Article Text

Abstract
Patients with rheumatoid arthritis (RA) are at increased risk of mortality compared with the general population. Evidence suggests that this increased mortality can largely be attributed to increased cardiovascular death. In a retrospective study of an inception cohort of RA patients in Rochester, MN, the contribution of traditional and RA-specific risk factors was investigated to this increased risk of cardiovascular morbidity and mortality. Several traditional cardiovascular risk factors were found to behave differently in RA patients. In addition, their associations with cardiovascular disease are weaker in RA patients as increased inflammation associated with RA also appears to contribute substantially to the increased cardiovascular mortality. Furthermore, the impact of disease-modifying antirheumatic drugs and biologicals on cardiovascular disease in RA patients is unclear. Cardiovascular risk scores for the general population may underestimate the risk for RA patients. Together with other studies that have demonstrated similar associations between RA and cardiovascular mortality, these data suggest that optimal control of cardiovascular risk factors is important, but not sufficient in RA patients. RA-specific cardiovascular risk prediction tools are needed, as well as clinical trials to assess the impact of therapies and tight control of inflammation in RA patients on cardiovascular outcomes and mortality.
Statistics from Altmetric.com
It is now well recognised that people with rheumatoid arthritis (RA) die prematurely.1 Recent evidence also suggests that the mortality gap between individuals with RA and those in the general population has been widening.2 In other words, individuals with RA have not enjoyed the improvements in survival that have been evident in the general population over the past few decades. The increased risk of mortality among individuals with RA occurs largely as a result of a higher risk of cardiovascular death, a higher risk of ischaemic heart disease, particularly silent myocardial infarction (MI) and sudden cardiac death as well as a higher risk and poor outcomes associated with heart failure. The goals of this paper are to: (1) review the contribution of traditional cardiovascular risk factors towards the excess cardiovascular death in RA; (2) to review the contribution of non-traditional risk factors (markers of inflammation, RA features) towards the excess cardiovascular risk in RA; and (3) to discuss the implications of these findings for the reduction of cardiovascular risk in RA. The epidemiological methods of the research to be discussed are summarised briefly below.
We have assembled a population-based incidence cohort of Olmsted County, Minnesota residents 18 years of age and older with RA ascertained according to the 1987 American College of Rheumatology diagnostic criteria. This cohort now contains 822 subjects with a mean follow-up of 14.2 years. We also assembled an age and gender-matched non-RA comparison cohort identified from the same underlying community. The non-RA cohort is composed of 603 subjects, with a mean follow-up of 16.8 years. Both cohorts have been followed up retrospectively through the complete medical records, and information on demographics, cardiovascular risk factors, comorbidities and RA characteristics were collected over the entire follow-up period noted above. In addition, information on cardiovascular outcomes, including cardiovascular death, ischaemic heart disease, heart failure and other clinical outcomes was ascertained. The prevalence of traditional risk factors at RA incidence was described by Gonzalez and colleagues.3 As seen in table 1, with the exception of cigarette smoking, which is more prevalent among RA subjects, the prevalence of traditional cardiovascular risk factors does not appear to differ between RA and non-RA subjects at the time of RA incidence. Likewise, the development of several cardiovascular risk factors over the follow-up period after disease onset is not significantly different when comparing RA and non-RA subjects for hypertension, high body mass index (BMI) or diabetes mellitus. However, hyperlipidaemia was found to be significantly less common over the follow-up period and low BMI was found to be significantly more common over the follow-up period among RA compared with non-RA subjects. Solomon and colleagues,4 using data from the Nurses Health Study, also demonstrated that most traditional cardiovascular risk factors were similar among patients with RA when compared with individuals without the disease. In summary, therefore, with the exception of smoking, the prevalence of many of the traditional cardiovascular risk factors is similar among RA and matched non-RA patients. Patients with RA are significantly more likely to develop low BMI and less likely to develop dyslipidaemia over the course of their disease when compared with non-RA patients. RA patients are at similar risk of developing hypertension, less likely to become obese and somewhat less likely to develop diabetes, although the latter differences were not statistically significant.
