Article Text

Abstract
Objective: Etanercept monotherapy has been studied and approved for treatment of polyarticular juvenile idiopathic arthritis (JIA). The following study evaluates the safety and efficacy of combination therapy of etanercept and methotrexate compared to etanercept monotherapy in JIA.
Methods: We perfomed an open, non-randomised study on patients who had previously failed to respond to at least one disease-modifying antirheumatic drug (DMARD). A total of 722 patients with JIA in whom at least 1 item of follow-up data was recorded were identified; of these, 118 patients treated with further slow acting drugs were excluded. In all, 504 patients were treated with a combination of etanercept and methotrexate. A total of 100 patients treated with etanercept only were in the control group. Efficacy was calculated using the American College of Rheumatology paediatric scores for 30, 50 and 70% improvement (PedACR30/50/70). Adverse events (AEs) and serious adverse events (SAEs) were reported.
Results: After 12 months 55 patients in the monotherapy group and 376 patients in the etanercept and methotrexate group were available for comparison. For the intention to treat analysis, 65 patients discontinuing treatment prematurely were included. All activity parameters decreased significantly in both treatment groups. After 12 months 81%/74%/62% of patients of the etanercept and methotrexate group and 70%/63%/45% of patients of the etanercept monotherapy group achieved PedACR30/50/70 scores, respectively (p<0.05 for PedACR30, p<0.01 for PedACR70). The likelihood of achieving a PedACR70 increased with combination therapy with an odds ratio of 2.1 (95% CI 1.2 to 3.5). In total, 25 infectious and 23 non-infectious SAEs including 3 malignancies occurred in the etanercept and methotrexate group, and 1 infectious and 3 non-infectious SAEs occurred in the single etanercept group.
Conclusions: The patients’ disease activity improved during etanercept monotherapy and etanercept and methotrexate combination therapy. Tolerability in both treatment groups was comparable.
Statistics from Altmetric.com
With an incidence of 19.8 per 100 000 children below the age of 16 years, juvenile idiopathic arthritis (JIA) is the most common chronic inflammatory disease in childhood and can lead to severe disability.1–4 Conventional therapy consists of disease-modifying antirheumatic drugs (DMARDs), corticosteroids and non-steroidal anti-inflammatory drugs (NSAIDs) with methotrexate as the most common first line DMARD. Treatment is not always successful, especially in patients with polyarticular and systemic subtypes.5–7 Anti-tumour necrosis factor (TNF)-α therapy with etanercept has shown success in patients with polyarticular JIA aged at least 4 years in a single randomised controlled study.8 9
In Germany, etanercept is licensed and recommended for children with polyarticular JIA after failure or intolerance of methotrexate.10 An earlier analysis showed that about 80% of patients with JIA were treated by combining etanercept and methotrexate instead of replacing methotrexate by etanercept.11 In adults with rheumatoid arthritis the combination of etanercept and methotrexate is associated with higher response rates.12 13
The aim of this prospective non-interventional observational study is to evaluate the safety and efficacy of combination therapy of etanercept and methotrexate versus monotherapy with etanercept in JIA, using data from the German Etanercept Registry.
METHODS
The German Etanercept Registry is a prospective database that has been maintained since 2001. After approval by the medical ethics committee at the site of the principal investigator (GH; Martin Luther University, Halle-Wittenberg, Germany), written consents were obtained and the data were collected in pseudonymous form. The patients’ history, previous and concomitant therapy were documented. All follow-up forms received prior to July 2007 were evaluated. A total of 26 patients with diseases other than JIA were excluded from the analysis. In all, 722 patients with JIA between the ages of 2 and 18 years were recruited from 45 centres. The patients were classified into seven subgroups according to International League of Associations for Rheumatology (ILAR) criteria (table 1).3 The decision to use methotrexate in combination with etanercept was not influenced by the Registry. The mean dosage of etanercept, methotrexate and prednisone equivalent is given in table 2.
