Article Text

Abstract
Background: Treatment of active ankylosing spondylitis (AS) with the recombinant, soluble tumour necrosis factor α (TNFα) receptor molecule etanercept has been shown to be clinically highly effective. The precise mechanism of action, however, is not known.
Objective: To assess the change in the cytokine secreting ability of CD4+ and CD8+ T cells and macrophages during etanercept treatment.
Patients and methods: Peripheral blood mononuclear cells from 10 patients with AS treated with 25 mg etanercept and 10 patients with AS treated with placebo were investigated during treatment given twice weekly subcutaneously. Production of cytokines by T cells was investigated after in vitro stimulation by flow cytometry.
Results: Twelve weeks of etanercept treatment induced a significant increase in the number of interferon γ (IFNγ) positive (14.2% (9.6–19.5%) before v 24.4% (13.4–36.4%) after) and TNFα positive CD4+ T cells (p=0.008 for both cytokines) and IFNγ positive (37.5% (19.0–45.4%) before v 52.9% (33.2–60.0%) after) and TNFα positive CD8+ T cells (p=0.008 for both cytokines) upon phorbol myristate acetate/ionomycin stimulation, but not in the placebo group. Furthermore, etanercept treatment induced a significant increase in the number of IFNγ positive CD8+ T cells (p=0.024 at 12 weeks) and a non-significant increase of TNFα positive CD8+ T cells after in vitro stimulation with the aggrecan derived peptides.
Conclusions: Neutralisation of peripheral TNFα does not induce a down regulation of the ability of T cells to produce TNFα but rather an up regulation, possibly due to a counterregulatory mechanism.
- tumour necrosis factor α
- interferon γ
- ankylosing spondylitis
- etanercept
- T cells
- AS, ankylosing spondylitis
- IFNγ, interferon γ
- IL, interleukin
- PMA, phorbol myristate acetate
- RA, rheumatoid arthritis
- TNFα, tumour necrosis factor α
Statistics from Altmetric.com
- AS, ankylosing spondylitis
- IFNγ, interferon γ
- IL, interleukin
- PMA, phorbol myristate acetate
- RA, rheumatoid arthritis
- TNFα, tumour necrosis factor α
In the past decade it has been shown that tumour necrosis factor alpha (TNFα) is a major contributor to the pathogenesis of synovitis and joint destruction in rheumatoid arthritis (RA). To date, two forms of TNF inhibition therapy have been extensively investigated in RA. Both the TNF receptor-Fc fusion protein (TNFR:Fc, etanercept) and the chimeric anti-TNFα monoclonal antibody (infliximab) have been proved to be highly active for the treatment of RA1,2 and psoriatic arthritis.3,4
We showed previously that TNFα is highly expressed in biopsy samples taken from sacroiliac joints of patients with ankylosing spondylitis (AS).5 Encouraged by this finding and by the positive results of TNF blockade in other diseases, we showed recently that the disease activity index of patients with AS improved impressively when they were treated with the anti-TNFα monoclonal antibody infliximab.6 Subsequently, in a placebo controlled trial a similar efficacy was shown for etanercept in the treatment of AS.7
Most recently, we also carried out a placebo controlled study with etanercept in 30 patients with AS. We obtained a similar good response8 compared with the other etanercept studies in AS7 and compared with our infliximab study in AS.6 We took advantage of this trial and investigated longitudinally the T cell cytokine pattern during the etanercept study both in the etanercept and in the placebo group during treatment to examine the mechanism of etanercept treatment.
PATIENTS AND METHODS
Patients and design of the clinical study
In this placebo controlled double blind study 10 patients were randomly assigned to receive etanercept and 10 patients to placebo treatment. In the etanercept group patients were treated with 25 mg etanercept given twice weekly subcutaneously for 12 weeks, while patients of the placebo group were treated with placebo for six weeks and afterwards were switched to etanercept treatment for another six weeks.8 Cytokines were investigated in both groups before, six weeks, and 12 weeks after treatment.
In vitro stimulation of T cells by non-specific and specific antigen and analysis by flow cytometry
Peripheral blood mononuclear cells (1×106) were cultured for six hours either in the presence of 5 ng/ml phorbol myristate acetate (PMA; Sigma, St Louis, MO) plus 1 ng/ml ionomycin (Sigma, St Louis, MO), or stimulated with a pool of 46 overlapping 18-mer peptides (5 μg/ml for each peptide) derived from the G1 domain of aggrecan in the presence of anti-CD28 (1 μg/ml; Immunotech, Marseille, France), as described previously.9 After this, cells were fixed and quadruply stained for surface markers CD3 (PE) and CD8 (Perc P) (Becton Dickinson, Heidelberg, Germany) and for two intracellular cytokines, either interferon γ (IFNγ; FITC)/interleukin (IL)4 (APC) or TNFα (FITC)/IL10 (APC) (Pharmingen, San Jose, CA). Positive cells were subsequently quantified by flow cytometry using a FACSCalibur from Becton Dickinson (San Jose, CA) with Cellquest software.9
Statistical analysis
Because numbers in each groups were small the Wilcoxon test was used to compare cytokine production before and after treatment in the etanercept group, and before and after placebo or etanercept treatment in the placebo group. The medians and the 25th to 75th centiles are given. Differences were considered to be significant with a two tailed p value of <0.05.
