Article Text

Abstract
Objective: To determine protein and activity levels of matrix metalloproteinases 1 and 3 (MMP-1 and MMP-3) in synovial fluid of patients with knee joint injury, primary osteoarthritis, and acute pyrophosphate arthritis (pseudogout).
Methods: Measurements were done on knee synovial fluid obtained in a cross sectional study of cases of injury (n = 283), osteoarthritis (n = 105), and pseudogout (n = 65), and in healthy controls (n = 35). Activity of MMP-1 and MMP-3 in α2 macroglobulin complexes was measured using specific low molecular weight fluorogenic substrates. ProMMP-1, proMMP-3, and TIMP-1 (tissue inhibitor of metalloproteinase 1) were quantified by immunoassay.
Results: Mean levels of proMMP-1, proMMP-3, and TIMP-1 were increased in injury, osteoarthritis, and pseudogout compared with controls. MMP-1 activity was increased in pseudogout and injury groups over control levels, whereas MMP-3 activity was increased only in the pseudogout group. The increase in MMP-1 activity coincided with a decrease in TIMP-1 levels in the injury group.
Conclusions: Patients with joint injury have a persistent increase in proMMP-1 and proMMP-3 in synovial fluid and an increase in activated MMPs, which are not inhibited by TIMP. The differences in activation and inhibition patterns between the study groups are consistent with disease specific patterns of MMP activation and/or inhibition in joint pathology.
- α2M, α2 macroglobulin
- MMP, matrix metalloproteinase
- proMMP, pro-matrix metalloproteinase
- TIMP, tissue inhibitor of metalloproteinases
- matrix metalloproteinases
- arthritis
- joint injury
- synovial fluid
Statistics from Altmetric.com
- α2M, α2 macroglobulin
- MMP, matrix metalloproteinase
- proMMP, pro-matrix metalloproteinase
- TIMP, tissue inhibitor of metalloproteinases
Osteoarthritis is a slowly progressive joint disorder which usually occurs late in life and principally affects the hands and the large weight bearing joints.1 Joint trauma is one of several known predisposing factors for the development of osteoarthritis.2–8 In animal models of osteoarthritis, the development of macroscopic and radiological changes in the joint is preceded by early change in cartilage metabolism.9 Previous cross sectional marker studies on patients with knee injuries showed that synovial fluid contains increased levels of aggrecan fragments and cartilage oligomeric matrix protein (markers of matrix metabolism) immediately after the initial joint trauma,10,11 indicating increased degradation of joint tissue.12,13 Moreover, high levels of matrix metalloproteinases (MMPs) were present in synovial fluid of injury patients.11,14,15
MMPs are a group of Zn2+ dependent extracellular enzymes that play a key role in normal and pathological tissue remodelling16–19 and have the combined ability to degrade all components of the extracellular matrix.18 Based on domain structure and substrate specificity, MMPs can be divided into subclasses (collagenases, gelatinases, stromelysins, and membrane type MMPs).16,17 MMP-3 (stromelysin 1) plays an important role in the MMP cascade owing to its ability to degrade various components of cartilage such as gelatin, aggrecan, and collagen types III, IV, IX, and X, as well as to activate proMMPs 1, 7, 8, 9, and 13.16,17 Collagenases (MMP-1, MMP-8, and MMP-13) are capable of degrading intact collagen type II, one of the main components of the articular cartilage, into characteristic ¼ and ¾ fragments, which can be further degraded by gelatinases.16,17
Increased MMP production in joint pathology has been demonstrated by high levels of mRNA at tissue level20 and by increased amounts of proMMPs in synovial fluid.11,14,15,21–28 Moreover, previous studies have shown that there is an imbalance between MMPs and tissue inhibitors of MMPs (TIMPs), in favour of the MMPs, in various pathological conditions such as inflammatory joint disease, suggesting that, once activated, MMPs may not be sufficiently counteracted.11,14,15,21,28–30 However, as the extent of activation of the proMMPs remains an unknown variable in vivo, we can only speculate about the levels of activated MMPs. Inactivation of the MMPs involves specific TIMPs and the high molecular weight proteinase inhibitor α2 macroglobulin (α2M), which is abundantly present in body fluids31–33 and also in synovial fluid during inflammation.32,34,35 TIMP is thought of as a major inhibitor of MMPs at the tissue level; however, determination of specific MMP/TIMP complexes remains a challenge. It is suggested that α2M plays an important role in the inhibition of activated MMPs in body fluids.36 The active site of the MMPs in α2M/MMP complexes is shielded, which deactivates MMPs towards natural high molecular weight substrates such as collagen. Nevertheless, the quantity of α2M/MMP complexes can be determined using low molecular weight substrates, which can penetrate α2M and reach the “bite region” of the activated MMPs inside α2M.37
