Article Text

Abstract
Background Aortic structural damage (ASD) may complicate the course of patients with giant cell arteritis (GCA). However the frequency and outcome of ASD has not been assessed in long term prospective studies.
Methods In a previous screening of 54 biopsy proven GCA patients, significant ASD was detected in 12 (22.2%) after a median follow-up of 5.4 years. These patients were periodically evaluated (every 4 years) over a median of 10.3 years (range 4–16.6 years) in order to investigate the development of new ASD and the outcome of previously detected abnormalities.
Results 18 of the 54 patients abandoned the study due to death or other reasons. The remaining 36 patients were subjected to a second screening and 14 to a third screening. 12 (33.3%) of the 36 patients re-screened and 16 (29.6%) of the initial cohort developed ASD, all but one in the thoracic aorta. Aortic diameters at the ascending and descending aorta significantly increased over time. One patient (1.9% of the initial cohort) died from aortic dissection. Surgery was advised in eight (50%) patients with ASD but could only be performed in three patients (37.7%). The development of ASD was not associated with persistence of detectable disease activity.
Conclusions The incidence of ASD is maximal within the first 5 years after diagnosis but continues developing over time, affecting up to 33.3% of individuals after long term follow-up. Once ASD occurs, dilatation increases over time, underlining the need for periodic evaluation. Surgical repair is feasible in about one-third of candidates.
- Systemic vasculitis
- Giant Cell Arteritis
- Cardiovascular Disease
- Corticosteroids
- Outcomes research
Statistics from Altmetric.com
Introduction
Giant cell arteritis (GCA) is a large vessel vasculitis in the elderly, typically targeting the cranial arteries.1 ,2 Aortic involvement by GCA has been sporadically reported in small necropsy studies or surgical series for decades3–5 but the prevalence of aortic inflammation in GCA has remained undefined until recently when the development of imaging techniques has allowed detection of aortitis at early disease stages, before the development of aortic complications requiring surgery or death.6–8 Using positron emission tomography or CT angiography, up to 45–65% of GCA patients can be identified exhibiting radiological signs of aortic inflammation at the time of diagnosis.6–8 Aortitis is usually asymptomatic but may lead to subsequent aortic structural damage (ASD) with the potential for catastrophic events, such as aneurysm rupture or dissection.9–12
In a retrospective, population based study, Evans et al9 found that GCA patients were 17.3 times more likely to develop thoracic aortic aneurysms and 2.4 times more likely to develop abdominal aortic aneurysms than individuals of similar age and gender from the general population. Subsequent studies have estimated that 9.5–18% of GCA patients develop aortic aneurysm or dissection.10 ,11 However, the retrospective nature of these studies where patients were not routinely imaged might have underestimated the prevalence of aortic complications. In 54 GCA patients systematically subjected to a defined screening protocol, significant ASD was detected in 12 (22.5%) after a median follow-up of 5.4 years (range 4–10.5 years).12
The development of significant ASD is challenging due to the life threatening nature of its complications13 and the difficulties in performing aortic reconstructive surgery in aged individuals. The natural history of aortic dilatation in GCA is not well known and has not been prospectively investigated. According to retrospective studies, although aortic dissection may occur early in the course of the disease, aortic dilatation appears to be more frequently a delayed complication.9–12 The frequency of aortic related life threatening complications is not known, and therefore, whether or not aortic dilatation conveys an increased mortality in aged patients with a naturally limited lifespan has not been clearly defined. Moreover, feasibility and outcome of reconstructive surgery in these patients has not been evaluated. Answers to these questions are seminal to establish recommendations about systematic population screening.14
The aim of this study was to perform a prospective longitudinal evaluation of a patient cohort previously screened for ASD in order to assess the development of new ASD and the outcome of previously detected abnormalities over an extended follow-up period.
