Article Text

Abstract
Tumour necrosis factor (TNF)-blocker tapering has been proposed for patients with rheumatoid arthritis (RA) in remission.
Objective The trial aims to compare the effect of progressive spacing of TNF-blocker injections (S-arm) to their maintenance (M-arm) for established patients with RA in remission.
Methods The study was an 18-month equivalence trial which included patients receiving etanercept or adalimumab at stable dose for ≥1 year, patients in remission on 28-joint Disease Activity Score (DAS28) for ≥6 months and patients with stable joint damage. Patients were randomised into two arms: maintenance or injections spacing by 50% every 3 months up to complete stop. Spacing was reversed to the previous interval in case of relapse, and eventually reattempted after remission was reachieved. The primary outcome was the standardised difference of DAS28 slopes, based on a linear mixed-effects model (equivalence interval set at ±30%).
Results 64 and 73 patients were included in the S-arm and M-arm, respectively, which was less than planned. In the S-arm, TNF blockers were stopped for 39.1%, only tapered for 35.9% and maintained full dose for 20.3%. The equivalence was not demonstrated with a standardised difference of 19% (95% CI −5% to 46%). Relapse was more common in the S-arm (76.6% vs 46.5%, p=0.0004). However, there was no difference in structural damage progression.
Conclusions Tapering was not equivalent to maintenance strategy, resulting in more relapses without impacting structural damage progression. Further studies are needed to identify patients who could benefit from such a strategy associated with substantial cost savings.
Trial registration number: ClinicalTrials.gov: NCT00780793; EudraCT identifier: 2007-004483-41.
- Rheumatoid Arthritis
- Anti-TNF
- Treatment
Statistics from Altmetric.com
Introduction
Remission is the widely accepted objective for patients with rheumatoid arthritis (RA) thanks to an early, dynamic, step-up therapeutic strategy based on conventional synthetic and/or biological disease-modifying anti-rheumatic drugs (csDMARDs and bDMARDs, respectively).1–4 Once this objective is achieved, treatment down-titration should be attempted, for patient preference, safety issues5–11—potentially dose-dependent8 ,12—or economic reasons.13
The feasibility of discontinuing biological agents used as induction treatment in early RA is a different question.14–18 The most frequently tested step-down strategy in established RA is a complete discontinuation of bDMARDs in patients with stable clinical remission (ie, lasting >6 months).19–24 Whatever the biological agent considered, most patients do not stably remain in drug-free remission, although discontinuation may be proposed to patients with RA in remission. The risk of relapse was found substantial in the year after treatment discontinuation, with increased risk of joint damage when assessed.
Dose reduction could be relevant; some authors have suggested that the dose of biologics given in clinical practice may be unnecessarily high.25 ,26 A first observational study assessed progressive down-titration of infliximab over 1 year.22 Down-titration was feasible for 45% of patients, with a mean dose reduction of 60% (mean dose 224 mg at baseline to 130 mg after 1 year). Discontinuation of infliximab was possible for 16% of patients. The second study was a randomised controlled trial of patients with RA achieving remission after 1-year treatment with etanercept (ETA) and compared three strategies: full-dose maintenance, half-dose reduction and complete one-step discontinuation.24 Dose reduction was associated with a non-significant risk of relapse and structural damage progression at 1 year as compared with full-dose maintenance. Reduction in number of injections could be preferred by patients to reduced dosing of each injection.
Here, we report the results of a multicentre randomised controlled trial whose primary objective was to demonstrate the equivalence of a down-titration strategy of progressively spacing injections of biologics, namely tumour necrosis factor (TNF) blockers, relative to the usual regimen, maintaining therapy at full dose, in terms of disease activity.
Patients and methods
Study design
The STRASS—Spacing of TNF-blocker injections in Rheumatoid ArthritiS Study—was a multicentre 18-month equivalence randomised controlled trial following the Prospective Randomized Open Blinded End-point (PROBE) methodology.27 It compared two therapeutic strategies in patients with established RA who achieved clinical remission with subcutaneous injection of the TNF blocker ETA or adalimumab (ADA) in 22 rheumatology departments in France and one department in Monaco. The study aimed to demonstrate the equivalence of down-titrating ETA or ADA by progressively spacing injections (S-arm) and maintaining full-regimen therapy (M-arm) in terms of disease activity.
