Article Text

Abstract
Objective: Dehydroepiandrosterone (DHEA) administration has been reported to improve fatigue, psychological distress, and physical disability. These are common features of primary Sjögren syndrome (pSS). We investigated the effects of DHEA administration on fatigue, well-being, and functioning in women with pSS.
Methods: In a double-blind, randomised placebo-controlled clinical trial, 60 female patients with pSS received 200 mg oral DHEA or placebo. Primary outcome measures were general fatigue, depressive mood, mental well-being, and physical functioning. In addition, pain, sicca complaints and disease activity parameters were measured. Patients were assessed before treatment, after 3, 6, and 12 months on study medication, and 6 months after cessation of treatment.
Results: Patients from both the DHEA- and placebo-treated group improved on general fatigue (p<0.001), mental well-being (p = 0.04), and depressive mood (p = 0.008). Physical functioning did not change (p = 0.44). Of the secondary outcome variables, complaints of a dry mouth diminished during treatment in both groups (p = 0.006), the erythrocyte sedimentation rate showed a decrease for the DHEA group (p = 0.02), and complaints of dry eyes improved in the placebo group (p = 0.01). The belief to have used DHEA was a stronger predictor for improvement of fatigue and well-being than the actual use of DHEA.
Conclusions: Our study does not support a superior effect of DHEA over placebo in female patients with pSS. Both DHEA and placebo induce improvement of fatigue and well-being. This may suggest possibilities for cognitive behavioural interventions.
Statistics from Altmetric.com
The chronic autoimmune disorder primary Sjögren syndrome (pSS) is characterised by lymphocytic infiltration of exocrine glands. Hallmark symptoms are dryness of the eyes (keratoconjuncivitis sicca) and mouth (xerostomia). The disease has female preponderance and manifests itself most frequently in the fourth and fifth decade of life.1 Many patients with pSS experience disabling fatigue and reduced mental well-being and physical functioning.2–6 Chronic widespread pain is frequent with 10 to 55 percent of patients fulfilling the criteria of fibromyalgia.7
Attention has been drawn to the influence of dehydroepiandrosterone (DHEA) and its sulfate ester DHEAS on autoimmune diseases.8 DHEA and DHEAS are weak androgens secreted by human adrenal glands in response to adrenocorticotrophic hormone. DHEA administration can improve fatigue and well-being in elderly9–11 and in a variety of disease states.12–17 In female patients with systemic lupus erythaematosus (SLE), improved well-being and fatigue18 and reduced disease activity19 20 were observed with oral DHEA (200 mg per day).
Women with pSS appear androgen deficient.21 22 Reduced serum levels of DHEA or DHEAS were observed as well as a correlation between circulating levels of DHEAS and mental well-being.21 23 Androgens suppressed inflammation in a mouse model of Sjögren syndrome.24 Based on these previous studies, we expected to find, in a randomised double-blind placebo-controlled study, beneficial effects of daily oral administration of 200 mg DHEA on fatigue, well-being, and functioning in women with pSS.
METHODS
Design
In a double-blind, randomised placebo-controlled clinical trial, patients received 200 mg oral DHEA (Fagron, Nieuwerkerk a/d IJssel, The Netherlands) or placebo during one year. At baseline, after 3, 6, and 12 months on study medication, and 6 months after cessation of treatment, patients had a physical examination (by AH), filled out questionnaires, and donated blood. Patients who stopped medication intake prematurely were evaluated 6 months after the last capsule was taken, and these data were considered as being obtained at 18 months. Patients, physicians, and researchers were blinded to the treatment.
Participants
Patients were recruited from the outpatient clinics of the departments of Rheumatology and Clinical Immunology of the University Medical Centers in Utrecht and Groningen, The Netherlands. The study was approved by the institutional review boards of both hospitals, and all participants provided written informed consent.
Charts of 395 patients with sicca complaints were evaluated for eligibility resulting in 155 eligible women, who fulfilled the European criteria for classification of pSS including a focus score ⩾1 on minor salivary gland biopsy,25 and were ⩾18 years. Exclusion criteria were pregnancy or wish to conceive, a malignancy within the preceding 5 years, use of glucocorticosteroids in the preceding year, and abnormal thyroid stimulating hormone (TSH), serum creatinin, or liver function.
