Article Text

Abstract
Objectives To investigate whether a treat-to-target strategy with methotrexate and intra-articular glucocorticosteroid injections suppresses MRI inflammation and halts structural damage progression in patients with early rheumatoid arthritis (ERA), and whether adalimumab provides an additional effect.
Methods In a double-blind, placebo-controlled trial, 85 disease-modifying antirheumatic drug-naïve patients with ERA were randomised to receive methotrexate, intra-articular glucocorticosteroid injections and placebo/adalimumab (43/42). Contrast-enhanced MRI of the right hand was performed at months 0, 6 and 12. Synovitis, osteitis, tenosynovitis, MRI bone erosion and joint space narrowing (JSN) were scored with validated methods. Dynamic contrast-enhanced MRI (DCE-MRI) was carried out in 14 patients.
Results Synovitis, osteitis and tenosynovitis scores decreased highly significantly (p<0.0001) during the 12-months’ follow-up, with mean change scores of −3.7 (median −3.0), −2.2 (−1) and −5.3 (−4.0), respectively. No overall change in MRI bone erosion and JSN scores was seen, with change scores of 0.1 (0) and 0.2 (0). The tenosynovitis score at month 6 was significantly lower in the adalimumab group, 1.3 (0), than in the placebo group, 3.9 (2), Mann–Whitney: p<0.035. Furthermore, the osteitis score decreased significantly during the 12-months’ follow-up in the adalimumab group, but not in the placebo group, Wilcoxon: p=0.001–0.002 and p=0.062–0.146. DCE-MRI parameters correlated closely with conventional MRI inflammatory parameters. Clinical measures decreased highly significantly during follow-up.
Conclusions A treat-to-target strategy with methotrexate and intra-articular glucocorticosteroid in patients with ERA effectively decreased synovitis, osteitis and tenosynovitis and halted structural damage progression as judged by MRI. The findings suggest that addition of adalimumab is associated with further suppression of osteitis and tenosynovitis.
- Rheumatoid Arthritis
- Magnetic Resonance Imaging
- Treatment
Statistics from Altmetric.com
Introduction
Early and aggressive treatment with disease-modifying antirheumatic drugs (DMARDs) markedly improves short-term and long-term outcome in patients with rheumatoid arthritis (RA).1 However, the optimal treatment strategy of patients with early RA (ERA), including choices such as initial monotherapy versus combination therapy, and the role of glucocorticosteroids and biological agents has still not been settled.2 ,3 Trials including active comparators rather than a traditional placebo arm, require sensitive outcome measures to be able to distinguish reliably between therapeutic strategies.4 ,5
MRI demonstrates better sensitivity to change and discrimination between treatment arms in clinical trials with a validated scoring system such as the Outcome Measures in Rheumatology Clinical Trials (OMERACT) RA MRI scoring system (RAMRIS).4–6 The OMERACT RAMRIS system provides semiquantitative assessment of synovitis, osteitis and MRI bone erosion.7–9 Furthermore, tenosynovitis10 and OMERACT joint space narrowing (JSN)11 ,12 scoring systems have been developed, but have not yet been applied in multicentre clinical trials.
The aim of this study was to investigate whether a treat-to-target strategy with methotrexate and intra-articular glucocorticosteroid injections suppressed synovitis, osteitis and tenosynovitis, and halted progression of structural damage (MRI bone erosion and JSN) in patients with ERA, and whether adalimumab provided an additional effect, as judged by MRI.
Patients and methods
This is an MRI substudy of the OPERA trial (OPtimised treatment algorithm in Early Rheumatoid Arthritis),13 an investigator-initiated, randomised, double-blind, placebo-controlled, two-armed, parallel-group, multicentre study. One hundred and eighty DMARD-naïve patients with ERA, disease duration <6 months and a 28-joint count Disease Activity Score (DAS28) >3.2 were included. All patients received oral methotrexate (increased to 20 mg/week over 2 months) in combination with placebo–adalimumab or adalimumab 40 mg subcutaneously every other week. Patients were followed up for 12 months, with monthly visits for the first 3 months and visits every 3 months thereafter. At all visits, swollen joints were injected with triamcinolone hexacetonide (20 mg/mL, 0.5–2 mL/joint, maximum four joints and 4 mL per visit).13 Details of the OPERA MRI substudy are described below.