Patients and methods
Study population and screening protocol
The study group comprised 54 patients (14 men and 40 women) with biopsy proven GCA systematically screened for ASD, 5.4 years (range 4.0–10.5 years) after diagnosis. The results of the first screening have been published previously.12 After this initial assessment, patients were subjected to a longitudinal, prospective follow-up and the same screening protocol was performed approximately every 4 years. If relevant ASD was detected in the initial screening, additional imaging was performed when judged appropriate by the consultant cardiovascular surgeon. All patients were treated and followed by the authors according to uniform criteria.12 The screening protocol consisted of a medical evaluation and routine blood tests, including acute phase reactants. Serum concentrations of proinflammatory cytokines (interleukin 6 and tumour necrosis factor α) were measured by immunoassay according to the manufacturer's instructions (R&D Systems, Minneapolis, USA). A chest x-ray was performed in all patients and compared with that obtained at the time of diagnosis. When aortic dilatation or changes with respect to previous radiographs were suspected, even minimal or questionable, a contrast enhanced spiral chest CT scan was performed and aortic diameters were measured at different segments. The abdominal aorta was evaluated by ultrasonography (US). CT and ultrasonography results were compared with those obtained at the initial screening. As previously stated, significant ASD was defined as focal dilatation (saccular or fusiform aneurysm) or, in the case of diffuse dilatation, when the aortic diameter exceeded 4 cm at the ascending aorta or reached at least 4 cm in the aortic arch/descending aorta or 3 cm at the abdominal aorta.8 ,15 Clinical data recorded included number of relapses, time to first relapse, time required to achieve a maintenance prednisone dose <10 mg/day and time to complete prednisone withdrawal. Relapses were defined as recurrence of cranial, polymyalgic or systemic symptoms, including anaemia not attributable to other causes, which completely resolved by increasing prednisone 10 mg above the previously effective dose. Relapses were usually accompanied by mild to marked increases in acute phase reactants. However, isolated variations in erythrocyte sedimentation rate or C reactive protein were not considered relapses unless the above mentioned disease features appeared. Number and cause of deaths and survival time from GCA diagnosis were also recorded.
Statistical analysis
Comparisons between groups were performed using a t test for continuous variables and Fisher's exact test for categorical variables. Time to first relapse, time required to achieving a maintenance prednisone dose <10 mg/day, time to complete prednisone withdrawal and time to death were analysed by Kaplan–Meier survival analysis and compared using the log rank test.
Results
Development of aortic dilatation over time
The initial cohort of 54 patients was prospectively followed for a median of 10.3 years (range 4–16.6 years), until death, dropout, the third screening or March 2013. During the study period and before the second screening, 18 of the 54 patients died or abandoned the study for major logistical difficulties in continuing visits at a referral centre (figure 1). A second screening was completed in the remaining 36 patients (10 men and 26 women; 66.6% of the initial cohort) after a median follow-up of 8.7 years (range 6.9–13.6 years). Seven of these patients dropped out before the third screening (figure 1) which, to date, has been completed in 14 patients (median follow-up 12.8 years, range 10.3–16 years). The remaining 15 patients will be eventually re-screened within the next 2 years if they continue their scheduled appointments.

Flowchart of the outcome of the study cohort. A remarkable drop out occurred during the study period, due to advanced age of the study population. GCA, giant cell arteritis.
During the overall study duration, 12 (33.3%) of the 36 patients who completed the second or third screenings and 16 (29.6%) of the 54 patients encompassing the initial cohort, developed ASD. In 12 patients, ASD was detected at the first screening, in three at the second assessment and in one at the third evaluation. Figure 2A shows the percentage of patients who developed ASD over time.

Patient outcome according to the presence or absence of aortic structural damage (ASD). (A) Percentage of patients with ASD over time (weeks). (B) Percentage of patients alive over time (weeks). (C) Relapse free survival. (D) Proportion of patients receiving glucocorticoid therapy over time (weeks).