Prevalence of traditional cardiovascular risk factors at RA incidence in RA and non-RA patients
We next examined the impact of traditional risk factors on cardiovascular outcome. In these analyses, cardiovascular outcome was defined as a combined cardiovascular endpoint including MI, heart failure and cardiovascular death.3 These analyses illustrated that the relative impact of cardiovascular risk factors including male gender, current smoking, personal history of ischaemic heart disease, family history of ischaemic heart disease, hypertension, hyperlipidaemia, BMI greater than 30 kg/m2 and diabetes mellitus differed significantly in RA compared with non-RA subjects (fig 1). In particular, the relative impact of several of these risk factors appeared to be significantly less in RA subjects compared with non-RA subjects. Although the reasons for this are unclear, we posit the existence of a competing mechanism (perhaps related to chronic systemic inflammation), which imparts additional cardiovascular risk in RA but not in non-RA patients. The presence of an additional mechanism in RA but not in non-RA patients may result in an apparent dilution effect, making the relative contribution of each individual mechanism or risk factor appear smaller. These findings support the hypothesis that systemic inflammation is a major cardiovascular risk factor in RA.

Relative impact of traditional cardiovascular (CV) risk factors on combined cardiovascular endpoint in rheumatoid arthritis (RA) and non-RA subjects.3 BMI, body mass index.
Whereas BMI is considered a traditional cardiovascular risk factor, the relationship between BMI and cardiovascular mortality in individuals with RA is notable. As shown in fig 2, in the non-RA cohort, low BMI was not associated with an increased risk of cardiovascular death. Indeed, if anything, low BMI was somewhat protective against cardiovascular death. However, among RA patients, low BMI was associated with a threefold increased risk of cardiovascular death. This significant association remained even after adjusting for cardiac history, smoking, diabetes mellitus, hypertension and malignancy. Therefore, unlike the general population, low BMI in individuals with RA appears to be associated with a significant risk of cardiovascular death. As low BMI among individuals with RA may indicate active systemic inflammation, this finding lends further support to the hypothesis that inflammation plays a key role in the pathogenesis of cardiovascular death.5 Escalante and colleagues6 also reported on the “paradoxical effect of BMI on survival in persons with RA” demonstrating that as BMI declined so did survival probability among study subjects with RA.

Traditional cardiovascular risk factors in rheumatoid arthritis (RA) compared with non-RA patients—paradoxical effect of body mass index (BMI). HR, heart rate. Reproduced from Maradit Kremers et al5, with permission.
Lipids also appear to have a paradoxical effect on cardiovascular risk in individuals with RA. As shown in fig 3, total serum levels of cholesterol and low-density lipoprotein cholesterol decline precipitously during the 3–5-year period before RA incidence.7 The declines are significantly more marked than those observed in matched non-RA subjects (data not shown).

Traditional cardiovascular risk factors—paradoxical effect of lipids. LDL, low-density lipoprotein; RA, rheumatoid arthritis; Tch, total cholesterol.
Therefore, whereas the prevalence of traditional cardiovascular risk factors is similar in RA compared with non-RA subjects, their impact on cardiovascular outcomes, ie, the degree to which they impart a risk of heart disease, differs in RA compared with non-RA patients. Most cardiovascular risk factors appear to have weaker associations with heart disease in RA subjects and some risk factors have a paradoxical effect when compared with non-RA subjects. Clearly, more research is needed to understand better the mechanisms underlying these relationships.
In addition to traditional cardiovascular risk factors, we also evaluated the independent contribution of inflammatory indicators and RA characteristics towards the risk of cardiovascular death, after adjusting for the aforementioned traditional cardiovascular risk factors and after also adjusting for comorbidities.8 These analyses demonstrated that high erythrocyte sedimentation rate (ESR), small and large joint swelling, destructive changes on joint radiographs, rheumatoid nodules, vasculitis, rheumatoid lung disease and corticosteroid use were all statistically significantly associated with an increased risk of cardiovascular death after adjusting for cardiovascular risk factors and comorbidities. We have also previously examined the role of elevated ESR as a cardiovascular risk factor in RA. Analyses of ESR levels in 172 RA cases with heart failure demonstrated that the proportion with significantly elevated ESR (⩾40) was highest during the 6-month period before heart failure diagnosis compared with any other time over the entire follow-up period.9 These findings suggest that the 6-month period immediately preceding heart failure in RA cases is characterised by exceptionally high levels of systemic inflammation. We also examined the risk of cardiovascular outcome including MI, heart failure, vascular disease and cardiovascular death associated with rheumatoid factor (RF) positivity as well as antinuclear antibody (ANA) positivity in the Olmsted County general population both before and after the presence of rheumatoid disease. Statistical models were adjusted for age, sex, calendar year and comorbidity. These analyses demonstrated a significantly increased risk of the combined outcome of MI, heart failure or vascular disease as well as overall mortality in subjects testing positive for RF, even after adjusting for the presence of rheumatoid disease. These same relationships were seen for ANA-positive patients. The finding that RF and/or ANA positivity alone, even in the absence of rheumatoid disease, was a significant predictor of cardiovascular outcome suggests that immune dysregulation may promote cardiovascular risk not only in individuals with rheumatic disease but also in the general population.10 In summary, a number of inflammatory indicators, ie, characteristics of active RA such as joint swelling, vasculitis and RA lung, as well as high ESR and RF, represent significant independent risk factors for cardiovascular mortality and cardiovascular events in RA. RF and ANA appear to be associated with cardiovascular events and overall mortality even in the absence of rheumatoid diseases.