In the present study, synovial fluid levels of proMMP and TIMP-1 were measured, as well as MMP activity in α2M/MMP complexes (MMP activity). As collagenases and stromelysin may represent different aspects of joint disease—for example, destruction and inflammation38—both MMP-1 and MMP-3 were therefore investigated. We made comparisons between joint pathologies with prominent inflammation (pseudogout), primary osteoarthritis, and joint trauma (injury), which predisposes to the development of osteoarthritis.
METHODS
Patients and samples
The study groups were patients with acute pyrophosphate arthritis (pseudogout), anterior cruciate ligament rupture that was either isolated or combined with a tear of the meniscus or collateral ligament (injury), and primary knee osteoarthritis. Diagnosis was made by arthroscopy, radiography, assessment of joint fluid, and clinical examination. The diagnosis of acute pyrophosphate arthritis was based on the acute onset of symptoms consistent with this diagnosis, combined with the presence of pyrophosphate crystals demonstrated by joint fluid microscopy. No patient underwent surgery before joint fluid sampling. Pharmacological treatment before sampling was limited to analgesics or the occasional non-steroidal anti-inflammatory drug. All patients were symptomatic at the time of sampling. In this cross sectional study, each volunteer and patient supplied a sample at one time point only. For patients, sampling took place at various times after knee injury or after the onset of symptoms. The patients’ age at time of sampling and the lengths of time after the injury or after the start of symptoms are given in table 1. Collected synovial fluid was centrifuged at 2000×g for 10 minutes to remove cells and debris. Aliquots were then frozen at −70°C. The healthy knee control group has been described before.10,11
Sampling age and time after injury or start of symptoms in the different study groups
Patient related procedures were approved by the ethics review board of the Medical Faculty of Lund University.
ProMMP-1, proMMP-3, and TIMP-1
ProMMP-1, proMMP-3, and TIMP-1 concentrations in these samples were previously quantified by immunoassay.21 In short, collagenase-1, stromelysin-1, and TIMP-1 levels in synovial fluid were determined by a sandwich enzyme linked immunosorbent assay (ELISA) using monoclonal and polyclonal antibodies to the human recombinant proteins.21–23,39 These MMP assays detect the pro-form of the enzymes as well as active forms and the enzymes in complex with TIMP-1, but not the complexes between activated enzymes and α2M. It was shown previously that in synovial fluid samples of this type more than 90% of the MMP-3 detected by ELISA is in form of proenzyme.23 The assay for TIMP-1 detects only free TIMP-1.
MMP-1 and MMP-3 activity in MMP/α2 macroglobulin complexes
Measurements of MMP activity in α2M complexes were based on methods described previously by Beekman et al,32,34 DeGroot et al,40 and Riley et al.41 In short, MMP activity in 1/50 diluted synovial fluid samples (all dilutions and concentrations are final) was determined using fluorogenic MMP specific substrates TNO113-F (Dabcyl-Gaba-Pro-Cha-Abu-Smc-His-Ala-Cys(fluorescein)-Gly-Lys-NH2, 5 μM) and TNO003-F (Dabcyl-Gaba-Arg-Pro-Lys-Pro-Val-Glu-Nva-Trp-Arg-Cys(fluorescein)-Gly-Lys-NH2, 5 μM) for MMP-1 and MMP-3 assays, respectively. EDTA-free completeTM solution (Roche, Mannheim, Germany; one tablet in 10 ml) was added to all conditions to reduce non-MMP substrate conversion. All incubations and measurements were undertaken in 384-well plates, black with a clear flat bottom (Corning Inc, Corning, NY, USA). The increase in fluorescence which results from enzyme mediated cleavage of the substrates was measured for four hours at 30°C using Cytofluor 4000 (Applied Biosystems, Foster City, California, USA) at 485/530 nm (excitation/emission).