Patients were randomly assigned in a 1:1 ratio to one of the two strategies. The randomisation list was generated by use of a computer-generated sequence with blocks of variable (2–6) and undisclosed size stratified by centre and TNF-blocker (ie, ETA or ADA). Treatment allocation was concealed to patients, research staff and clinical staff until randomisation by use of an internet-based randomisation module (Cleanweb, Telemedecine technologies S.A.S, Boulogne-Billancourt, France). Patients and clinical staff could not be further masked to treatment allocation because a sham intervention was not feasible (sham of spacing injections); however, patients were unaware of the study hypothesis, and clinical staff were unaware of aggregate outcomes during the study. The outcome assessor for 28-joint Disease Activity Score (DAS28) (primary outcome) and X-ray readers were masked to treatment allocation.
The study and all related documents were approved for all centres by an ethics review board (CPP Ile de France VI; IRB authorisation no. 100-07); the study was conducted in accordance with the Declaration of Helsinki and Good Clinical Practices. A standardised information sheet was given to eligible patients to explain that different therapeutic strategies have been proposed to patients with RA in remission but without formal evaluation so far, which necessitated the conduct of trials such as STRASS. Written informed consent was obtained from all patients before their participation in the trial.
Patients
From September 2008 to January 2011, we included patients who were ≥18 years old, had a diagnosis of RA according to the 1987 American College of Rheumatology classification criteria28 and received subcutaneous injections of ETA or ADA at a standard and stable dosage (ie, 50 mg weekly for ETA or 40 mg every other week for ADA) for at least 1 year as monotherapy or combined with a stable csDMARD (methotrexate or leflunomide) for at least 6 months. Prednisone was allowed if daily doses were stable and at ≤5 mg for at least 6 months. Patients needed to be in clinical remission according to the DAS2829 (ie, DAS28≤2.6) for at least 6 months with no structural damage progression seen on hand and foot X-rays in the year before inclusion according to the treating rheumatologist.
Non-inclusion criteria were contraindications to TNF-blocker therapy maintenance, prednisone use >5 mg/day, planned surgical intervention or pregnancy within the 18-month study period, women of childbearing age without efficacious contraception, history of cancer, diagnosis of an auto-immune disorder other than RA, non-affiliation with the French social security system and presence of factors preventing informed consent or protocol adherence (eg, inability to communicate in the French language, mental incapacity, guardianship).
Finally, all included patients underwent clinical examination, were able to understand the French language and protocol requirements and gave their signed informed consent to be in the trial.
Intervention
Patients receiving csDMARDs and prednisone (≤5 g/day) along with a TNF blocker were allowed to continue these therapies at a strictly stable dose throughout the study period.
In the M-arm, patients continued to receive TNF-blocker subcutaneous injections at the standard full regimen.
In the S-arm, the strategy relied on an algorithm (see online supplementary appendix) that progressively spaced out subcutaneous injections according to DAS28 assessment; all other treatments remained at a stable dose throughout the trial. Injection spacing was based on augmenting by approximately 50% every 3 months the interval between two injections according to five steps (step 0 corresponding to the full-dose regimen): ETA 50 mg every 10 days (step 1), 14 days (step 2), 3 weeks (step 3) or stopped (step 4); ADA 40 mg every 21 days (step 1), 28 days (step 2), 6 weeks (step 3) or stopped (step 4). The rule used to define the next step depending on the DAS28 was as follows: with DAS28≤2.6 at the next 3-month follow-up visit, the treatment progressed to the next step interval for the next 3-month period; with DAS28 score >2.6 and an increase of ≤0.6 in score since the last visit, the treatment remained at the current step; and with DAS28>2.6 and an increase of >0.6 in score, the treatment reverted to the interval of the previous step. A second attempt could be proposed after remission re-achievement.
In case of RA relapse among M-arm patients or S-arm step-0 (full-regimen) patients, changes in therapy were at the discretion of the rheumatologist, but patient follow-up continued to the end of the study.