Outcome variables
The primary outcome measures were general fatigue, depressive mood, physical functioning, and mental well-being. For the general fatigue scale of the Multidimensional Fatigue Inventory (MFI, range 4–20),26 patients responded to four statements indicating fatigue during the previous 3 days (range 1–5). The Zung self-rating scale (range, 20–80) assessed affective, psychological, and somatic characteristics of depressive mood;27 patients responded to 20 statements (range 1–4). The RAND (short form-36, SF-36) Health Survey28 was used to measure physical component summary (PCS) and mental component summary (MCS) scores.29
Secondary outcome measures were self-reported pain and ocular and oral dryness, presence of fibromyalgia, tear production, and surrogate parameters of disease activity: erythrocyte sedimentation rate (ESR), haemoglobin concentration, and serum- immunoglobulin-G (serum-IgG). Patients indicated on a 100 mm visual analogue scale (VAS) their pain during the last 2 days between the extremes “no pain” (0 mm) and “the most pain ever” (100 mm), and the degree of ocular and oral dryness between the extremes “not troublesome” (0 mm) and “extremely troublesome” (100 mm). Tender point count was performed according to the criteria for fibromyalgia.30 The Schirmer I test was used to measure mean tear production.25 ESR, haemoglobin concentration, and serum-IgG were determined according to standard procedures.
Control variables
Laboratory tests included whole blood count, serum creatinin, gamma glutamic transpeptidase (GGT), and alanine aminotransferase (ALT) according to standard procedures.
DHEAS levels were measured using an Advantage chemiluminescense system (Nichols Institute Diagnostics, San Juan Capistrano, California, USA). The lower limit of detection was 0.2 µmol/L and interassay variation <11%. Normal values in our laboratory are 0.5–9 µmol/L. Testosterone was measured after diethylether extraction using an in house competitive radio-immunoassay with a polyclonal antibody with [1,2-3H(N)]-Testosterone as a tracer. The lower limit of detection was 0.12 nmol/L, interassay variation 5–7%, and crossreactivity to DHEA <0,1%. Samples were stored at −80°C and analysed in single runs.
Patients indicated if they had noted, as compared to pretreatment, an increase in body hair, acne, oily skin or capital hair, or changes in the regularity or duration of the menstrual cycle or postmenopausal blood loss.
At the 18 month visit, when the patients were able to judge their status during and after treatment, they indicated whether they believed they had used DHEA or placebo.
Statistical analysis
Patients were analysed on an intention-to-treat basis; for missing values the last observation was carried forward. We also performed an analysis in patients who fully adhered to the treatment.
χ2 tests examined self-reported side-effects of the two groups. Schirmer I, ESR, and IgG (skewness >1.5) were logarithmically transformed before parametric analysis. The primary and secondary outcome measurements were evaluated with repeated measures analysis of variance. The quadratic time effect examined whether both the DHEA and placebo medication induced a change. The quadratic group × time interaction effect examined whether this change was different for patients on DHEA and placebo. The mean auto-correlation between the 5 assessment points varied from r = 0.56 for general fatigue to r = 0.76 for depressive mood. With an auto-correlation of r = 0.65 to achieve a moderate effect size of f = 0.25, analyses of variance (5 repeated measures, 2 groups with 30 participants each, 2-tailed α = 0.05) achieves a high power of β = 0.99 for both the time effect and the time × group interaction; the power to detect a small effect (f = 0.10) of β = 0.63 is below the β = 0.80 criterion.31
Ancillary analyses examined by repeated measures analyses of variance whether effects on primary outcomes were dependent on whether patients believed to have used DHEA or placebo and, within the patients who had used DHEA, whether effects were dependent on menopausal status, age, fibromyalgia, baseline DHEAS levels, the change of DHEAS in response to DHEA administration, and baseline levels of general fatigue, depressive mood, and mental well-being. In case of non-dichotomous variables, two subgroups were created by median split. The power of ancillary analyses in the group of 30 patients on DHEA is low (β = 0.33) for a small effect and high (β = 0.99) for a moderate effect.
Statistical analyses were performed using SPSS 11.5 for windows (SPSS, Chicago, Illinois). A two-sided p value <0.05 was considered statistically significant.
RESULTS
Patients
In all, 60 patients were randomly assigned to receive DHEA or placebo. Figure 1 is a flow chart of the research participants. Of 155 eligible patients, 95 declined participation because of fear of side-effects (44%), trial considered too much a burden (33%), travelling expenses (13%), absence of fatigue and distress (9%), and chance of being allocated to placebo medication (2%). Three patients in the DHEA group and one in the placebo group stopped the study medication prematurely.