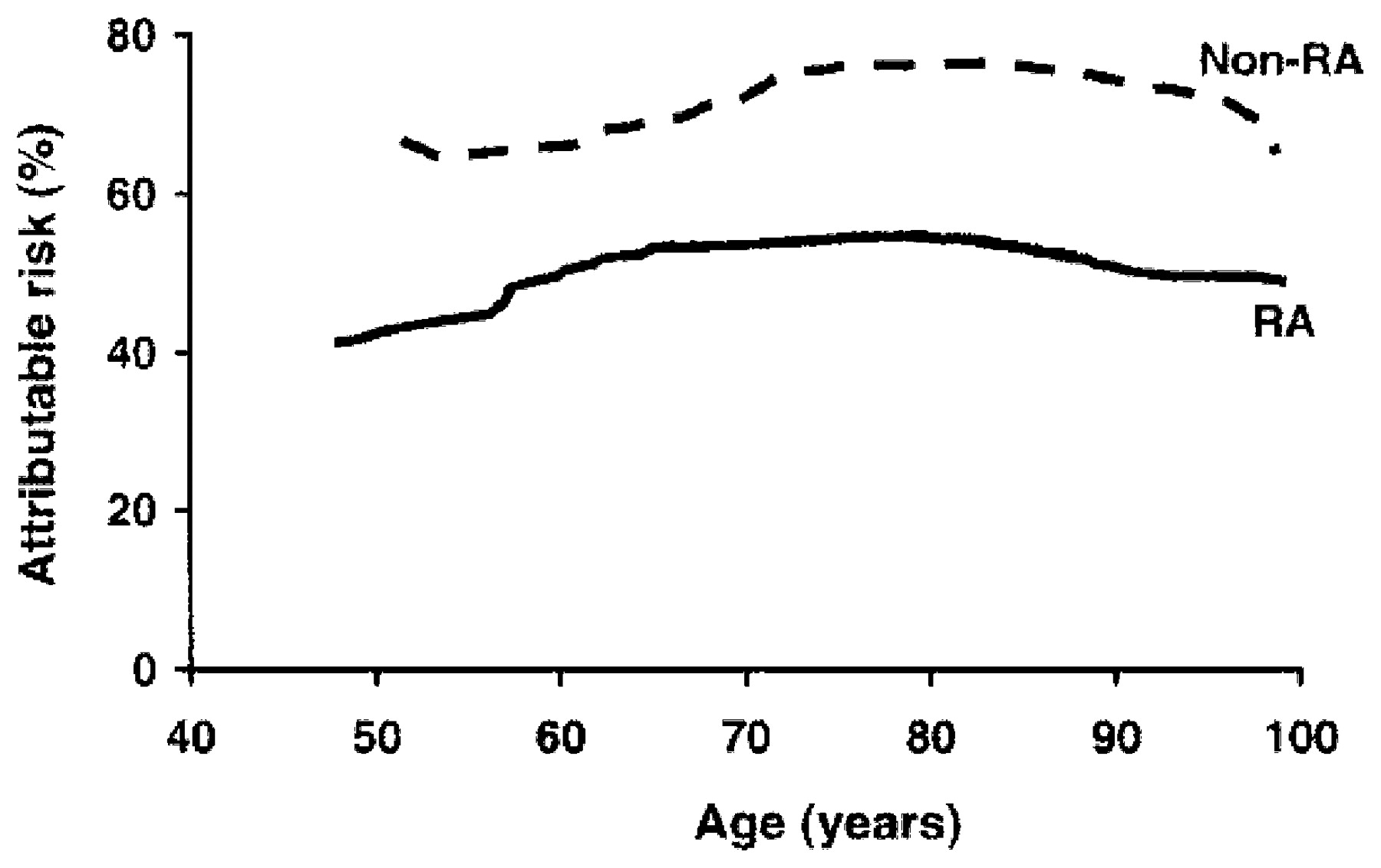
We then sought to determine how much of the increased incidence of heart disease in RA can be attributed to traditional (and thus potentially modifiable) cardiovascular risk factors such as smoking or hypertension. These analyses required the estimation of attributable risk or aetiological fraction, which is defined as the proportion of disease in a population that could, hypothetically, be prevented by the elimination of a risk factor. In this analysis, the outcome was heart failure. We first estimated how much of the heart failure risk is attributable to hypertension, and determined that to be approximately 60% in non-RA patients and 18–20% in RA patients. In other words, if all hypertension was eliminated, 60% of the heart failure risk would be eliminated among non-RA patients, whereas only 18–20% of the heart failure risk would be eliminated among RA patients. This analysis was repeated and summed for all cardiovascular risk factors, including a past history of ischaemic heart disease. As shown in fig 4, if all known cardiovascular risk factors and a past history of ischaemic heart disease were magically eliminated, that would eliminate approximately 80% of all heart failure risk among non-RA patients; however, it would only eliminate approximately 40% of the heart failure risk among RA patients.11 These results clearly demonstrate that a much larger proportion of the heart failure risk can be explained in non-RA compared with RA patients. Once again we posit that the systemic inflammation and immune dysregulation that characterise RA may represent the “unexplained risk” in RA patients.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
How much of the heart failure risk is attributable to all cardiovascular risk factors and ischaemic heart disease together in rheumatoid arthritis (RA) compared with non-RA patient? Reproduced from Crowson et al11, with permission.
Incidence of cardiovascular risk factors over follow-up in RA and non-RA patients