Endpoints
The primary endpoint was the evolution in RA inflammatory activity over 18 months as measured by the DAS28 every 3 months. Disease activity was assessed by the DAS28 in each centre by a rheumatologist who was unaware of the study arm of the patient (local investigators and patients were told not to give the assessor any information related to the treatment strategy allocated). Secondary clinical endpoints were evolution of RA inflammatory activity during the 18 months as measured by the DAS4430 every 3 months, relapse during the 18 months defined as DAS28>2.6 with DAS28 increase >0.631 since the previous study visit and evolution of functional ability over 18 months as measured by the Health Assessment Questionnaire (HAQ) score.32 In addition, structural damage progression seen on X-rays between baseline and 18 months was assessed by the modified-van der Heijde Sharp score (vSHS).33 This score relied on hand and foot X-rays and was assessed by two independent readers (FG and VF; interobserver reproducibility estimated by interclass coefficient 0.97; smallest detectable change 4.5 points) who were blinded to the patient's treatment arm and clinical outcomes.
The safety of the two strategies was assessed and reported in terms of rate of non-serious and serious adverse events (AEs). Finally, predictors of relapse were explored.
Data collection
Comprehensive sociodemographic and disease characteristics as well as clinical and biological parameters were collected at the time of inclusion. During follow-up, visits were scheduled every 3 months for 18 months. RA clinical and biological parameters and medication use were collected at each visit. Radiography of hands and feet was performed at baseline and 18 months.
Statistical analysis
This trial was designed to detect equivalence of the slope of DAS28 from baseline to 18-month follow-up between the two arms. Primary analysis compared the standardised difference between the slopes (ie, the difference of the slopes divided by the SD of this difference). The equivalence margin for the standardised difference was fixed at ±30%.34 With α=5%, the number of repeated DAS28 measures for each patient during the study7 and the correlation between DAS28 measures (0.5), we needed 250 patients (125 in each arm) to establish equivalence with a power of 80%.
The principal analysis involved a linear mixed-effects model to account for correlations between repeated measurements in the same individual. First, we fitted a linear mixed-effects model including trial arm, time, and interaction between trial arm and time as fixed-effect covariates, a random intercept and slope across individuals. In this model, the coefficient associated with the interaction term represents the difference between the slopes of DAS28 score. We used this coefficient and its SD to estimate the standardised difference of interest and used bootstrapping (1000 replications) to estimate the 95% CI.35 The trial arms were considered statistically equivalent if the 95% CI of the standardised difference was within the prespecified equivalence margins (+30% to −30%). Considering the same assumptions as used for sample size estimation and an SD of DAS28 set at 1,36 the equivalence margins could be interpreted as a maximum difference in mean DAS28 between arms of ±0.34 at 18 months. As recommended, the primary analysis was per protocol, supplemented by an intent-to-treat analysis. The per-protocol population included patients who completed the study without major deviations regarding the strategy of the trial arm. A major deviation was defined as a change in therapeutic strategy able to modify the probability of maintaining remission or relapsing, such as modification of ongoing csDMARDs or a return to the full regimen in the M-arm even though relapse occurred at step 2 or higher. A sensitivity analysis involved a more strict definition of the per-protocol population (ie, patients with no deviations from the protocol, major or not). Subgroup analyses were performed by molecule at baseline and mode of prescription at baseline. Equivalence between trial arms in terms of DAS44 and HAQ score was analysed in the same way.
To assess whether the spacing strategy induced relapse, relapse rate was compared between treatment arms by univariate Cox proportional-hazards models. Survival curves were constructed by the Kaplan–Meier method. The predictors of relapse were explored by univariate Cox models. Potential predictors were DAS28 score, HAQ score, rheumatoid factor (RF), anticitrullinated peptide antibodies (ACPA), C-reactive protein, treatment group, morning stiffness duration, pain intensity, patient global assessment, vSHS and smoking status. All potential confounding factors were entered into a multivariable Cox model.
The DAS28 at relapse for patients who experienced relapse was compared between trial arms by the Wilcoxon test. Structural damage progression seen on X-rays—vSHS variation >1 point (smallest detectable difference, SDD)—and the number of serious and non-serious AEs were compared between trial arms by Wilcoxon tests. All statistical analysis involved use of SAS V.9.2 (SAS Inst., Cary, North Carolina, USA).