Statistical analysis
The statistical significance of the differences between groups was determined by Kruskal–Wallis one way analysis of variance on ranks. Data was analysed with SPSS software (Chicago, Illinois, USA). All tests were two tailed, and a probability (p) value of <0.05 was considered significant.
RESULTS
Injury patients: MMPs, TIMP-1, and time after injury
Comparison of the MMP and TIMP-1 levels in the injury patients versus the control group showed an increase in proMMP-1 (p = 0.029), proMMP-3 (p<0.001), MMP-1 activity (p<0.001), and TIMP-1 (p<0.001) in the injury group. MMP-3 activity did not differ between the injury patients and the controls (p = 0.189). Although the mean sampling age differed between the study groups (table 1), we have previously reported that neither age nor sex influences the joint fluid concentrations of these markers.14 MMP and TIMP-1 levels are shown in table 2.
ProMMP-1, proMMP-3, TIMP-1, MMP-1, and MMP-3 activity in MMP/α2 macroglobulin complexes in the various study groups
For further analysis, samples from injury patients were ordered by time after injury and evenly divided into six time “windows” (fig 1). Increased proMMP-1 and proMMP-3 levels, increased MMP-1 activity, and increased TIMP-1 levels were found in synovial fluid from injury patients immediately after the injury. The high levels of TIMP-1 that were found during the first two weeks after injury decreased significantly by the week 17 (p<0.001) and remained stable for the remainder of the study. MMP levels showed a different time course. Whereas proMMP-1 and proMMP-3 levels remained high throughout the same period, MMP-1 activity was increased (p<0.001) in the time window when a significant decrease in TIMP-1 levels was found. Later during the study, a significant decrease in proMMP-1 and proMMP-3 levels was found (weeks 17 to 58 and 180 to 1500 for proMMP-1 and proMMP-3, respectively). MMP-3 activity was not increased compared with controls and did not differ between the injury subsets (p = 0.17).

ProMMP-1 concentration (A), MMP-1 activity (B), TIMP-1 concentration (C), proMMP-3 concentration (D), and MMP-3 activity (E) in synovial fluid v time after injury (values are medians with standard errors). The whole group was divided into “time windows” based on time of sampling after injury: 0–0.6 weeks (n = 44), 0.6–2 weeks (n = 58), 2–17 weeks (n = 45), 17–57 weeks (n = 50), 58–170 weeks (n = 47), 180–1500 weeks (n = 39). Time of sampling after injury is reported on a logarithmic scale. Dashed line represents corresponding values in control groups. MMP, matrix metalloproteinase; proMMP, pro-matrix metalloproteinase; TIMP, tissue inhibitor of metalloproteinases.
MMP-1, MMP-3, and TIMP-1 levels: osteoarthritis and inflammatory arthritis
Levels of the MMPs and TIMP-1 for the arthritis study groups (osteoarthritis and inflammatory arthritis) v controls are shown in fig 2.