Assessments used
Efficacy was assessed with the American College of Rheumatology paediatric scores for 30, 50 and 70% improvement (PedACR30/50/70) criteria, including the German Childhood Health Assessment Questionnaire (CHAQ) after 12 months of therapy.14–16 Analysis was performed using the intention to treat population (ITT) in all patients in whom the complete set of six core set criteria were available. All patients who discontinued prematurely due to poor efficacy, due to adverse events or at the patient’s request were labelled as non-responders. For patients who discontinued because of disease remission, their last PedACR response was carried forward. Patients who had been treated for less than the 12-month evaluation goal, but who had not discontinued treatment, were excluded from the ITT analysis. Other assessments not included in the PedACR score were the swollen and tender joint count, duration of morning stiffness and serum C-reactive protein (CRP) levels.
Safety analysis
Adverse events were elicited on every follow-up form after 1, 3 and 6 months of therapy and 6-monthly thereafter. Serious adverse events (SAEs) were defined as events that were fatal or life threatening, resulted in a persistent or significant disability or incapacity, or required or prolonged inpatient hospitalisation or led to a congenital anomaly or birth defect.
The reason for withdrawal of etanercept was also documented.
Statistical analysis
In order to compare differences in subtype distribution, in response rate as well as in the use of corticosteroids within the etanercept and methotrexate group and the control group the χ2 test was used. Calculated odds ratios were given with 95% CIs. Differences in single disease activity parameters between the groups were compared by unpaired Student t test if appropriate.
RESULTS
Patient characteristics
A total of 722 registered patients with JIA with at least one follow-up assessment prior to 30 June 2007 were identified. In all, 4510 follow-up assessment forms were obtained and were used for safety analysis. A total of 26 patients with autoimmune diseases other than JIA (eg, Crohn disease, colitis ulcerosa, Takayasu arteriitis, juvenile dermatomyositis, neonatal-onset multisystem inflammatory disease (NOMID), chronic recurrent multifocal osteomyelitis, sarcoidosis etc.) and 118 JIA patients treated with other DMARDs (eg, azathioprine, ciclosporine A, leflunomide, mycophenolate, chlorambucile, cyclophosphamide or thalidomide) were then excluded from the analysis. Of the remaining 604 patients, 504 patients were receiving combination therapy of methotrexate and etanercept and 100 patients were receiving etanercept only. The characteristics of the total patient group (504 patients in the etanercept and methotrexate group and 100 patients in the etanercept group) are summarised in tables 1 and 2. Both groups were comparable in terms of gender distribution, mean age at onset of the disease, mean disease duration, age when etanercept was started, antinuclear antibody (ANA) positivity and the presence of human leukocyte antigen (HLA)-B27. There were significant differences in JIA subtype distribution at baseline. There were more patients with rheumatoid factor positive polyarthritis in the etanercept and methotrexate group than in the etanercept group (p<0.01, χ2 test). Patients with the enthesitis related arthritis subtype of JIA were less frequent in the etanercept and methotrexate group than in the etanercept group (p<0.001, χ2 test).
There were 31 patients in the etanercept group and 77 patients in the etanercept and methotrexate group who had not reached the 12-month evaluation goal but had not discontinued treatment. A total of 376 patients in the etanercept and methotrexate group and 55 patients in the etanercept group were followed up for at least 12 months. The data of all patients treated with etanercept or etanercept and methotrexate with at least 12 months of follow-up not treated concomitantly with other therapy and those who discontinued prematurely were used to perform an intention to treat analysis.
A total of 65 patients discontinued etanercept prematurely (fig 1). In the etanercept group 14% of patients and in the etanercept and methotrexate group 10% of patients discontinued treatment with etanercept (p>0.05). Discontinuation due to intolerance was reported in 14 patients in the etanercept and methotrexate and in 3 patients in the etanercept group. Remission was the reason for discontinuation in six patients in the etanercept and methotrexate group but in none of the etanercept group. Poor efficacy led to discontinuation in 22 patients (4%) in the etanercept and methotrexate group and in 8 patients (8%) in the etanercept group.

Flow chart showing the number of patients included in the registry and those analysed for efficacy. Horizontal arrows indicate the group of patients excluded from the analysis at each step. ETA = etanercept, MTX = methotrexate, AE = adverse event.
At the start of treatment, some of the disease activity parameters differed in the two groups (table 2). Only the duration of morning stiffness was significantly prolonged in the combination group (p<0.05, Student t test). Steroids were used more frequently (62% vs 48%, p<0.025, χ2 test) in the latter group. However, the mean daily corticosteroid dosage in corticosteroid users was comparable.