Results
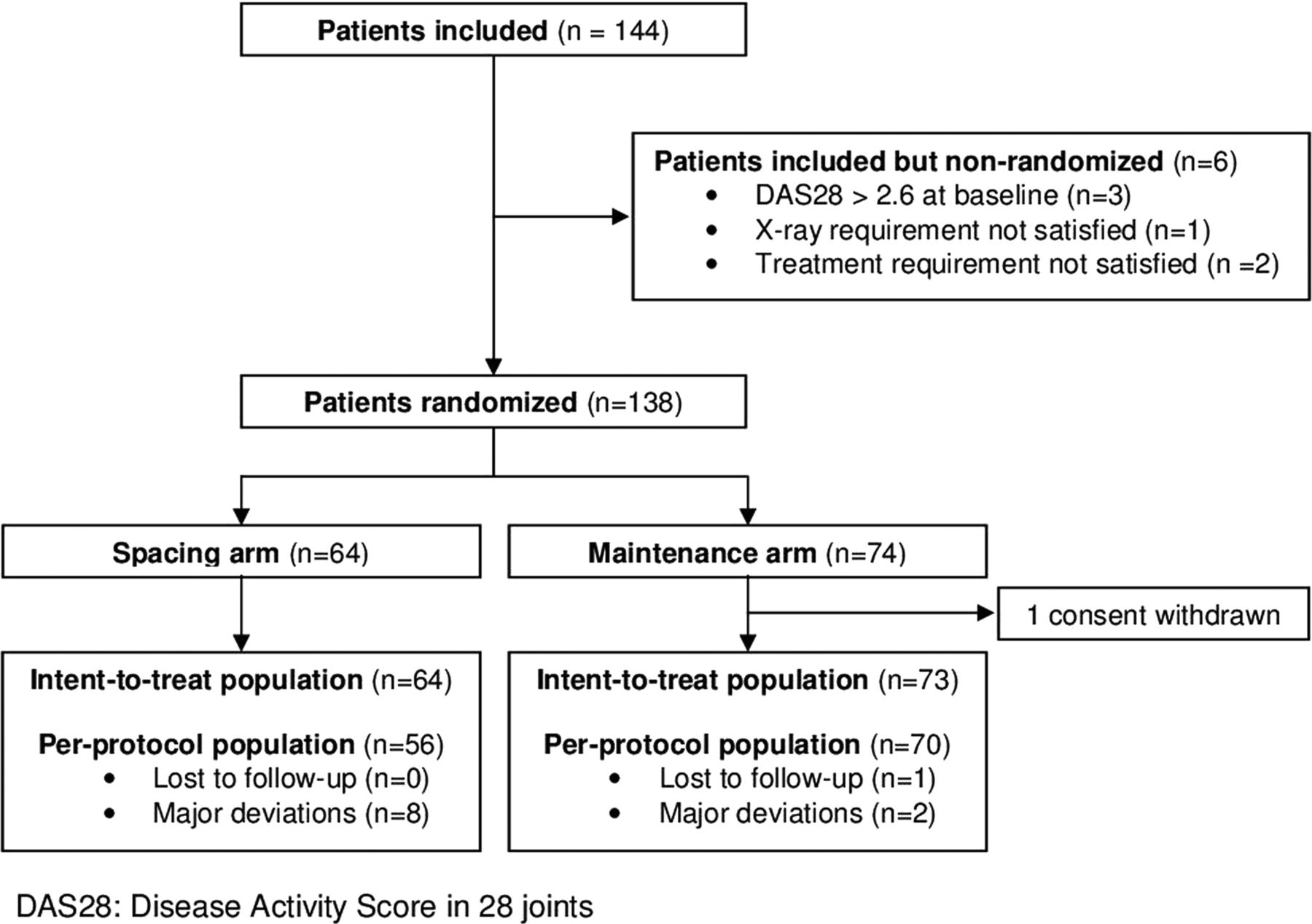
The enrolment rate was lower than expected, and inclusions were stopped prematurely, when 144 patients had been recruited, because of lack of funding. Enrolment difficulties were mainly due to patients with RA in remission being essentially cared for in community rheumatology practices and less prone to visit a university hospital. Among the included patients, 138 patients were randomised, 64 to the S-arm and 74 to the M-arm (figure 1). Among 73 patients for analysis in the M-arm, one patient withdrew consent. The main baseline characteristics of patients are in table 1. In all, 63 received ADA and 74 ETA, with 104 receiving both a TNF blocker and a csDMARD and 33 TNF-blocker monotherapy.