Patients
Patients included in the OPERA trial at sites where MRI was available were invited to participate in the OPERA MRI substudy. Eighty-five patients were included from August 2007 to December 2009 with 43 patients in the placebo group and 42 patients in the adalimumab group. Exclusion criteria were as in the main study (http://www.clinicaltrials.gov, NCT00660647): serum-creatinine > upper normal limit and contraindications for contrast-enhanced MRI (allergy, claustrophobia). During 12 months’ follow-up nine patients were excluded owing to high disease activity (placebo/adalimumab: 1/1), non-compliance (2/1), patient's wish (1/1), malignancy (1/0) and leucopenia (0/1). Thus, 38 patients in each treatment group completed the trial.
MRI
MRI of the right 2nd–5th metacarpophalangeal (MCP) joints and the wrist joint were obtained at baseline, and after 6 and 12 months of treatment. The MRI units used in the different centres were a 0.6 T Philips Panorama MRI unit (Herlev, 31 patients), a 1.0 T Oni OrthOne MRI unit (Graasten, 30 patients), a 3.0 T Philips Achieva MRI unit (Aarhus, 15 patients) and a 1.5 T GE Sigma HDxt MRI unit (Aalborg, nine patients), respectively. At all centres, the hand was placed in a dedicated extremity coil.
Coronal isometric high-resolution, gradient-echo, T1-weighted sequences were obtained before and after an intravenous bolus injection with a gadolinium-containing contrast agent (gadoteric acid 0.2 mL/kg body weight, Dotarem) and a precontrast coronal short tau inversion recovery (STIR) sequence.
The following imaging parameters were used for the STIR sequence: repetition time (TR) 2300–4500 ms, echo time (TE) 24.4–102 ms, inversion time (TI) 90–200°, field of view (FOV) 120–160 mm2, matrix 180–256×196–256, slice thickness 2–3 mm; and for the T1-weighted sequences: TR 20 ms, TE 8 ms, flip angle 15–65°, FOV 100–160 mm2, matrix 216–288×192–283, slice thickness 0.7–0.8 mm (reconstructed to 0.4 mm).
After 1 September 2007, the MRI protocol at Herlev included a T1-weighted gradient-echo dynamic sequence obtained at the time of the contrast injection. Fourteen patients were included in the dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) protocol, for which the imaging parameters were as follows: TR 33 ms, TE 4.2 ms, flip angle 25°, FOV 200 mm2, matrix 108×192, slice thickness 3 mm.
Image evaluation
One reader scored all conventional MRI for synovitis, osteitis, MRI bone erosion, JSN and tenosynovitis. The reader was blinded to clinical and other imaging data, treatment group and chronology. Using the RAMRIS system, synovitis was scored 0–3 in three wrist regions and in 2nd–5th MCP joints, total scores 0–21. Osteitis was scored 0–3 and bone erosion 0–10 in the wrist and MCP joint bones,9 JSN 0–4 in 21 joints in wrist and MCP joints11 and tenosynovitis at the wrist 0–3 in 10 wrist compartments.10
DCE-MRI findings were analysed using the image processing software Dynamika V.4.6.0 (http://www.imageanalysis.org.uk, London, UK). The number of enhancing voxels (Nvoxel), initial rate of enhancement (IRE) and maximum enhancement (ME) were extracted from manually delineated regions of interest positioned to include the entire wrist joint and to exclude enhancing voxels due to blood vessels and tenosynovitis, as previously described.14
Twenty-four MRI sets, of which 10 also included a dynamic sequence, were re-anonymised and scored a second time for calculation of intrareader agreement.
Conventional radiographs of both hands (posterior–anterior projection) and forefeet (anterior–posterior projection) were scored according to the Sharp/van der Heijde method.15
Clinical and laboratory evaluation included swollen joint count and tender joint count of 28 joints, visual analogue scale (VAS) patient's global, VAS fatigue and VAS pain, VAS physician's global, Health Assessment Questionnaire score, and serum C-reactive protein (CRP).