Table 1 summarises the characteristics and outcome of ASD in these patients. In 15 of the 16 patients with ASD, dilatation was found in the thoracic aorta, and only one patient had a small fusiform aneurysm located at the abdominal aorta that remained stable over time. This aneurysm was detected at the first screening. It is unclear whether this aneurysm was related to GCA or to atherosclerotic disease. No abdominal aneurysms were detected in additional patients during follow-up.
Characteristics of aortic structural damage during follow-up
Outcome of aortic dilatation over time
According to the screening protocol designed for potential general use, assessment of the thoracic aorta was initially based on a chest x-ray. However, 44 (81.5%) of the 54 patients underwent a CT scan at some point during follow-up because of a slight, moderate or high suspicion of aortic dilatation, allowing accurate measurements of the aortic diameters. As shown in table 1, aortic diameters increased over time in patients with ASD. Table 2 shows aortic diameters at various segments of the thoracic aorta in 17 patients who underwent a CT scan in both the first and second screenings. A significant increase in the diameters of the ascending and descending aorta was observed. This was at the expenses of patients with ASD in the first CT scan, indicating progressive dilatation over time of the damaged aortic segments.
Diameters of the thoracic aorta in 17 patients subjected to CT scan at the first and second screenings
Aortic reconstructive surgery
At the end of the follow-up period, eight (50%) of the 16 discovered dilatations were candidates for elective surgery, according to general consensus guidelines for surgical repair of aneurysmal disease.16 However, aortic reconstructive surgery was performed in only three patients (37.5% of candidates for surgery, 18.8% of those with dilatation and 5.5% of the entire patient cohort). In the remaining five, surgery was not advised because of advanced age and comorbidities (three patients) or patients themselves declined intervention after being informed of the potential risks (two patients). One of the three patients who underwent surgical repair of an ascending aortic aneurysm exhibited diffuse dilatation of the aortic segments distal to the aortic prosthesis at the second screening. Another patient suddenly died 6 months after surgery.
Patient mortality according to ASD
Forty-one of the 54 patients were followed until the end of the study or death, and 13 abandoned the study (figure 1). During the study period, at least 12 patients (22.2% of the initial cohort) died. One patient developed an aortic dissection and died shortly after the discovery of an ascending thoracic aneurysm at the second screening which, at that time, was not considered large enough to warrant surgery. At the time of death, the patient was in stable remission and had been able to withdraw corticosteroids 5 years before. This death was considered GCA related. As shown in figure 1, eight additional deaths were unrelated to GCA and three were sudden deaths at the patient’s home, including the above mentioned patient who underwent aortic repair 6 months before. Necropsy studies of these three patients were not performed and an acute aortic complication as the cause of death cannot be confirmed or ruled out. Therefore, mortality directly related to aortic complications in our patient cohort was at least 1.9%.
Extended follow-up of the original cohort showed a trend towards an increased mortality (any cause) among patients with ASD although differences did not reach statistical significance (figure 2B).
Development of ASD and disease activity
There were no significant differences in follow-up duration between patients who did or did not develop ASD (9.8 ± 3.1 vs 10.7 ± 3.1 years, NS).
At the end of the follow-up period, 11 patients achieved sustained remission with no relapses and 43 patients experienced at least one (median 2, range 0–7). The proportion of patients in sustained remission throughout the study period was significantly higher among patients with ASD (figure 2C). Accordingly, ASD was more frequent among patients without recurrences (73%) compared with those who had experienced at least one relapse (16%) (RR 4.47, 95% CI 2.07 to 9.63, p=0.001).
Patients who developed ASD suffered significantly lower numbers of relapses than patients without ASD (mean 0.9 ± 1.2 vs 2 ± 1.5, p=0.006) during the study period.
At the end of the follow-up period, 36 patients had been able to withdraw therapy and 18 patients were still on prednisone (median 2.5 mg/day, range 1.25–12.5). Only one of the patients who developed ASD was receiving corticosteroids at the end of follow-up (6.2 years). Patients who developed ASD needed shorter periods of time to achieve a maintenance prednisone dose lower than 10 mg/day than patients without ASD (mean 45±32 vs 79±65 weeks, p=0.015) and to completely withdraw therapy (mean 213 ± 37 vs 423 ± 41 weeks, p=0.001) (figure 2D). The overall dose of prednisone required at the end of follow-up was also lower among patients who developed ASD (9.5 ± 4 vs 15.4 ± 7.1 g, p<0.001).