Patient characteristics at baseline

Flow-chart of the patients enrolled in the STRASS (Spacing of TNF-blocker injections in Rheumatoid ArthritiS Study).
The per-protocol population for the primary analysis involved 56 patients in the S-arm and 71 in the M-arm. One patient from the M-arm was lost to follow-up. A total of 10 patients (7.3%), 8 in the S-arm and 2 in the M-arm, had major protocol deviations, and 23 patients (16.8%), 18 in the S-arm and 5 in the M-arm, had minor protocol deviations. At the last visit, six and seven patients in the S-arm and M-arm, respectively, stopped receiving treatment by the treatment algorithm because of loss of efficacy.
In the S-arm, 13 patients (20.3%) returned to the initial step and were not able to space TNF-blocker injections. In all, 48 (75.0%) were able to space injections: 25 patients (39.1%) could completely stop TNF-blocker injections (step 4) and 10 (15.6%) could taper TNF blockers up to step 3, 7 (10.9%) to step 2 and 6 (9.4%) to step 1.
Clinical endpoints
The evolution of the mean DAS28 in each trial arm over time is in figure 2. The equivalence of the M-arm and S-arm strategies was not demonstrated in terms of disease activity measured by the DAS28 during follow-up (standardised difference 19% (95% CI −5% to 46%), outside of the interval). We obtained similar results for disease activity measured by the DAS44 during follow-up (standardised difference 12% (95% CI −12% to 39%)) and functional status during follow-up (standardised difference 25% (95% CI −0.3% to 50%)). Results were similar in the second per-protocol and intent-to-treat population (see online supplementary table A). Subgroup analyses of disease activity by TNF-blocking agent and mode of prescription showed similar results for patients receiving ETA or ADA and patients receiving TNF blockers combined with a csDMARD (methotrexate or leflunomide) or as monotherapy. Evolution of the mean DAS28 in each trial arm in these subgroups over time is in figure 3. In addition, a superiority analysis was conducted and did not reveal any significant difference (see online supplementary figure A).

Evolution of disease activity during the 18-month follow-up in the whole population. DAS, Disease Activity Score.
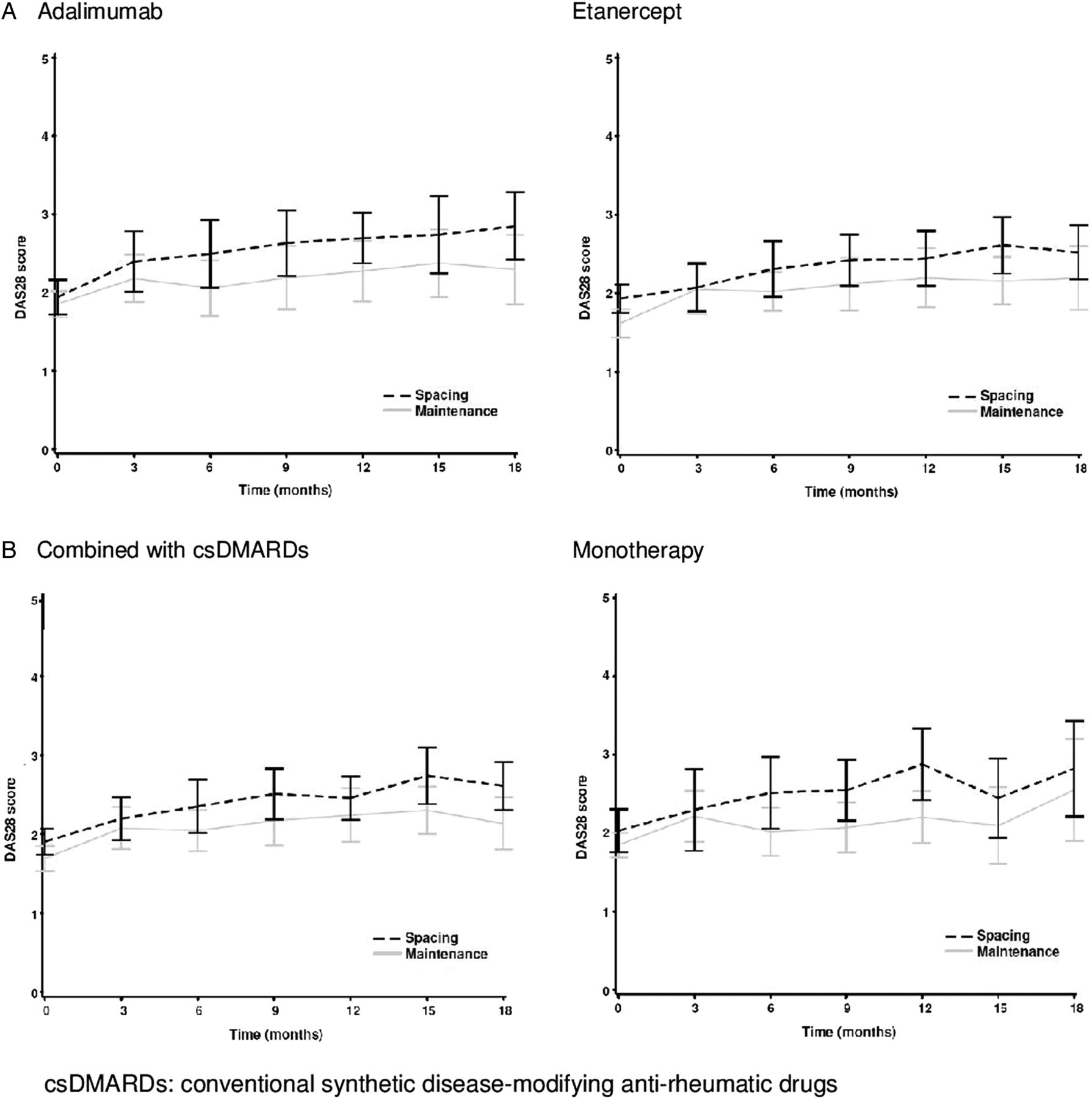