Patient characteristics at enrolment were similar for both treatment groups (table 1).
DHEAS and testosterone levels
At baseline, mean serum DHEAS was 1.9 (SD 1.1) and 1.7 (SD 1.1) μmol/L for the DHEA and placebo groups, respectively. Mean serum testosterone was 0.9 (SD 0.4) nmol/L in both groups. During treatment with DHEA, mean levels of DHEAS and testosterone increased to supraphysiological values of 20.0 μmol/L and 4.3 nmol/L, respectively. DHEAS and testosterone values were within normal limits at baseline, after discontinuation of treatment, and during treatment with placebo.
We suspected that four patients did not take the DHEA study medication regularly. In these patients the change in DHEAS levels after 12 months of DHEA intake was between −0.4 and 2.6 µmol/L. This is in the range of changes observed in the placebo group (−1.60 to 3.20 µmol/L). In the other patients on DHEA, the increase in DHEAS levels varied from 4.9 to 48.7 µmol/L.
Side effects
Androgenic
An increase of acne and body hair was reported more often by patients on DHEA than those on placebo: 37, 47, and 43% of the patients on DHEA reported an increase of acne at the 3, 6, and 12 month assessments (10, 7, and 10% of the patients on placebo) and 20, 40, and 63% of the patients on DHEA reported an increase of body hair (0, 3, and 7% of the patients on placebo). The frequencies of menstrual abnormalities and oily skin or capital hair did not differ between the groups with increased oily skin or capital hair after 12 months (17% in DHEA and 0% in placebo) as the only exception. One patient of the DHEA group stopped study medication after 3 months because she feared increase of hirsutism.
Other
In the DHEA group one patient stopped participation after 7 days because she experienced restlessness, malaise, night sweats, and skin rash and another patient stopped after 6 months, because of increased ocular pain and dryness, restlessness, and sleep disturbance.
Two patients in the DHEA group had a severe deterioration in health during the study period. Both continued DHEA treatment and had all evaluations. One patient, known to have mitral valve insufficiency, developed heart failure 5 months after the start of DHEA treatment when she had a pulmonary infection. The second patient had progressive dyspnoea 12 months after the start of DHEA. A diagnosis of lymphocytic interstitial pneumonitis was made; she was treated with high dose glucocorticoids and 6-monthly intravenous infusions with cyclophosphamide.
Primary outcomes
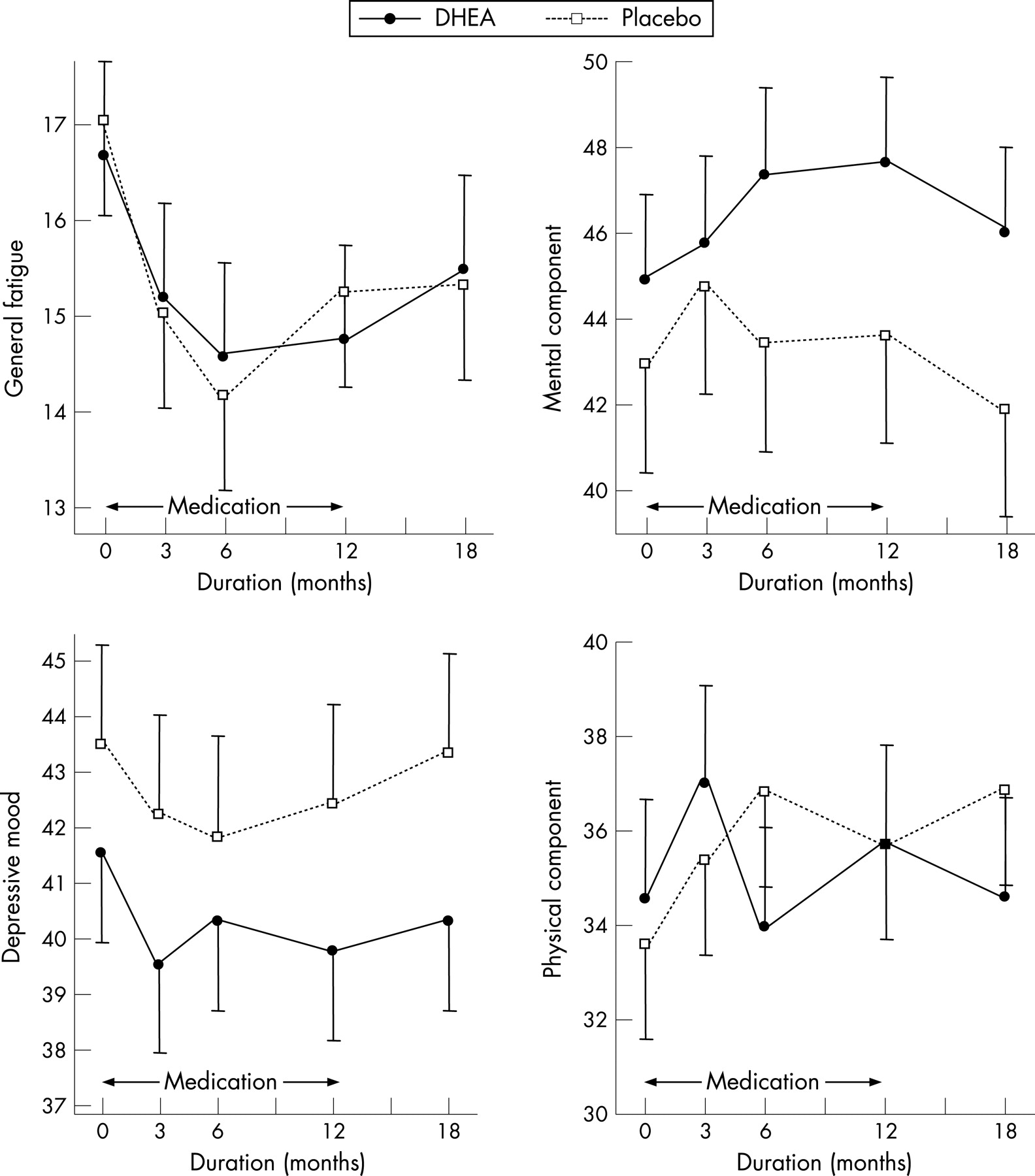
Figure 2 shows the change during the study period of the four primary outcome measures for the DHEA and the placebo group. General fatigue showed a significant change for both treatments (p<0.001): it decreased during the first 6 months of medication use and steadily increased after this period. There was no differential effect of medication: the change in fatigue did not differ for the DHEA and placebo group (p = 0.77). Also, the mental component score (p = 0.04) and depressive mood (p = 0.01) showed a significant change during the study for both medication groups; the best scores were observed during the treatment period. For the mental component score (p = 0.90) and depressive mood (p = 0.65) no significant differences were found between the change in the DHEA and in the placebo group. In both treatment groups no systematic change (p>0.33) was found for the physical component score.