Outcome measures
MRI status scores and changes between time points (‘change scores’) of synovitis, osteitis, MRI bone erosion, JSN and tenosynovitis were used. Further, an osteitis score of 0 and synovitis score of ≤5 were noted, and used as a measure of MRI remission.16 Clinical outcome measures were DAS28, low disease activity (DAS28-CRP <3.2), European League Against Rheumatism (EULAR) response rates, remission rates (DAS28-CRP <2.6) and ACR/EULAR 28 Boolean remission.
Statistics
Analyses were carried out for as-observed data only, without data imputation or intention-to-treat analysis. Non-parametric statistics were used. Comparisons between groups were tested using χ2/Fisher's exact test (dichotomous responses) and Mann–Whitney U test (non-dichotomous responses), and comparison between time points was tested using Wilcoxon's signed-ranks test. A value of p<0.05 was considered statistically significant.
The intrareader agreement was tested using intraclass correlations coefficient (two-way mixed, absolute agreement).
Results
Baseline characteristics of the patients are presented in table 1. In the MRI substudy, there were no statistically significant differences between the treatment groups in any demographic, clinical and MRI baseline characteristics. However, the patients in the MRI subgroup had less disease activity than the patients who did not participate in the MRI substudy, table 1.
Demographic and clinical baseline characteristics of the participants of the OPERA trial, the participants in this MRI substudy and those not included in this MRI substudy are presented separately
MRI measures of disease activity
The synovitis, osteitis and tenosynovitis scores at baseline were median 7 (range 0–21), 1 (0–35) and 4 (0–26), respectively, and they all decreased markedly from baseline to 5 (0–13) (p<0.0001), 0 (0–35) (p=0.001) and 0 (0–18) (p<0.0001) at 6 months and 4 (0–15), 0 (0–36) and 0 (0–30) (all p<0.0001) at 12 months (table 2).
MRI, clinical and radiographic status scores for all patients and for patients in the placebo and the adalimumab groups
After 6 and 12 months the MRI synovitis change scores were median −3.5/mean −3.6 and −3.0/−3.7, the MRI osteitis change scores were 0.0/−2.9 and −1.0/−2.2 and the tenosynovitis change scores were −3.0/−4.3 and −4.0/−5.3 after 6 and 12 months, respectively. After 6 months, the tenosynovitis score was higher in the placebo group than in the adalimumab group (p=0.04), while the synovitis and osteitis scores did not differ between the two treatment groups.