Efficacy assessments
Patients in both groups demonstrated marked improvement in all disease activity parameters. Despite differences at start of treatment, after 12 months the residual disease activity was comparable in both groups expressed as mean (SD) (table 2).
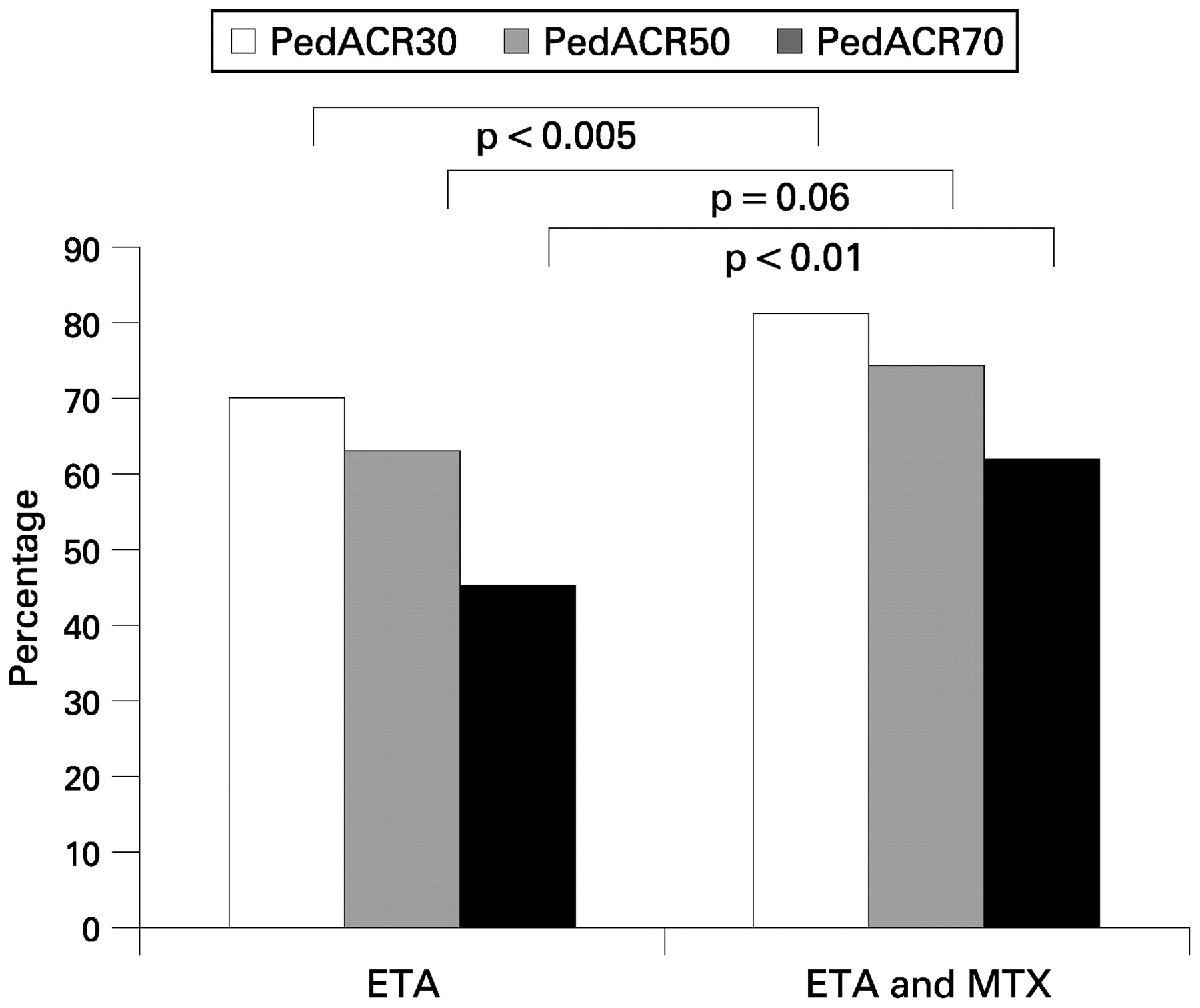
Analysis of PedACR criteria performed at 12 months in the intention to treat population is outlined in fig 2. The intention to treat population consisted of 376 patients in the etanercept and methotrexate group and 55 patients in the etanercept group who had been treated for at least 12 months, in addition to 51 patients and 14 patients who discontinued prematurely (fig 1). Of these, complete core set variables were available for 419 and 67 patients respectively. A total of 338/419 (81%) patients in the etanercept and methotrexate group and 47/67 (70%) patients in the etanercept monotherapy group achieved a PedACR30 (p<0.05); 310/419 (74%) patients in the etanercept and methotrexate group and 42/67 (63%) patients in the etanercept group reached a PedACR50 response (p = 0.55); 261/419 (62%) patients in the etanercept and methotrexate group and 30/67 (45%) patients in the etanercept group reached PedACR70 responses (p<0.01). The odds ratio for reaching a PedACR70 in the intention to treat analysis was 2.1 (95% CI 1.2 to 3.5) for patients treated with etanercept in combination with methotrexate compared to those treated with etanercept monotherapy.