RESULTS
Etanercept treatment induces an increase in the number of IFNγ and TNFα positive T cells after non-specific in vitro stimulation
For the etanercept group, a significant change in the IFN or TNFα production by CD4+ T cells could be seen after 12 weeks of treatment but not yet after six weeks upon PMA/ionomycin stimulation at this time (fig 1).

A significant increase in the production of IFNγ and of TNFα by CD4+ T cells upon PMA/ionomycin stimulation was observed after 12 weeks of etanercept treatment in the etanercept group. *p=0.008, compared with before treatment, but no change in the cytokine production was detected after six weeks of etanercept treatment in the placebo group. The medians and ranges of non-specific cytokine production are indicated in the figure.
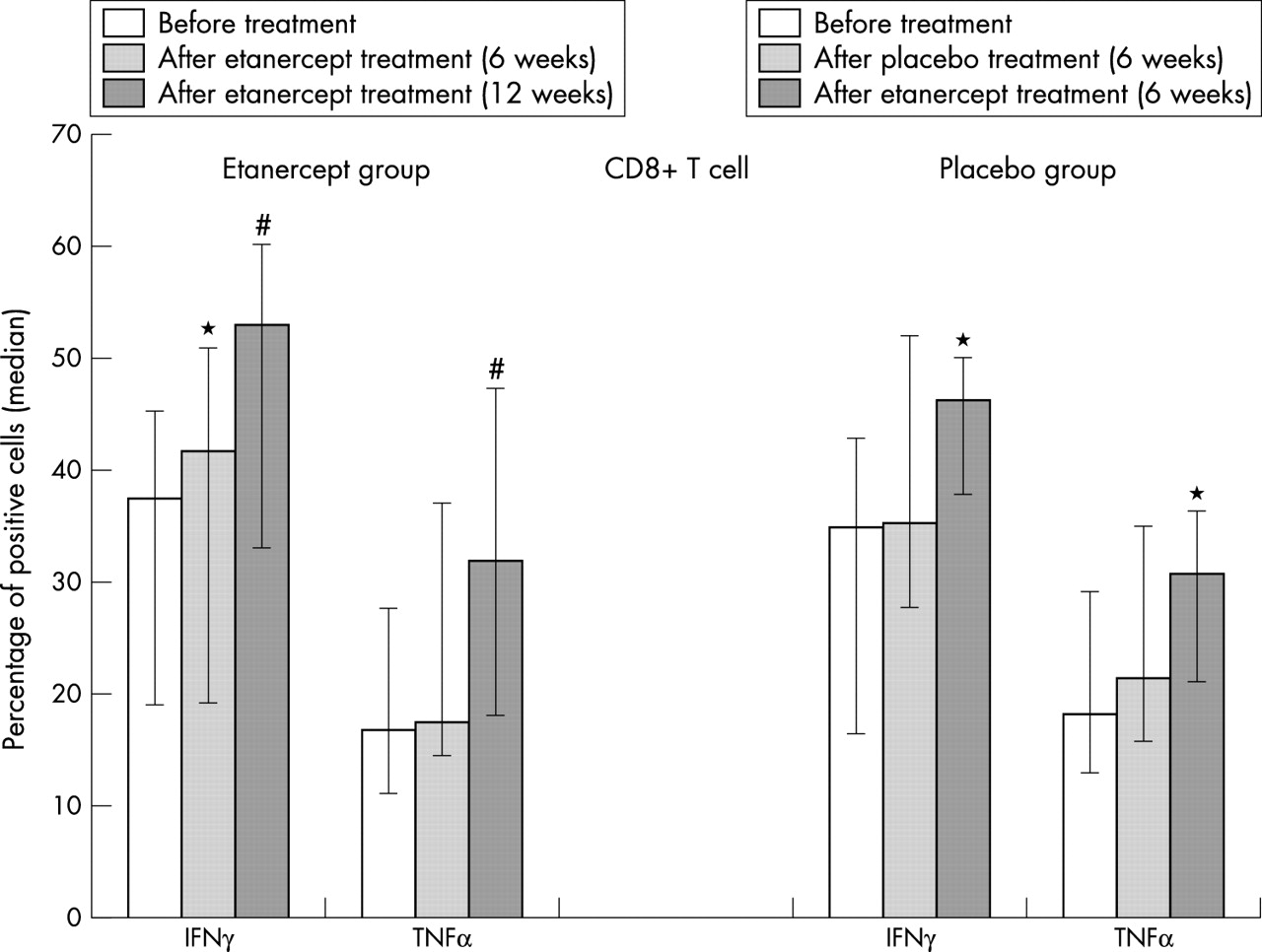
In the CD8+ T cell population, six weeks of etanercept treatment induced a significant increase in the number of IFNγ positive (p<0.05) but not yet in the number of TNFα positive CD8+ T cells (fig 2). The increase became even clearer for cytokine production of CD8+ T cells after 12 weeks of etanercept treatment (fig 2).