The decreases in the synovitis and tenosynovitis scores were statistically significant in both treatment groups, while the osteitis score decreased significantly in the adalimumab group (p=0.001 and p=0.002 after 6 and 12 months, respectively), but not in the placebo group (p=0.146 and p=0.062 after 6 and 12 months), figure 1.

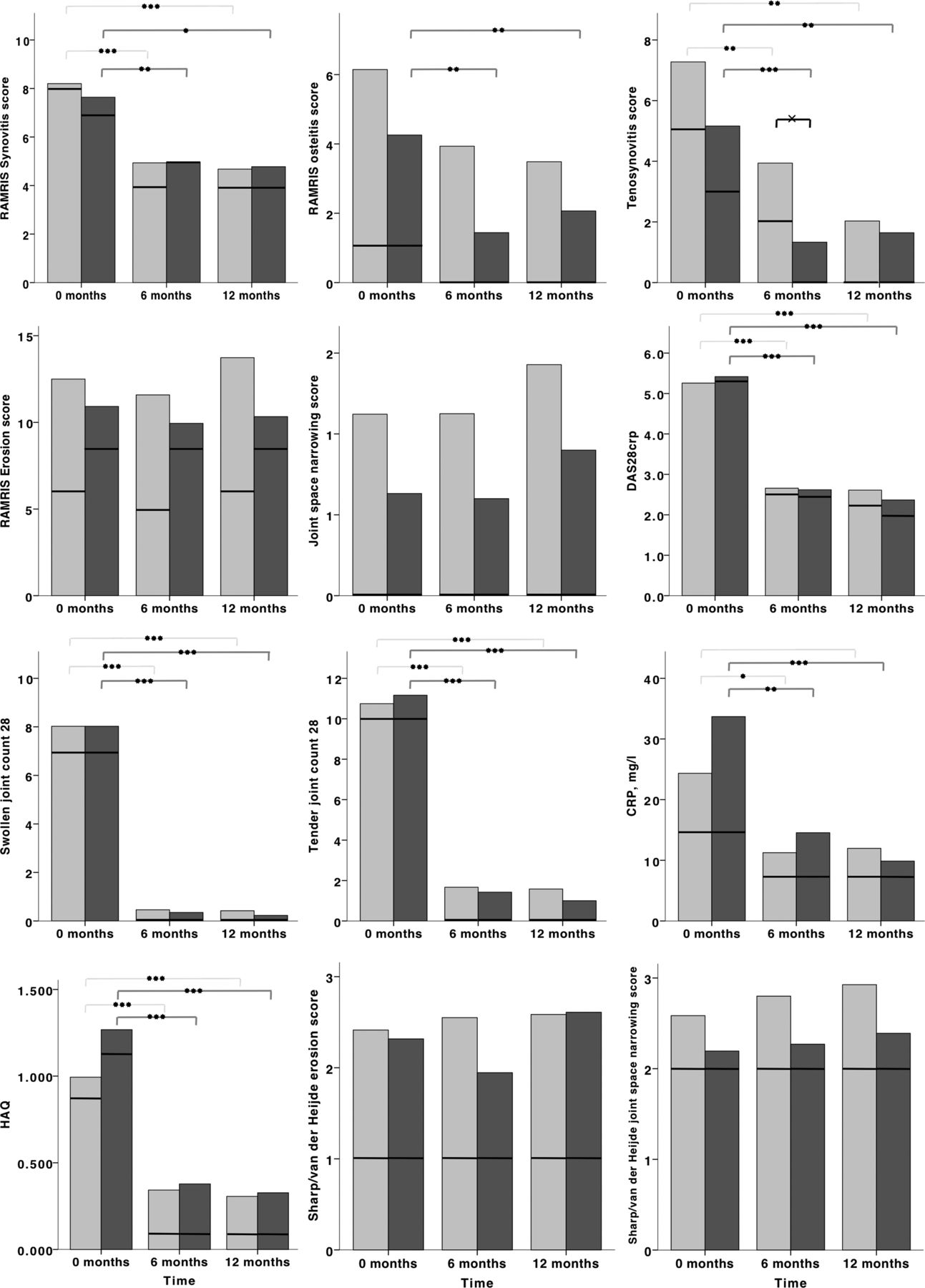{kind=link}
Light grey bars: placebo group; dark grey bars: Adalimumab group. Bars represent mean values, and lines in bars represent median values. Changes from 0 months to 6 and 12 months were tested using Wilcoxons test: *p<0.001; **p≤0.005; ***p≤0.0001. Differences between groups were tested by Mann-Whitney's test: x, p≤0.05.
Clinical measures of disease activity
Clinical outcome measures of disease activity are presented in table 2. All clinical measures decreased highly significantly in both treatment groups from baseline, all p<0.009. There was no statistically significant difference between the two treatment groups in any of the scorings, data not shown.
MRI and clinical low disease activity and remission
At baseline, 25% of patients met the proposed MRI remission criteria, 38% had no osteitis and 33% had a synovitis score ≤ 5. The numbers were 43%, 61% and 55% after 6 months of treatment and 43%, 62% and 60% after 12 months of treatment. At the same time 78% of the patients had reached low disease activity (DAS28 <3.2) and 65% had reached clinical remission (DAS28 <2.6). The EULAR good response and the 28 Boolean remission criteria were met by 77% and 33%, respectively. There were no statistical differences between the two treatment groups for MRI or clinical low disease activity or remission criteria.
DCE-MRI data
Baseline values of Nvoxel, IRE, ME and the composite parameters IRE×Nvoxel and ME×Nvoxel are presented in table 3. In the 14 patients examined by DCE-MRI, numerical, but not statistically significant decreases in Nvoxel, IRE and ME from baseline to after 6 and 12 months were seen. For these 14 patients, the RAMRIS scores showed no statistically significant changes either, and the DCE-MRI outcome measures were highly correlated to the wrist RAMRIS disease activity scores (Spearman's r: 0.718–0.837 for synovitis, p≤0.0001–0.002, and r: 0.547–0.611, p≤0.0001–0.001 for osteitis). The correlations to the total OMERACT RAMRIS synovitis, osteitis and tenosynovitis scores were slightly lower, but still highly significant (table 3).
