infections were reported in 76 patients (3.2%); there was one case of latent tuberculosis and four cases of opportunistic infections (two Pneumocystis jirovecii, one Cytomegalovirus, one Candida). The majority of serious infections were of the upper respiratory tract. A total of 24 neoplasms (benign, malignant and unspecified) were reported, two of which were pre-existing malignancies at baseline (brain malignancy and Bowen’s disease). Serious immune system disorders were reported in 20 patients, serious cardiac disorders in 17 patients and serious vascular disorders in 16 patients.
Discussion
As the number of available RA treatment regimens with unique mechanisms of action increases, a shift towards personalised medicine is necessary to ensure that patients receive the most appropriate treatment early in the course of disease to arrest or slow disease progression, and to prevent the accumulation of irreversible disability. Real-world, long-term treatment retention data in RA could serve as a surrogate measure of the benefit-to-risk ratio, complementing the data from the defined patient populations of randomised controlled trials with those from more diverse patient populations. In addition, the heterogeneous nature of both RA itself and the response to RA treatment highlights the value of predictors of treatment response in informed clinical decision-making.
This is the first analysis of ACTION to include a cohort of biologic-naïve patients for whom predictors of abatacept retention were detected using a multivariable analysis. In this analysis of a typical RA population with long-standing, erosive and moderate-to-severe disease, 12-month abatacept retention rates were higher in biologic-naïve versus biologic-failure patients (78% vs 70%, respectively), consistent with previous analyses of ACTION,5 and with independent registry data for abatacept.1 15 Higher retention rates in biologic-naïve versus biologic-failure patients with RA have similarly been reported for other biologics (76% vs 65% (infliximab), 72% vs 60% (etanercept), 68% vs 57% (adalimumab) and 81% vs 54%–66% (tocilizumab), respectively).16 17
Our analysis identified several predictors associated with higher rates of abatacept retention following 12 months of treatment in both biologic-naïve and biologic-failure patients, and included the poor prognostic factor of RF/anti-CCP double positivity.18 The predictors of abatacept retention identified in this analysis were similar to those identified in previous 12-month and 24-month interim analyses of biologic-failure patients enrolled in ACTION,5 8 and in other registry studies.3 6Patients who are anti-CCP positive tend to develop more severe, erosive disease.19 Interestingly, further investigation of the biologic-naïve and biologic-failure groups in this analysis revealed that RF/anti-CCP double positivity remained predictive of abatacept retention in patients with erosive disease at baseline, that is, in those with more than one poor prognostic factor and for whom a more aggressive approach to treatment is recommended.18
Anti-CCP and RF positivity have also been shown to be associated with a better clinical response to abatacept in both randomised clinical trials and real-world settings.7 20–25 In contrast, evidence for the effect of serostatus on retention or efficacy of anti-TNF agents and other biologics is conflicting.26–32
The association between response to abatacept and anti-CCP positivity is most intriguing. It could reflect the upstream mechanism of abatacept, whereby costimulation blockade inhibits T-helper cell activation with a subsequent impact on B cells and autoantibody production.33 34 Furthermore, seropositive and seronegative patients may differ in terms of disease heterogeneity. Compared with patients who are seronegative, seropositive patients may represent a more homogeneous population who are likely to respond to a treatment that targets underlying RA pathophysiology, such as abatacept.
Several studies have shown that obesity can negatively affect clinical response to anti-TNF agents and some other biologics in RA35–37; the effect of weight/BMI on tocilizumab efficacy is unclear.38 39 In contrast, in this analysis, BMI did not impact abatacept retention at 12 months in either biologic-naïve or biologic-failure patients, consistent with previous analyses of abatacept real-world data.3–5 Furthermore, BMI did not impact abatacept retention in either biologic-naïve or biologic-failure patients who were also seropositive for both RF and anti-CCP.
Among patients with RA, there is a high prevalence of comorbidities such as atherosclerosis-related cardiovascular diseases, some cancers and infections.40 Although the overall risk of malignancy is higher in patients with RA compared with the general population, this risk appears to be unaffected by treatment with abatacept or other biologics.41–44 In the current study, neoplasms (mainly endocrine and breast) and psychiatric disorders (mainly depression) were associated with lower retention in biologic-naïve patients, whereas cardiovascular disease was not associated with a higher risk of abatacept discontinuation, consistent with previous findings in biologic-failure patients.5 45 Any interpretation of these findings would be highly speculative; however, abatacept could be regarded as suitable for the treatment of RA in patients with cardiovascular disease. The long-term safety of intravenous abatacept is well established, and observational data suggest that the risk of acute myocardial infarction is lower in patients with RA initiating abatacept than in those initiating some anti-TNF agents.46 47 The question of the impact of comorbidities on drug retention does deserve further investigation.