{kind=link}
{kind=link}
Improvement rates of disease activity parameters after 12 months (right) of treatment for combination of etanercept and methotrexate compared to etanercept monotherapy. Improvement in the combination group was significantly more frequent than in the single treatment group (χ2 test).
Safety
Safety was assessed in all 604 patients with JIA receiving at least 1 dose of etanercept. There were 190 adverse events (AE) reported, occurring during 1149 patient years of exposure (table 3). There were 21 AEs in 14 patients in the etanercept group (0.21 AEs/patient in the population of 100 patients) and 169 AEs in 98 patients in the etanercept and methotrexate group (0.34 AEs/patient in the population of 504 patients, p<0.025, odds ratio of 1.9 (95% CI 1.1 to 3.2) for the risk of an AE in the combination group vs the control group). The rate of AE was 0.16 AEs/patient/year in the etanercept and methotrexate group and 0.15 AEs/patient/year in the etanercept group. The total rate of AE tended to decrease after the first year of treatment from 0.20 AEs/patient/first year to 0.12 AEs/patient/year thereafter, while the rate of SAE remained stable. In all, 52 AEs were graded as serious (SAE, table 3). There were 0.1 SAEs/patient in the etanercept and methotrexate and 0.04 SAEs/patient in the etanercept group. A total of 25 infectious SAE occurred in the etanercept and methotrexate group (0.05 per patient) and 1 in the etanercept monotherapy group (0.01 per patient, p>0.05 χ2 test). In all, 23 non-infectious SAE occurred in the etanercept and methotrexate group, 3 non-infectious SAE in the etanercept monotherapy group.
One non-familial carcinoma of the thyroid gland and one yolk sac carcinoma occurred in the etanercept and methotrexate group. The first patient started treatment with etanercept at the age of 17 years after a 3-year history of JIA. Thyroid carcinoma was detected 10 months later. Etanercept treatment was temporarily discontinued. JIA was diagnosed at the age of 14 years in the second patient. Etanercept was initiated after disease duration of 2.5 years. Yolk sac carcinoma was diagnosed 3 weeks later and etanercept was discontinued. In a third case non-Hodgkin’s lymphoma was detected. The patient’s history gave exposure to several antirheumatic drugs including methotrexate, azathioprine and ciclosporine A in addition to etanercept. There were no deaths.
There were several autoimmune diseases occurring or flaring-up during treatment with etanercept. Nine flare-ups of uveitis were reported as AE (four of them as SAE) in the etanercept and methotrexate group and two in the etanercept group (both SAE). In one patient with JIA, treatment with etanercept was started at the age of 7 years after disease duration of 2 years. Crohn disease was diagnosed after treatment duration of 2.5 years.
There was one case of Stevens–Johnson syndrome occurring in a female patient after initiation of oral contraceptive treatment during ongoing therapy with etanercept and methotrexate. Treatment with etanercept and contraceptive was discontinued and etanercept was successfully and safely reintroduced later on. One patient in the etanercept and methotrexate group developed double-stranded anti-DNA antibodies without clinical signs of lupus.