Status DCE-MRI and conventional MRI status scores and correlations between baseline status and change DCE and conventional MRI scores
Measures of structural damage
The MRI bone erosion and JSN status scores are presented in table 2. At baseline, the median (range) MRI bone erosion and JSN scores were 7 (0–64) and 0 (0–8). The median/mean change scores from baseline to 6 and 12 months were 0.0/−1.3 and 0.0/0.1 for MRI bone erosion, and 0.0/−0.2 and 0.0/0.2 for JSN. There were no significant changes in structural damage scores over time (table 2) or between the two treatment groups.
The total Sharp/van der Heijde score scores were 3 (0–31), 3 (0–35) and 4 (0–32) at baseline and after 6 and 12 months, respectively, table 2. There were no significant changes in radiographic scores or differences between the two treatment groups during the 12-months’ follow-up.
The MRI and radiographic structural damage status scores were highly statistically significantly correlated. The Spearman's r between MRI and the radiographic erosion scores was 0.317, p<0.0001 and between MRI and radiographic JSN scores 0.451, p<0.0001. The correlations between the radiographic and MRI structural change scores were not statistically significant, data not shown.
Reliability
The intrareader agreement, calculated as the intraclass correlation coefficient, ICC (95% CI), for the RAMRIS MRI measures was synovitis: 0.90 (0.85 to 0.94); osteitis: 0.91 (0.81 to 0.96); tenosynovitis: 0.69 (0.53 to 0.80); MRI bone erosion: 0.85 (0.77 to 0.91) and JSN: 0.84 (0.75 to 0.90). For the 0–6/12 months change scores, the ICC was: synovitis: 0.78 (0.54 to 0.90)/0.85 (0.66 to 0.94); osteitis: 0.79 (0.53 to 0.91)/0.82 (0.60 to 0.92); tenosynovitis: 0.86 (0.64 to 0.95)/0.52 (0.09 to 0.79); MRI bone erosion: 0.11 (−0.35 to 0.53)/0.27 (−0.20 to 0.64) and JSN: 0.37 (−0.03 to 0.67)/0.10 (−0.35 to 0.50).
The intrareader agreement, ICC (95% CI) for the DCE-MRI measures was Nvoxel: 0.94 (0.89 to 0.97); IRE: 0.76 (0.58 to 0.87); ME: 0.12 (−0.20 to 0.43); IRE×Nvoxel: 0.96 (0.93 to 0.98) and ME×Nvoxel: 0.95 (0.90 to 0.97). For the DCE-MRI 0 to 6/12 months change scores, the ICC was Nvoxel: 0.93 (0.72 to 0.99)/0.95 (0.81 to 0.99); IRE: 0.96 (0.83 to 0.99)/0.82 (0.45 to 0.95); ME: 0.96 (0.83 to 0.99)/0.21 (−0.49 to 0.72)NS; IRE×Nvoxel: 0.96 (0.83 to 0.99)/0.97 (0.89 to 0.99); ME×Nvoxel: 0.94 (0.74 to 0.99)/0.95 (0.83 to 0.99).
Discussion
We found that aggressive combination treatment with methotrexate and intra-articular glucocorticosteroid, with or without adalimumab, effectively decreased MRI disease activity in patients with ERA, and that there was no MRI structural damage progression by 1 year. Adalimumab seemed to have an additive effect in suppressing osteitis and tenosynovitis. The improvement in MRI measures of inflammation was considerable, with mean changes in synovitis −3.6/−3.7, osteitis −2.9/−3.3 and tenosynovitis −4.3/−5.3 from baseline to 6/12 months. These figures are numerically higher than previously reported.6 ,17 ,18 In a 6-months’ trial including DMARD and tumour necrosis factor inhibitor naïve patients with RA, synovitis and osteitis scores decreased by −2.4 and −2.3 (mean values), respectively, during combined MTX and golimumab therapy.6 In two other randomised, placebo-controlled trials, patients with active RA despite methotrexate (MTX) therapy were treated with MTX±abatacept/placebo and MTX±golimumab/placebo, respectively. In the MTX±abatacept study,17 the mean synovitis (wrist) score decreased from 4.5 to 4.0 after 4 months treatment and the mean osteitis score (wrist and MCP) decreased from 7.7 to 5.8. In the MTX±golimumab study18 the mean synovitis and osteitis scores (wrist+MCP joints) decreased by 1.1 and 1.7, respectively. In both those studies, the decreases in the MTX+placebo groups were smaller than in the groups receiving active combination treatment, which was not the case in our study. In our study we used aggressive treatment with frequent visits by both treatment arms, and all patients were treated with intra-articular glucocorticosteroid injections in any swollen joint, which might explain the marked decrease in the MRI inflammatory measures in both treatment groups. However, it should be emphasised that the median total dose of triamcinolone hexacetonide used in this study corresponded to about 1 mg prednisolone a day during the 12-months’ follow-up, and there was no difference between the two treatment groups. This indicates that intra-articular injection with glucocorticosteroid is an effective treatment of inflammation in patients with RA, and that only a small cumulative dose is needed.