Secondary outcomes
Of eight secondary outcome measures, a significant change for both groups was only detected for self-perceived oral dryness with least complaints during intake of study medication (p = 0.005, fig 3).

For three secondary outcome measures, ie self-perceived ocular dryness, ESR, and haemoglobin, the change was significantly different between the treatment groups (fig 3). Ocular dryness complaints became worse for patients on DHEA as compared to patients on placebo (p = 0.01). The ESR decreased with the use of DHEA and was stable with placebo (p = 0.03). Haemoglobin levels showed a different change for the DHEA and placebo group (p = 0.04), but these changes did not reflect an improvement during the medication intake for either group.
Ancillary analyses
We examined whether the change of general fatigue, mental well-being, and depressive mood was related to the patient’s belief to have used DHEA or placebo, menopausal status, age, presence of fibromyalgia, baseline DHEAS serum level, the change in DHEAS level in response to DHEA administration, perceived side effects, and baseline levels of the primary outcome measures.
Of the 30 patients with DHEA, 19 believed to have used DHEA, 9 placebo, and 2 did not know. Of the 30 patients with placebo, 21 believed to have used placebo, 7 DHEA, and 2 did not know. Excluding the 4 patients who did not know, we analysed the change of general fatigue, mental well-being, and depressive mood in relation to actual and believed medication used (fig 4). The change of general fatigue (p = 0.15), the mental component score (p = 0.43), and depressive mood (p = 0.22) did not differ as a function of actual medication use, whereas the change of general fatigue (p<0.001), and depressive mood (p = 0.02), but not the mental component score (p = 0.13), were significantly different as a function of believed medication use: the patients who believed to have used DHEA demonstrated an improvement on fatigue and depressive mood.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
In the DHEA-treated group, the change of general fatigue, mental well-being, and depressive mood did not depend on menopausal status (p>0.26), age (p>0.31), fibromyalgia (p>0.51), extent of change in serum DHEAS levels during treatment (p>0.07), or perceived side effects (p>0.62). Patients with higher baseline serum levels of DHEAS improved more on general fatigue than patients with lower levels (p = 0.03), while changes in depressive mood and the mental component score (p>0.66) were not dependent on baseline DHEAS. The change in general fatigue, depressive mood, and the mental component score did not depend on baseline levels of these three variables with one exception: the decrease of depressive mood from baseline to the first assessment after 3 months was higher for the group with more depressive mood (p = 0.04).