Maradit Kremers et al12 reported the 10-year absolute cardiovascular risk in individuals with RA and demonstrated that although relative risk information is useful, estimating the absolute risk by age group is much more clinically meaningful. In this analysis, we demonstrated a high 10-year absolute cardiovascular risk at RA onset across the four age groups from 40 to 80 years of age. When compared with non-RA, the absolute cardiovascular risk in RA patients was equivalent to that in non-RA patients who were 5–10 years older. These results, combined with the finding that traditional cardiovascular risk factors behave differently in RA patients (above), suggest that risk scores based on these traditional cardiovascular risk factors are likely to underestimate cardiovascular risk in RA. Indeed, such risk scores have been demonstrated to underestimate cardiovascular risk in other chronic diseases such as chronic kidney disease and diabetes.13 14 15 16
In conclusion, traditional cardiovascular risk factors are important in individuals with RA; however, they are relatively less important in terms of the risk they impart in RA compared with non-RA patients. Indeed, some risk factors may act in the opposite direction, as one would expect based on evidence from the general population. Inflammatory markers and markers of rheumatoid disease are highly significant predictors of cardiovascular outcome even after adjusting for demographics and cardiovascular risk factors. Together, these findings suggest that the systemic inflammation and immune dysregulation associated with RA appears to promote cardiovascular disease and cardiovascular death. These findings also suggest that effective, even optimal, control of traditional risk factors alone may be insufficient in reducing cardiovascular risk for individuals with RA, and highlight the need for RA-specific clinical risk prediction tools to estimate cardiovascular risk accurately in individuals with RA. Finally, the cardiovascular impact of immune modulating agents and especially biological agents used in the treatment of RA is unknown. Large simple trials are needed to elucidate the impact of these agents on cardiovascular outcomes and mortality.
REFERENCES
Footnotes
Funding This work was supported in part by grants from the National Institutes of Health (R01-R46849 and AR-30582) from the National Institute of Arthritis and Musculoskeletal Skin Diseases.
Competing interests None.
Provenance and Peer review Not commissioned; externally peer reviewed.