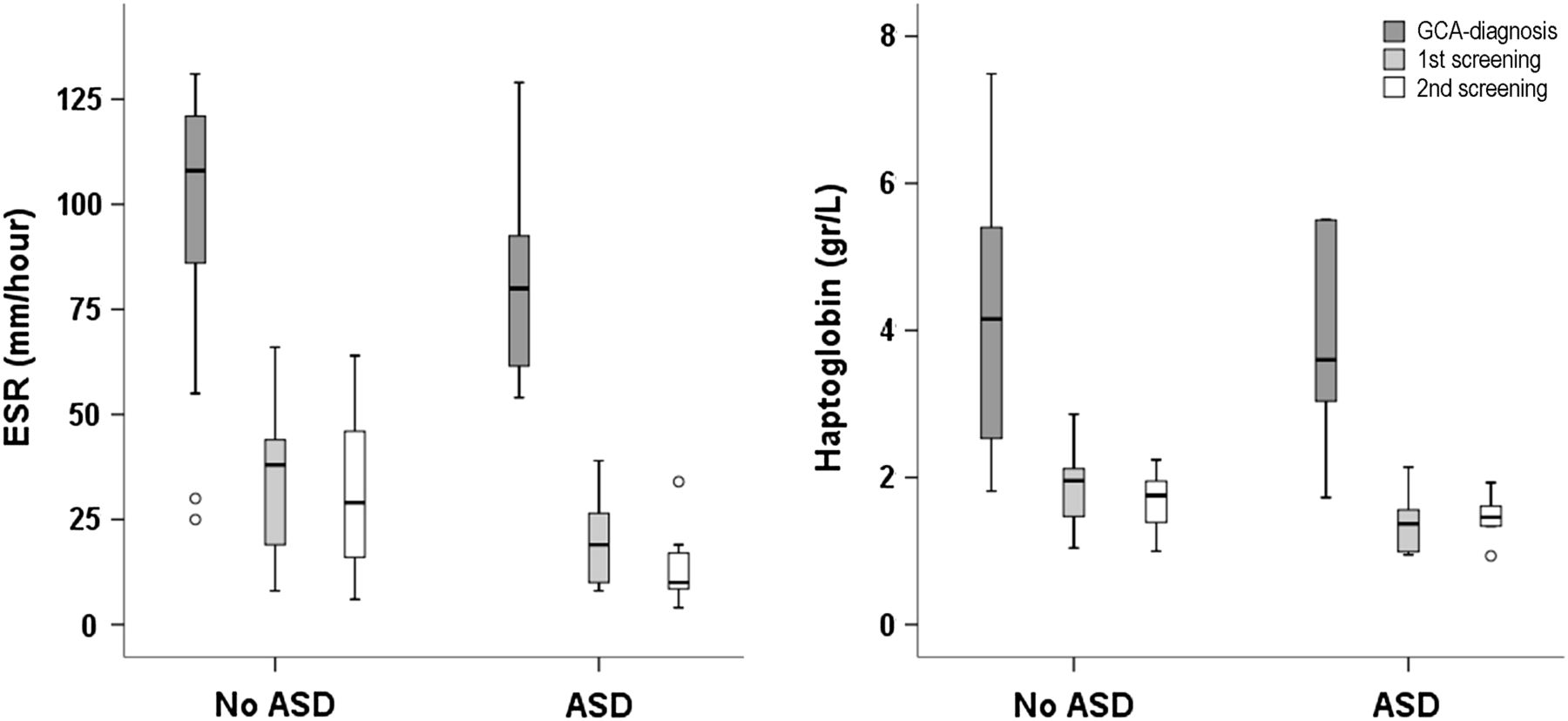
Patients who developed ASD exhibited lower levels of the acute phase reactants erythrocyte sedimentation rate and haptoglobin at different time points compared with patients who did not develop aortic dilatation (figure 3). C reactive protein and proinflammatory cytokines (interleukin 6 and tumour necrosis factor α) concentrations did not show significant differences between groups (data not shown).