{kind=link}
{kind=link}
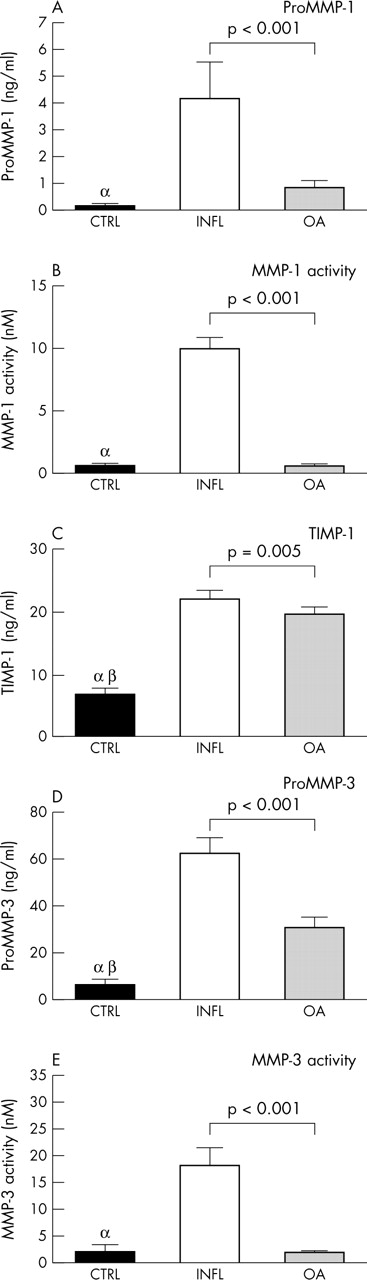
ProMMP-1 concentration (A), MMP-1 activity (B), TIMP-1 concentration (C), proMMP-3 concentration (D), and MMP-3 activity (E) in synovial fluid of the study groups (values are medians with standard error bars). CTRL, knee-healthy controls; INFL, inflammatory arthritis (pseudogout); OA, osteoarthritis. α: p<0.001, CTRL v INFL; β: p<0.001, CTRL v OA.
TIMP-1 levels (fig 2C) were increased in pseudogout and osteoarthritis compared with the controls (p<0.001 for both pseudogout and osteoarthritis), whereas levels of TIMP-1 in the injury group were initially at least twofold higher than in the pseudogout or osteoarthritis groups (p<0.001, injury v both pseudogout and osteoarthritis). At later times after joint injury, levels were comparable to the osteoarthritis and pseudogout groups.
ProMMP-1 values were greatly increased in the pseudogout group (detected in 90% of the samples) compared with the other study groups (p<0.001, pseudogout v all other groups). In the injury group, proMMP-1 was detected in 71% of the samples, whereas in the osteoarthritis and control groups it was detected in 26% and 11%, respectively. Active MMP-1 values were increased in the pseudogout and injury groups compared with the osteoarthritis and control groups (p<0.001, both pseudogout and injury v osteoarthritis or control groups).
ProMMP-3 values in joint fluid samples from pseudogout and injury patients were comparable and both were greatly increased compared with the osteoarthritis or control groups. In contrast to MMP-1, MMP-3 activity was increased in the pseudogout group only. No differences were found between injury, osteoarthritis, and control groups.
DISCUSSION
Our study shows the following for the first time:
-
increased MMP activity in α2 macroglobulin complexes in synovial fluid from patients with inflammatory arthritis and joint injury, accompanied by a high proMMP/TIMP-1 ratio;
-
the co-occurrence of an increase in MMP-1 activity in synovial fluid after joint injury and a significant decrease in TIMP-1 levels;
-
a higher degree of activation of MMP-1 compared with MMP-3 in synovial fluid from patients with joint injury.