In the etanercept group there was one patient with transient hearing loss. Several neuropsychological adverse events were reported in a number of patients in the etanercept and methotrexate group. In two patients optic nerve papillitis was reported, in one patient white matter lesions were seen on MRI, two patients had seizures, one patient suffered from optic and acoustic hallucinations, frequent revulsion of feeling was reported in two patients, depression in another, tinnitus was reported in one patient. In one patient, diminished colour discrimination was possibly indicative of retrobulbar neuritis.
DISCUSSION
During the last decade methotrexate has become the standard treatment of polyarticular JIA. The TNF antagonist etanercept is the first biological approved for treatment of polyarticular JIA. Both drugs have been investigated in placebo-controlled randomised double-blind trials.7 8 Currently there is no randomised controlled trial with these drugs showing the tolerability as well as the superiority of combination therapy in patients with JIA.
Although the patients were followed up prospectively in a non-interventional, observational study, due to the non-randomised design of this observational study there were limitations. There were significant differences in several baseline variables between those patients treated by a combination of etanercept and methotrexate and those treated by etanercept monotherapy. In particular, the JIA subtypes were not equally distributed. Patients who used combination treatment seemed to show more disease activity at initiation of etanercept therapy than those with single treatment. These differences in disease activity parameters had disappeared after 12 months of treatment with etanercept, so that the relative reduction of symptoms due to therapy seemed to be more pronounced in the combination group.
However, all single disease activity parameters decreased in both groups. After 12 months of treatment patients receiving a combination of etanercept and methotrexate reached a PedACR30, 50 or 70 response more frequently than those on etanercept monotherapy. This was especially evident in the intention to treat population. In particular, the number of patients with JIA reaching a PedACR70 response was significantly higher in the etanercept and methotrexate group than in the etanercept monotherapy group. The same effect was observed in a last observation carried forward analysis including those patients with ongoing treatment for a shorter period of time (data not shown). Comparison of efficacy data has to be interpreted with caution because patients treated in the combination group received corticosteroids more frequently. The response levels in this observational study including high numbers of patients were comparably to those in the randomised controlled trial.8 Therefore, etanercept monotherapy as well as etanercept and methotrexate combination therapy would be effective therapeutic options for patients with JIA who do not respond to methotrexate and/or other DMARDs.
In the etanercept monotherapy group there were relatively more patients with enthesitis related arthritis. For this JIA-type, earlier studies have shown dramatic clinical improvement with etanercept monotherapy.17 18 In these studies, mostly data after 3–4 months of treatment were evaluated. In a 12 months study, only 39% of patients had a PedACR30 response.19 By contrast, in our study we observed sustained improvement in patients with enthesitis-related arthritis treated with etanercept monotherapy. Patients with rheumatoid factor negative polyarticular JIA in particular showed significantly higher response rates under combination therapy than under etanercept monotherapy. This subgroup of patients is the largest group of patients with JIA treated with etanercept. No difference was found for the systemic arthritis subgroup, or for the psoriasis and arthritis subgroup (data not shown).
The overall number of adverse events was low and only few patients discontinued treatment with etanercept because of intolerance. One of the limitations of our study was the voluntary reporting system of adverse events. The frequency of adverse events reported in patients in the combination group was not different to that of the control group when the time of exposure to the drug was taken into consideration. This indicates a very favourable interaction profile for the combination of etanercept and methotrexate. There seemed to be fewer serious AEs in the etanercept monotherapy group but the difference failed to reach statistical significance (p = 0.06, χ2 test). Infectious serious adverse events were also more frequent in the etanercept and methotrexate group. The rate of AEs declined after the first year of treatment, which may be due to infrequent reporting or to a bias whereby those patients still on treatment were those who best tolerated etanercept.