In the total OPERA trial population (180 patients),13 all clinical outcome measures decreased in both treatment groups, and more patients in the adalimumab group than in the placebo group met the strict response indices (ACR/EULAR 28 joint remission and DAS28 <2.6) during follow-up.13 We did not find similar differences in the clinical and MRI responses in the MRI substudy. However, patients participating in the MRI subgroup generally had a lower clinical disease activity at baseline than those who did not participate in this substudy and the difference in sample size (180 vs 85), might explain the differences between the cohorts. Further, we analysed data as-observed only, and did not perform data imputation on missing data or an intention-to-treat analysis. Using this approach some of the real differences between treatment groups might have been missed.
The tenosynovitis score decreased significantly more in the adalimumab group than in the placebo group. This is an important finding, as tenosynovitis has been found to be a predictor of erosive progression in patients with early RA.19 Further, the decrease in the osteitis score was only significant in the adalimumab group, indicating that the suppression of inflammation was better in the adalimumab group than in the placebo group. The difference in the tenosynovitis and osteitis changes in the two treatment groups is in accordance with the finding in the entire OPERA cohort that radiographic progression was less in the adalimumab group than in the placebo group,13 although we could not show the same difference in the 1-year follow-up in this subgroup of patients. After 12 months of treatment, the proposed MRI remission state (osteitis score=0 and synovitis score ≤5) was reached by 41% and 46% in the placebo and the adalimumab group, respectively. Both synovitis and osteitis have been found to be predictive of subsequent MRI bone erosion, and tight control of these two measures is important.16 ,20 ,21 The synovitis cut-off point was selected based on an international study documenting a minimal risk of erosive progression in patients with a synovitis score ≤5.16 The proportion of patients reaching clinical low disease activity and remission was comparable to that in the entire OPERA cohort.13
DCE-MRI parameters were tested as potential future outcome measures in a subset of 14 patients. There were no statistically significant decreases in the DCE-MRI or the RAMRIS disease activity scores from 0 to 12 months. The sample size in the DCE-MRI cohort was very small and only two patients had clinical involvement of the hand at baseline. Nevertheless, DCE-MRI and RAMRIS disease activity measures were highly correlated. The correlation coefficients between RAMRIS synovitis and Nvoxel scores were similar to those found in a previous study using the same computer-aided method for DCE-MRI analysis and a 0.2 T MRI unit.22 The pronounced treatment-induced changes in DCE-MRI parameters and the high reproducibility found suggest that further and larger studies of DCE-MRI as outcome measure in clinical trials would be useful.
In this study, the intrareader agreement for scores of inflammatory parameters in conventional MRI was similar to that previously reported, but slightly lower for the structural damage scores.10 ,11 ,23 However, in our study the reader was blinded to the order of the images, and also, the patients had low disease activity and almost no structural damage progression in the 12-months’ follow-up, neither radiographically nor as assessed by MRI, which probably explains the lower intrareader agreement for structural damage change scores.
This study has some limitations. Radiographic and MRI findings were scored blinded to chronology, whereas clinical outcomes were not, which might bias clinical assessment towards higher treatment responses. The MRI was carried out with four different MRI units, with different field strengths, and this might have affected the MRI reads. The sample size was relatively small and minimal structural progression was seen, which may be one explanation for the absence of any statistically significant difference between the two treatment groups. Furthermore, we cannot rule out the possibility that there was some selection bias, as the patients who did not enter the MRI substudy had higher disease activity than those who did participate.