Erythrocyte sedimentation rate (ESR) and haptoglobin concentrations at various time points (diagnosis, first screening and second screening) in patients with or without aortic structural damage (ASD). p<0.05 for the following comparisons: ESR 1st screening, ESR 2nd screening and haptoglobin 2nd screening. GCA, giant cell arteritis.
Histopathological examination of aortic specimens
During the study period, histopathological evaluation of the aortic wall was performed in six patients during surgery or necropsy. Three had undergone reconstructive surgery of an ascending aortic aneurysm. Two patients died from GCA unrelated conditions but one also had an ascending aortic aneurysm. Finally, as mentioned above, one patient developed aortic dissection and died. Aortic specimens were obtained a median of 9.2 years (range 5.1–11.1 years) after GCA diagnosis. All of these patients were in stable remission and had been able to withdraw corticosteroid therapy. Two patients exhibited severe atherosclerosis of the aorta. None of the aortic samples exhibited dense inflammatory infiltrates in the media, suggestive of significant ongoing inflammation. Only two patients exhibited scattered mild inflammatory infiltrates at the media. The most striking finding was the significant loss and disarray of elastic fibres, even in areas devoid of current inflammation (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Serial findings in a patient with giant cell arteritis and aortic aneurysm. (A) Chest x-ray at the time of the first screening did not show aortic abnormalities. (B) Chest x-ray at the time of the second screening was suggestive of aortic enlargement. (C) The CT scan demonstrated an aortic aneurysm at the ascending aorta (50 mm). (D) A few months later, the patient developed an aortic dissection and died. (E, F) Histopathological examination of the aortic wall with haematoxylin/eosin (H/E) and orcein staining exhibited loss and disorganisation of elastic fibres in the absence of inflammatory infiltrates.
Discussion
Aortic involvement by GCA has received a great deal of attention due to the life threatening nature of its potential complications.1–3 However, the prevalence, timing and long term outcome of ASD are not well known. In addition, as most patients with GCA are elderly and, consequently, with a limited lifespan and at increased risk for major surgery, the clinical relevance and therapeutic impact of discovering ASD in patients with GCA are unclear. The lack of prospective long term follow-up studies prevents the design of specific recommendations about whether or not GCA patients should be systematically screened, what would be the best cost effective screening method and how often this should be applied.14
This is the first prospective study to assess the development and outcome of ASD over a long period of time. Nearly one-third of the initial cohort, and 33.3% of those who completed successive screenings, developed significant ASD during the entire follow-up period, representing a much higher prevalence of aortic aneurysm/dilatation than previously observed in retrospective surveys.9–11 ,17
Similarly to previous studies, clinically significant aortic dilatation predominated at the ascending aorta.9–11 ,17 However, CT was able to detect subtle structural abnormalities, such as non-significant dilatation (<4 cm) or thickening of the aortic wall, at other segments (data not shown), suggesting previous inflammatory involvement of larger portions of the aorta, as has been demonstrated in necropsy studies or, more recently, by imaging techniques.6–8
The chronology of ASD development has not been well defined. A prospective study of aortic involvement in newly diagnosed patients showed that only 15% have some aortic dilatation at the time of diagnosis.8 This is in contrast with the remarkable prevalence of aortic dilatation during long term follow-up found in the present study and supports the concept that ASD is a delayed complication. As found in a recently published retrospective study,17 the majority of dilatations occurred during the first 5 years, but continued to occur thereafter. Moreover, existing dilatations progressively increased in size over time. Confirmed dissection occurred in only one patient but aortic complications may have accounted for some of the reported sudden deaths. Overall mortality tended to be higher in patients with ASD but differences were not significant, possibly influenced by the limited size of our cohort. Recently published retrospective studies have also suggested increased mortality among patients with aortitis18 or aortic dilatation.17
In about half of the discovered dilatations, surgical repair was advised, according to current guidelines16 but this could be applied to only one-third of candidates. The number of patients subjected to repair was too low to draw conclusions about the advantages of elective surgery. Surgery was followed by distal dilatation of the remaining aorta in one patient and sudden death 6 months later in another.