Osteoarthritis is a slowly progressive joint disease characterised by deterioration in the articular cartilage over a long period.1 As joint injuries predispose to the development of osteoarthritis at a young age,42 it is likely that a single incident sets in motion a long lasting process with severe consequences for the joint cartilage. The molecular basis of the osteoarthritic process is not fully understood but studies of events following joint injury may provide clues to the processes that lead to osteoarthritis. Previously, we showed that increased levels of cartilage degradation products—such as aggrecan fragments and COMP—persist in synovial fluid from patients with joint injuries for a long time after the initial injury.12,13,21,43,44 Although the levels of both proMMPs and TIMPs are increased in synovial fluid after an injury,10,11,13,14,21–23 the proMMP/TIMP molar ratio is also increased, indicating a shift in favour of the MMPs. However, little is known about the activation of proMMPs in vivo. The results of the present study show that in addition to an increase in the proMMP/TIMP-1 ratio, increased levels of activated MMPs complexed with α2M are present in synovial fluid after joint injury and in joint inflammation. Activated MMPs are inhibited either by specific tissue inhibitors or by complex formation with α2M, a general protease scavenger. TIMP is considered to be a major MMP inhibitor at tissue level because tissue cells produce TIMP and high molecular weight α2M is unlikely to penetrate tissues such as articular cartilage. In body fluids, however, the situation is different. α2M is present in normal synovial fluid and in synovial fluid from patients with inflammatory conditions.36,45–47 It has previously been shown that in the presence of both TIMP and α2M, activated MMPs will be entrapped by α2M.36 As only activated MMPs will form complexes with α2M, the present findings suggest that pathological changes following joint trauma result not only in the increase of proMMP levels in synovial fluid but also in an increase in the levels of activated MMPs. Following complex formation between activated MMP and α2M, conformational changes occur at the surface of α2M and the proteinase/scavenger complex is rapidly cleared.48,49 It remains a challenge to measure MMPs complexed with TIMPs, and we are therefore unable to account for this variable in our study. Moreover, the clearance rates of low molecular weight proMMPs and MMP/α2M complexes may differ, which is why no hard conclusions can be drawn from the present data with regard to the relative proportions of activated MMPs and the proMMPs produced.
The increased MMP activity in pseudogout group is in line with previous observations of increased MMP/α2M levels in another inflammatory joint condition, rheumatoid arthritis.32,34,37,50 This suggests that increased levels of activated MMPs may be a common feature of joint inflammation. Moreover, the results show that increased MMP-1 activity in MMP/α2M complexes is found not only in pseudogout group but also in synovial fluid of injury patients. These findings indicate a similarity between joint inflammation and the initial stages of injury with regard to the changes in the proteolytic system, which may eventually lead to joint cartilage degradation and osteoarthritis. Additional studies are needed to investigate the precise relation between tissue and synovial fluid levels of the MMPs—that is, whether synovial fluid levels of measured MMPs represent the activity of the proteolytic system in joint tissue. Interestingly, an increase in MMP-1 activity was detected in the same time window during which the TIMP-1 levels in synovial fluid of injury patients were significantly decreased (fig 1). These observations support a role of α2M as a scavenger of activated MMPs, and indicate the applicability of MMP activity measurements using small fluorogenic substrates to study joint pathology. It should be noted that only one subclass of TIMPs (TIMP-1) was measured in the present study and that other TIMPs—such as TIMP-2 and TIMP-4—could contribute to the inhibition of MMP-1.51 Nevertheless, the increased levels of MMP/α2M complexes in synovial fluid of injury patients compared with the control group indicates that the net effect of the upregulation of the proteolytic system is free activated MMPs, despite an increase in TIMP levels following joint trauma.
Whereas significantly increased levels of activated MMP-1 were present in both the pseudogout and the injury groups, high levels of activated MMP-3 in this study were detected only in the pseudogout group. Although several explanations for these findings are possible, it seems most likely that proMMP-3 is not converted into the active form following injury to the same degree as in pseudogout. These results imply that increased proMMP-1 and proMMP-3 production under these conditions may have a different pathophysiological significance. Whereas the presence of proMMP-3 in synovial fluid is associated with synovitis, and activated MMP-3 is thought to activate multiple other proMMPs,52,53 activated MMP-1 is believed to play an important role in the degradation of type II collagen, one of the main components of the articular cartilage. Thus, while increased proMMP-3 levels in synovial fluid of injury patients do not result in increased levels of active MMP-3, and the biological significance of high proMMP-3 levels remains unclear, proMMP-1 is converted to its active form, which may contribute to deterioration of the articular cartilage and to the development of osteoarthritis.