In conclusion, in this randomised double-blind trial, we found that a treat-to-target strategy with methotrexate and intra-articular glucocorticosteroid, with or without adalimumab, effectively decreased MRI disease activity in patients with ERA, and no MRI structural damage progression was found after 1-year of follow-up. The findings suggest that addition of adalimumab was associated with further suppression of osteitis and tenosynovitis.
Acknowledgments
The authors would like to thank all participating patients and study nurses.
References
Footnotes
Handling editor Tore K Kvien
Correction notice This article has been corrected since it was published Online First. The spelling of the first author's name has been corrected to ‘Mette Bjørndal Axelsen.’
Collaborators OPERA (OPtimised treatment algorithm in Early Rheumatoid Arthritis) study group. Ole Slot: Department of Rheumatology and DANBIO, Glostrup Hospital; Faculty of Health Sciences, University of Copenhagen, Glostrup, Denmark. Lars Kjær Nielsen: Department of Rheumatology, Odense University Hospital, Svendborg, Denmark. Henrik Skjødt: Department of Rheumatology and DANBIO, Glostrup Hospital; Faculty of Health Sciences, University of Copenhagen, Glostrup, Denmark. Ole Majgaard: Department of Rheumatology, Slagelse Hospital, Denmark. Tove Lorenzen: Diagnostic Centre, Silkeborg Regional Hospital, Silkeborg, Denmark; Department of Medicine, Vejle Regional Hospital, Vejle, Denmark. Marcin Kowalski: Department of Rheumatology, Aarhus University Hospital, Denmark; Aalborg Hospital, Denmark. Inger Lauge Johansen: Department of Rheumatology, Viborg Regional Hospital, Viborg, Denmark. Peter Mosborg Pedersen: Department of Rheumatology, Randers Regional Hospital, Denmark. Natalia Manilo: Department of Rheumatology, Bispebjerg Hospital, Denmark, Henning Bliddal: Department of Rheumatology, Parker Institute, Frederiksberg Hospital, Denmark. Henrik Thomsen, Department of Diagnostic Radiology, Copenhagen University Hospital At Herlev, Denmark. Mikael Boesen, Department of Radiology, Bispebjerg and Frederiksberg Hospital, Olga Kubassova, Image Analysis, London, England.
Contributors The study was designed by the OPERA study group and all data were collected by the group. All the investigators contributed to the design, analysis and writing of the report. MBA and MØ were the principal investigators.
Funding This study was supported by an unrestricted grant from AbbVie, Denmark. AbbVie was not involved in the study set-up, data collection, analysis or interpretation, and had no influence on the publication of data.
Competing interests KH-P: UCB Nordic (less than US$10 000); Abbott (unrestricted grant for the OPERA study). MLH: Abbott, Centocor, Roche, Wyeth/Pfizer (less than US$10 000 each); The Danish Rheumatism Association: several research grants after evaluation. PJ: the Danish Rheumatism Association: Several research grants after evaluation. JP: Abbott, Bristol-Myers Squibb, MerckSharpDohme (less than US$10 000). HL: MerckSharpDohme, Roche, Bristol-Myers Squibb and Abbott (less than US$10 000 each). AS: MerckSharpDohme, Roche, Wyeth/Pfizer (less than US$10 000 each). HCH: Abbott (less than US$10 000). MØ: Abbott, Amgen, Bristol-Myers Squibb, Centocor, Genmab, GlaxoSmithKline, MerckSharpDohme, Novo, Wyeth/Pfizer, Roche, Schering–Plough and UCB (less than US$10 000 each); the Danish Rheumatism Association: several research grants after evaluation. KS-P: Abbott (unrestricted grant for the OPERA study), Wyeth/Pfizer and Roche (less than US$10 000 each); the Danish Rheumatism Association: several research grants after evaluation.
Patient consent Obtained.
Ethics approval Regional ethics committee, Denmark (VEK-20070008).
Provenance and peer review Not commissioned; externally peer reviewed.