Adherers-only analyses
Results of analyses with exclusion of 4 patients with missing values and 4 patients with extraordinarily small changes in serum DHEAS levels, did not differ from the intention-to-treat analyses.
DISCUSSION
Our placebo controlled double-blind study in women with pSS demonstrates a beneficial effect on fatigue and well-being with both DHEA and placebo treatment and disproves a beneficial effect of DHEA over placebo.
These results apply to a pharmacological DHEA dose of 200 mg per day, which has been used and shown safe in inflammatory diseases.16 19 20 32 A substitution dose of 50 mg DHEA might be sufficient to affect mood, while a higher dose also affects disease activity.33 Our study showed that administration of DHEA-induced physiological effects: serum DHEAS and testosterone raised to supraphysiological levels, androgenic side effects were reported, and a decrease of ESR was measured.
The suggestion of a positive effect of DHEA administration on physical and psychological parameters comes from some,9–11 but not all34–36 studies in elderly healthy participants and studies in a variety of disease states.12–18 Several of these studies had a small sample size,13–15 18 lacked a placebo controlled design,11 15 18 or did not analyse according to intention to treat.16 17 A sound demonstration of a positive effect of DHEA replacement on well-being was given in women with subnormal DHEA serum levels caused by adrenal insufficiency.14
One can argue that we could not prove an effect of DHEA administration, because our patients were not DHEAS deficient, were not on glucocorticoid therapy which decreases serum DHEA(S) levels,37 38 and also because premenopausal women were included, while supplementation is more plausible after the menopause. The sample size of the ancillary analyses in our study was too small to detect small effects, and thus prohibits the generalisation of results to DHEA-deficient groups, groups on glucocorticoid therapy, or postmenopausal women. Our analyses did not, however, find a differential effect of DHEA of moderate magnitude in these subgroups.
Our primary aim was not to examine whether DHEA would affect disease activity in women with pSS, but we included ESR, haemoglobin concentration, and serum-IgG in our study as surrogate disease activity parameters. Studies in SLE19 20 and in a mouse model of Sjögren syndrome24 reported less disease activity with administration of androgens. In contrast with a previous study in pSS,39 in our study as in female patients with pSS treated with nandrolone decanoate,40 ESR decreased with DHEA compared to placebo.
Our study suggested favourable outcomes for both DHEA and placebo. Ancillary analyses demonstrated that fatigue and mood varied as a function of believed medication use instead of actual medication use. Two mechanisms may explain this observation: either the belief they had DHEA-induced improvement, or improvement induced the belief they had DHEA. The suggestion that a placebo effect, instead of regression to the mean, explains the improvement of fatigue and well-being is strengthened by the observation that the extent of improvement of general fatigue and the mental component score did not depend on baseline levels. Definite proof of a placebo effect warrants a study that also includes a waiting list control group.
Biological and psychological factors contribute to fatigue, inactivity, and depressed mood. Although these symptoms are reflex-like responses to the inflammatory process, it is, to a certain extent, possible to not give in to them depending on motivation.41 The willingness of the patients to participate in our intervention demonstrates their positive expectation and motivation, which may have increased their vitality and well-being.
Our study does not support efficacy of 200 mg oral DHEA over placebo. Both oral administration of DHEA and placebo improved fatigue and well-being in patients with pSS. We did not examine the mechanisms underlying this unexpected placebo effect, but its presence suggests that it is possible to ameliorate fatigue and well-being in some women with pSS through non-pharmacological mechanisms. This may indicate possibilities for cognitive behavioural interventions.
Acknowledgments
We thank Kim Jacobs for laboratory analyses
REFERENCES
Footnotes
-
Funding: This study was financially supported by the Dutch Arthritis Association (NR 98-2-301). The study sponsor was not involved in study design, in the collection, analysis, and interpretation of data, in the writing of the report and in the decision to submit the paper for publication.
-
Competing interests: None declared