{kind=link}
{kind=link}
A significant increase in the production of IFNγ and of TNFα by CD8+ T cells upon PMA/ionomycin stimulation is seen during etanercept treatment. No change in the cytokine production was detected after six weeks of treatment in the placebo group, but a significant increase in the production of IFNγ and of TNFα by CD8+ T cells upon PMA/ionomycin stimulation was seen after the patients were switched to etanercept treatment. The median and range of non-specific cytokine production are indicated in the figure. *p<0.05 compared with before treatment; #p=0.008 compared with before treatment.
In contrast, no change in the number of IFN or TNFα positive CD4+ and CD8+ T cells was seen during six weeks of placebo treatment upon PMA/ionomycin stimulation (figs 1 and 2). When these patients were switched to etanercept treatment, a similar increase in the cytokine production by CD8+ T cells was seen (p<0.05 for difference between before and after etanercept treatment for both cytokines) (fig 2) but only a non-significant increase occurred for these cytokines secreted by CD4+ T cells (fig 1).
Etanercept treatment induces an increase of IFNγ production by CD8+ T cells after antigen-specific in vitro stimulation
After six weeks of etanercept treatment, a significant increase of IFNγ positive but not of TNFα positive cells was found in the CD8+ subpopulation and a similar result was found after 12 weeks of treatment (table 1). There was no change in the number of IFN and TNFα positive CD4+ T cells after treatment upon in vitro stimulation with aggrecan G1 peptides.
IFNγ production by CD8+ T cells after etanercept treatment
No change was seen in the placebo group, but IFNγ positive antigen-specific CD8+ T cells increased significantly after the patients were treated with placebo.
No change in IL4 or IL10 positive T cells during treatment
In both the etanercept and the placebo group, no significant changes of non-specific IL4 and IL10 secretion were seen during treatment (data not shown). G1 peptide-specific stimulation of T cells did not induce IL4 or IL10 secretion before or after treatment.
DISCUSSION
In this study we showed that treatment of patients with active AS with the soluble TNF receptor etanercept increases both TNFα secretion and IFNγ secretion in the CD4+ T cell subpopulation after non-specific in vitro stimulation (at 12 weeks), but even more clearly in the CD8 subpopulation (at six and 12 weeks). We also observed an increase in the antigen-specific IFNγ production of CD8+ T cells at six and 12 weeks, but no change occurred during placebo treatment. Interestingly, there was no clear effect on monocyte production of TNFα upon in vitro stimulation with lipopolysaccharide during treatment (data not shown).
It has been suggested that TNFα has an inhibitory effect on T cell function, which can be restored by TNFα blockade.10–12 However, although our results are compatible with such an assumption, we showed that, in contrast with our study with etanercept, during treatment of patients with AS with infliximab both the non-specific and antigen-specific secretion of TNFα and IFNγ by T cells is significantly down regulated, a finding which also correlated well with a good clinical response.6,13 Thus, direct inhibition of TNFα by the TNFα blocking agents, and not restoration of immunosuppression induced by the disease, seems to be important. Although etanercept and infliximab seem to be similarly effective in the treatment of RA1,2 and AS,6–8 there are two important clinical differences: (a) infliximab is highly effective in Crohn’s disease,14 whereas etanercept is not15; (b) infliximab treatment seems to be associated with an increased rate of infection with Mycobacterium tuberculosis, whereas patients treated with etanercept seem to be less affected.16 Whether a differential effect of the two drugs on T cell function can offer an explanation for this difference remains to be shown.
This small increase in the ability of the T cells to produce TNFα and IFNγ was accompanied by a good clinical effect,8 indicating that neutralisation of soluble TNF without affecting T cell function is efficient. This increase might be explained by a counterregulatory effect on T cells.
Acknowledgments
We thank Peihua Wu, Martina Grolms, and all the doctors in the department of rheumatology for providing samples from patients and for technical assistance.