Differences in abatacept retention by participating country were observed in this patient population, consistent with findings from a pooled analysis of data from European registries.1 In the absence of local reimbursement restrictions, these differences may be indicative of national variance in prescribing guidelines and clinical practice, access to biologics, cultural differences or in the regulatory approval of abatacept and other RA agents.1 48 49
Limitations of this analysis are inherent in observational real-world studies, including the absence of an active comparator and loss of patients to follow-up, which can result in a substantial number of missing clinical measurements. In addition, physicians may have waited longer before deciding that abatacept treatment was ineffective in patients who had an inadequate response to multiple biologic agents prior to initiating abatacept, potentially affecting the observed abatacept retention rate.
Conclusions
Higher abatacept retention and better clinical outcomes were seen in patients who received abatacept as the first-line biologic versus later treatment. RF/anti-CCP positivity was identified as a predictor for better retention in both biologic-naïve and biologic-failure patients, and RF/anti-CCP double positivity remained associated with higher retention in patients with erosive disease. BMI had no impact on abatacept retention in RF/anti-CCP double-positive biologic-naïve or biologic-failure patients. An increased awareness of the combined effect of predictive factors of treatment retention may support personalised, clinical decision-making in patients with moderate-to-severe RA in the real-world setting.
Consent to participate
The ACTION study was conducted in accordance with the Declaration of Helsinki and was consistent with the International Conference on Harmonisation Good Clinical Practice Guidelines50 and Good Epidemiological Practice Guidelines.51 Enrolled patients provided informed consent (written or not, according to the local laws), were aged over 18 years, of either sex, with an established diagnosis of moderate-to-severe RA as defined by the American College of Rheumatology 1987 revised criteria.10 Any patients already enrolled in an interventional RA clinical trial were excluded.
Acknowledgments
The authors would like to thank all physicians and patients who participated in the ACTION study. Clinical research organisations involved in the ACTION study were inVentiv Health Clinical, Winicker Norimed, TFS Trial Form Support S.r.1. and Archemin BVBA, and statistical analysis support was provided by Florence Mercier (Stat Process) and Julia Heitzman (Excelya). Professional medical writing support and editorial assistance was provided by Stacey Reeber at Caudex, and was funded by Bristol-Myers Squibb.
References
Footnotes
Contributors RA, XM, H-ML, MG, AC, HGN, MC, YE, CR, MLB: substantial contributions to the conception or design of the work; or the acquisition, analysis or interpretation of data for the work; RA, XM, H-ML, MG, AC, HGN, MC, YE, CR, MLB: drafting the work or revising it critically for important intellectual content; RA, XM, H-ML, MG, AC, HGN, MC, YE, CR, MLB: final approval of the version to be published; RA, XM, H-ML, MG, AC, HGN, MC, YE, CR, MLB: agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding This study was sponsored by Bristol-Myers Squibb.
Competing interests RA: grant/research support: Bristol-Myers Squibb; consultant: Bristol-Myers Squibb; speakers bureau: Bristol-Myers Squibb. XM: grant/research support: Biogen, GSK, Pfizer; speakers bureau: Bristol-Myers Squibb, GSK, Pfizer, sanofi, UCB. HML: consultant: AbbVie, Bristol-Myers Squibb, Roche-Chugai, UCB, MSD, GSK, Sobi, Medac, Novartis, Janssen-Cilag, AstraZeneca, Pfizer, Actelion; speakers bureau: AbbVie, Bristol-Myers Squibb, Roche-Chugai, UCB, MSD, GSK, Sobi, Medac, Novartis, Janssen-Cilag, AstraZeneca, Pfizer, Actelion. MG: none declared. AC: grant/research support: UCB, Pfizer; consultant: AbbVie, Bristol-Myers Squibb, Chugai, Lilly, MSD, Novartis, Pfizer, Roche. HGN: consultant: Bristol-Myers Squibb, AbbVie, Celgene, Janssen, Eli Lilly, Pfizer, MSD, Novartis, Roche; speakers bureau: Bristol-Myers Squibb, AbbVie, Celgene, Janssen, Eli Lilly, Pfizer, MSD, Novartis, Roche. MC: employee: Bristol-Myers Squibb. YE: consultant: Bristol-Myers Squibb. CR: shareholder and employee: Bristol-Myers Squibb. MLB: shareholder and employee: Bristol-Myers Squibb at time of study.
Ethics approval The study protocol and patient enrolment were approved by ethics committees and regulatory agencies in accordance with each country’s requirements. The central ethics committee that first approved the study on 31 January 2008 was the Munich, Bavaria, Germany, central ethics committee (approval number 07136). For each country, local ethics committee approvals were also obtained as required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.