Evolution of disease activity during the 18-month follow-up in the whole population (mean Disease Activity Score (DAS) with 95% CI in spacing and maintenance arms at each visit), stratified by drug (A) and mode of prescription (B).
Cumulative incidence curves of RA relapse are in figure 4. The risk of relapse was significantly higher in the S-arm than in the M-arm (HR 2.37 (95% CI 1.47 to 3.83); p=0.0004). Altogether, 49 patients (76.6%) of the S-arm showed relapse: 18 at step 0, 7 at step 1, 7 at step 2, 14 at step 3 and 1 at step 4 (discontinuation of TNF blockers). In the M-arm, only 34 patients (46.5%) showed relapse. The median time to relapse was 9 versus 18 months in the S-arm versus M-arm. The median (IQR) DAS28 at relapse was 3.5 (3.0–4.0) in the S-arm and 3.1 (2.9–3.7) in the M-arm (p=0.12).

Relapse occurrence by strategy arm (Kaplan–Meier cumulative incidence curves by trial arm).
Baseline characteristics of patients associated with the occurrence of relapse are indicated in online supplementary table B. Factors significantly associated with relapse in the Cox model were the spacing strategy (HR 2.74 (95% CI 1.53 to 4.92), baseline HAQ score (HR 2.07 (1.23 to 3.49) and immunoglobulin M RF positivity (HR 1.99 (1.03 to 3.83), after adjustment for all potential confounding factors (DAS28, HAQ, RF and ACPA status, C-reactive protein, treatment arm, morning stiffness duration, pain intensity, patient global assessment, vSHS and smoking status).
Finally, the impact of the spacing strategy on HAQ was comparable with what was observed on DAS28 (see online supplementary figure B and table A).
Relapses were managed by TNF-blocker re-escalation in the S-arm: among the 49 patients with relapse, 20 (40.8%) achieved remission again, 19 (38.8%) had low disease activity and 4 (8.2%) had moderate disease activity (considered acceptable, therefore continuing the ongoing biologic). In the M-arm, relapses were managed with only symptomatic treatments: among the 34 patients, 17 (50.0%) achieved remission again, 4 (11.8%) had low disease activity and 6 (17.6%) had moderate disease activity. Four and six S-arm and M-arm patients with relapse, respectively, lost a therapeutic response (ie, were unable to reach an acceptable state—remission, low disease activity or moderate disease activity—with the same DMARD). A second tapering was attempted in eight patients, with a new relapse in four.