One case of suspected demyelinisation, which has already been published,20 and two further cases with optic papillitis were observed. The occurrence of demyelination during anti-tumour necrosis factor alpha therapy in further patients with JIA has already been described.20 There are a number of autoimmune diseases occurring or flaring up during treatment with etanercept, including uveitis and chronic inflammatory bowel disease. In one further patient treated with etanercept and Leflunomide, ulcerative colitis was diagnosed 3 months after treatment with etanercept was started. In addition, there were two patients listed in the registry treated with etanercept because of polyarthritis accompanying Crohn disease. In these two patients treatment was discontinued after 2 and 6 months respectively. In one of them, a noteworthy flare-up of Crohn disease had occurred during etanercept treatment. Crohn disease evolving under treatment with etanercept has also been diagnosed in patients so far classified as having JIA.19 Under treatment with etanercept, the occurrence and reoccurrence of uveitis have been described earlier and the therapeutic efficacy of etanercept in these diseases seemed to be limited as expected earlier.21 22
There were three malignant tumours, two detected several months and one only a few weeks after start of treatment with etanercept. The short duration of treatment before detection of a malignant tumour makes causality unlikely. Very recently however, a case of non-Hodgkin’s lymphoma has been reported to the registry. The patient’s history mentioned exposure to toxic agents including methotrexate, azathioprine and ciclosporine A in addition to etanercept. The incidence of malignancies in the German population between 2000 and 2004 was 14.7 per 100 000 children below the age of 15 years (http://www.kinderkrebsregister.de) which can be expressed as 0.0147/100 patient years. The rate of malignancies observed in this cohort was 3 in 1149 patient years (0.26/100 patient years). This must be interpreted with caution since these three cases cannot be easily attributed to treatment with etanercept and two of the patients were older than 15 years.
The number of patients discontinuing treatment was higher in the etanercept group than in the etanercept and methotrexate group, which is especially due to a higher number of patients discontinuing because of treatment failure. No patient discontinued treatment in the etanercept monotherapy group because of complete control of the disease activity.
In conclusion, etanercept as monotherapy and etanercept as combination therapy for more severely affected patients both have good long-term efficacy. Due to the nature of our study the results have to be considered preliminary. Further randomised controlled trials with an adequate duration are necessary to confirm our findings. All patients included in our analysis failed with at least one DMARD. The results of our observations can therefore not be extended to the general JIA population, especially to patients so far not exposed to methotrexate. Since a wide variety of AEs has been reported, a long-term follow-up of patients receiving etanercept monotherapy or combination therapy of etanercept and methotrexate is recommended.
Acknowledgments
The authors would like to thank L Nandini Moorthy of the Robert Wood Johnson Medical School, University of Medicine and Dentistry of New Jersey, New Brunswick, New Jersey, USA for her helpful comments on an earlier version of the manuscript. The German Etanercept Registry acknowledges the contributions of the German and Austrian Paediatric Rheumatology Collaborative Study Group (PRCSG). The following members of the PRCSG participated in data collection: Hospach A, Stuttgart; Urban A, Amberg; Linde T, Halle; Nimtz-Talaska A, Frankfurt/Oder; Borte M, Leipzig; Niehues T, Duesseldorf; Heubner A, Freital; Berger T, Datteln; Neudorf U, Essen; Brunner J, Insbruck; Baan A, Homburg; Mokroß C, Oldenburg; Weissbarth-Riedel E, Hamburg; Zimmermann O, Chemnitz; Terschluse K, Nordhausen; Möller J, Saarbrücken; Sailer-Höck M, Innsbruck; Ganser G, Sendenhorst; Benseler, S, Toronto; Kornbrust A, Bonn; Heubner G, Dresden; Gahr M, Dresden; Huocke C, Bremen; Huppertz I, Bremen; Ehl S, Freiburg; Schofer O, Neunkirchen; Thon A, Hannover; Roth J, Berlin; Keitzer R, Berlin; Kümmerle-Deschner J, Tübingen; Tzaribachev N, Tübingen; Küster RM, Bad Bramstedt; Quietzsch J, Plauen; Mathony K, Hamm.
REFERENCES
Footnotes
Competing interests: GH has been a member of the advisory boards for Wyeth Biopharma, Muenster, Germany, Abbott Pharma, Wiesbaden, Germany and Essex Pharma, Munich, Germany. GH is conducting clinical studies sponsored by Wyeth Biopharma, Muenster, Germany and Abbott Pharma, Wiesbaden, Germany.
Funding: The German Etanercept Registry is sponsored by Wyeth Biopharma, Muenster, Germany.
Ethics approval: Ethical approval was granted by the medical ethics committee at the site of the principal investigator (GH; Martin Luther University, Halle-Wittenberg, Germany); written consent was obtained and the data collected in pseudonymous form.