In our series, extended follow-up confirmed that development of significant ASD was not associated with persistence of clinically or analytically detectable disease activity.12 Late aortic dilatation frequently occurred in patients who had achieved sustained remission. Intriguingly, and as observed in the first screening,12 patients who developed significant ASD experienced fewer relapses and were able to withdraw therapy earlier than patients who did not develop significant ASD. It has been postulated that smouldering inflammatory activity, not clinically detectable, may progressively destroy the aortic wall. Chronic use of low dose glucocorticoids might then prevent aortic damage. However, patients with ASD exhibited lower concentrations of acute phase reactants, not only at diagnosis but also at various time points during follow-up than patients without aortic dilatation.12 Moreover, histopathological examination of aortic specimens obtained from six patients disclosed extensive destruction of elastic fibres as the main feature and slight residual inflammatory infiltrates were only observed in two patients. These findings suggest that persistence of inflammatory activity may not be the only or more determinant factor in aortic dilatation and that the characteristics and aggressiveness of the initial inflammation along with deficiencies in subsequent vascular remodelling may have a major role in the development of aortic dilatation.19–21 As previously suggested, haemodynamic factors may also contribute.8 Abnormalities in vascular remodelling may turn the aortic wall into a weakened structure that may undergo progressive dilatation, mainly at the ascending portion where mechanical forces are greater.8 ,20 ,21
In summary, the development of ASD seems to be much more frequent than suggested in retrospective studies. Although the maximal incidence appears to occur within the first 5 years after diagnosis, dilatation may develop subsequently. Moreover, existing dilatations increase in size over time. Therefore, it seems reasonable to periodically screen GCA patients, particularly those in a good general condition who could be eligible for surgery if needed and in whom aortic complications may reduce their life expectancy. The best approach and frequency of performing this surveillance have not been established. Our findings suggest that a simple chest x-ray may be sufficient for a population wide initial screening but this needs to be confirmed in larger studies. Feasibility and outcome of elective surgery needs to be further investigated. It remains to be elucidated whether the duration of low dose glucocorticoid therapy may influence the development of ASD and the risk/benefit of prolonged glucocorticosteroid treatment if that was the case. Moreover, new therapies tested in GCA patients should be evaluated for their ability to reduce the risk of subsequent dilatation as an important outcome measure.22 ,23
References
Footnotes
-
Handling editor Tore K Kvien
-
The results were presented in part at the 72nd ACR Annual Scientific Meeting (San Francisco, 2008), the 14th International Vasculitis and ANCA Workshop (Lund, 2009) and the Annual European Congress of Rheumatology (Berlin, 2012).
-
Contributors AG-M, SP-G, JH-R and MCC designed the study. PA, GE-F, MAA, MB, IT-B, AG-M, JH-R and MCC generated the data. AG-M and MCC drafted the manuscript. All authors reviewed and commented on the data. All authors read, commented on and approved the manuscript.
-
Funding Supported by Ministerio de Ciencia y Tecnología) (SAF 08/04328) and Ministerio de Economía y Competitividad (SAF 11/30073). AG-M, GE-F, MB, IT-B and SP-G were supported by a research award from Hospital Clínic. AG-M was supported by Fundació Pedro Pons. GE-F and MCC were supported by Instituto de Salud Carlos III.
-
Competing interests None.
-
Ethics approval The study was approved by the ethics committee of Hospital Clinic.
-
Provenance and peer review Not commissioned; externally peer reviewed.