Radiological endpoints
The median (IQR) vSHS change was 0.0 (0.0–1.5) and 0.0 (0.0–1.5) for M-arm and S-arm, respectively (p=0.7) (figure 5). The proportion of patients without structural damage progression was 69% and 66% in the M-arm and S-arm, respectively, with the SDD-based threshold (p=0.8).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cumulative progression of structural damage seen on X-rays measured by variation in 18-month van der Heijde-modified total Sharp score (vSHS) from baseline (mean of the two readings).
Safety
Two hundred and fifty-nine non-serious AEs were reported in 97 (71%) patients, that is, 69 and 73 AEs in 51 (70%) and 46 (72%) patients of the M-arm and S-arm, respectively. The median number of non-serious AEs of 1.0 in both groups (p=0.7), the most frequently reported being mild infections. Thirty serious AEs were reported in 16 patients, that is, 14 and 16 AEs in 10 (14%) and 6 (9%) patients of the M-arm and S-arm respectively. The median (IQR) number of serious AEs was 0.0 (0.0–0.0) and 0.0 (0.0–0.0) in the M-arm and S-arm, respectively (p=0.4), with 6 (5%) and 2 (3%) having reported two or more serious AEs. One serious event—urological tract infection—was observed in the M-arm, and optical neuritis suggestive of demyelinising disease was observed in a patient receiving ADA in the S-arm (see online supplementary table C).
Discussion
The present study is the first trial implementing the concept of ‘progressive achievement of the lowest efficacious dose’ in terms of a step-down strategy of injection spacing for patients with established RA who achieved stable remission while receiving subcutaneous injection of TNF blockers. The null hypothesis of non-inferiority could not be disproven due to insufficient recruitment. However, we found that such a step-down strategy is feasible but exposes patients to risk of relapse, which was controllable in most patients by reverting to the previous step (only two patients (3.1%) lost the therapeutic response and had to switch to another DMARD).
Several studies have tested the feasibility and risks of TNF-blocker reduction or interruption in established RA. Most studies were observational—some were long-term trial extension studies—and proposed complete, abrupt interruption of biological agents, either TNF blockers or other mode-of-action drugs such as abatacept or tocilizumab.20 ,21 ,23 ,37–42 The sample sizes ranged from 21 to 197 patients and included patients with RA in stable remission or low disease activity, for at least 6 months. Rates of sustained remission at 1 year despite biological agent interruption ranged from 13% to 49%. The main conclusion was that less than one patient in two would show sustained remission or low disease activity after biological cessation, with no relevant association between the risk of relapse and disease activity at biological cessation. Therefore, several authors proposed not to stop the treatment but rather to reduce the dose. The feasibility of such a strategy was first demonstrated in an observational cohort of patients with RA in remission who were receiving infliximab, for whom a systematic dose reduction by 25%–100% was proposed.22 Only a small subset of patients was able to completely stop infliximab; most were able to continue with lower doses. Since then, two randomised controlled trials of ETA, which is available in two dosages, demonstrated the absence of significant difference between half and full dose of ETA to maintain low disease activity.24 ,43
The injection spacing significantly increased the risk of relapse in our study, which was not observed with reduced doses of ETA in the two previous trials.24 ,43 The discrepancy was partly expected because our tapering strategy aimed to go as low as possible in terms of treatment reduction; flare occurrence was part of the design and helped identify the lowest efficacious dose (ie, the reduced dose just above the dose at which the relapse has occurred). Since spacing was reversed in case of relapse, no significant joint damage progression or complete loss of efficacy was observed. In another recent spacing strategy trial, flares occurred in 55% of the patients versus 20% in the M-arm.44 The spacing strategy was found non-inferior to the maintenance strategy in terms of persistent flare, due to the addition of steroid injections to restart of full-dose TNF blockers. However, the structural damage progression was significantly higher in the S-arm.
This study has some limitations. The sample size needed for sufficient power was 250 patients, but only 137 were enrolled, so the trial was underpowered. Enrolment difficulties were mainly due to the fact that patients with stabilised disease are cared for in private community rheumatology practice and prefer to stay away from the hospital. Other explanations could be (i) the unwillingness of physicians and/or patients to taper medications that have been effective with a risk of flaring and perhaps not recapturing benefit and (ii) the inclusion of patients in remission rather than low disease activity. Because of its design, the trial protocol could not blind patients and care providers to treatment allocation. Thus, we used a PROBE design, in which participating patients were kept unaware of the hypothesis of the trial; such a methodology has been found comparable with double-blinded controlled trials in terms of risk of measurement bias.27 Also, some deviations from the algorithm were observed, most being minor. Because of the different sensitivity analyses performed, these deviations did not bias the study results. Finally, an important question was not addressed by the study: could the tapering strategy have an impact on anti-drug antibody production, and thus increase the risk of secondary failure. The biological material was not available in the STRASS trial; however, such phenomenon has never been reported so far.
Our trial also has several strengths. It was an institutionally-sponsored multicentre randomised controlled trial which included patients with RA receiving two TNF-blocking agents by the same route of administration—a soluble receptor, ETA, and a monoclonal antibody, ADA. Moreover, we used a pragmatic design based on a reduced number of injections by progressively spacing the interval between subcutaneous injections rather than reducing the dose per injection. This strategy fits with patient expectations. One of the advantages of such a spacing strategy is the lack of dependence on the availability of a reduced dose of the compound. Injection spacing has been studied for ankylosing spondylitis and Crohn's disease.45–47 Although debated from a strict pharmacokinetics viewpoint (not respecting the drug half-life, fluctuating serum drug levels), such strategies were associated with a mild increase in disease activity but remained acceptable by physicians and patients. In our trial, a step-up strategy was reinitiated with disease relapsed, which reduced the risk of structural damage progression.
Conclusion
The null hypothesis of non-inferiority of the spacing strategy could not be disproven due to insufficient recruitment. Moreover, relapses occurred with bDMARD tapering. However, these patients were rapidly recaptured with bDMARD re-escalation to scheme. More than one quarter of patients did not flare with the tapering strategy warranting further study to identify patients with RA who could benefit from such a strategy.
Acknowledgments
The authors thank all patients who participated in the trial and the investigators of the inclusion centres: Dr S. Pavy (Bicêtre Hospital, Paris); Professor P. Dieudé (Bichat Hospital, Paris); Dr M. N'Guyen and Professor M. Dougados (Cochin Hospital, Paris); Professor F. Lioté and O. Peyr (Lariboisière Hospital, Paris); Drs A. Economou, C. Fevre and Professor X. Chevalier (Créteil); Dr V. Foltz and Dr B. Banneville (Pitié Hospital, Paris); Dr J. Sellam and Professor F. Berenbaum (St Antoine Hospital, Paris); Dr M. De Bandt (Aulnay); Dr J-CB (Belfort); Professor T. Schaeverbeke (Bordeaux); Dr S. Jousse-Joulin, Professors A. Saraux and V. Devauchelle-Pensec (Brest); Dr D. Poujol and Professor M. Soubrier (Clermont-Ferrand); Professor J-F. Maillefert (Dijon); Dr M. Gilson (Grenoble); Drs L. Artru and X. Puéchal (Le Mans); Professor R-M. Flipo (Lille); Dr M. Luc and Professor P. Lafforgue (Marseille); Drs C. Lukas and Dr G. Mouterde, Professor B. Combe (Montpellier), Dr Y. Maugars (Nantes); Dr I. Azaïs and Professor F. Debiais (Poitiers); Dr J-D. Albert, Professors A. Perdriger and G. Chalès (Rennes); Professors P. Goupille and D. Mullemann, Dr E. Ducourau (Tours); Dr O. Brocq (Monaco).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
- Data supplement 2 - Online appendix
Footnotes
Handling editor Tore K Kvien
XM and FT have provided similar contribution to this work and should be considered as co-last authors.
Contributors BF, TP, JM, XM and FT conceived the project. BF and FT organised the study. BF, TP, TA, JM, XM and FT wrote the paper. TA conducted the statistical analyses. FG and VF performed the X-ray reading. All authors participated in the project construction and realisation, as well as the discussion ad interpretation of results.
Funding The trial was conducted under the auspices of the CRI-IMIDIATE clinical research FCRIN network. Institutional support by a grant from the Ministry of Health (PHRC national 2007, AOM 07 127/P 070120), France. The sponsor was the Département à la Recherche Clinique et au Développement, Assistance Publique–Hôpitaux de Paris.
Competing interests None declared.
Patient consent Obtained.
Ethics approval CPP Paris 6.
Provenance and peer review Not commissioned; externally peer reviewed.