Article Text

Abstract
Objective To assess the effectiveness of switching to a second tumour necrosis factor inhibitor (TNFi) in patients with ankylosing spondylitis (AS).
Methods Data were extracted from an ongoing longitudinal observational multicentre study in Norway. This study included anti-TNF naïve patients with AS starting treatment with a TNFi as well as treatment with a second TNFi in these same patients. Effectiveness data and 2-year drug survival were compared between switchers and non-switchers and within switchers (first and second TNFi).
Results 514 anti-TNF naïve patients with AS were included; 77 patients switched to a second TNFi while 437 patients did not switch. The percentages of non-switchers using etanercept, infliximab or adalimumab were 53%, 32% and 15%, and the percentages of first and second TNFi in the switchers were 42%, 53% and 5% and 40%, 23% and 36%, respectively. The reason for switching was insufficient response (IR) in 30, adverse events (AEs) in 44 and not reported in 3 patients. Baseline disease activity was similar between the groups. Three-month BASDAI 50 and ASAS 40 responses were achieved by 49% and 38% of non-switchers, by 25% and 30% of switchers after the first TNFi and by 28% and 31% after the second TNFi. The 3-month disease activity level was higher for switchers on the second TNFi than for non-switchers. Drug withdrawal rate was higher during the second TNFi among switchers than for non-switchers (p=0.001). No difference was found in the effectiveness of the second TNFi between switchers due to IR and AE.
Conclusion This study confirms that switching to a second TNFi can be effective in AS and can be as useful as in rheumatoid arthritis, although overall effectiveness seems to be somewhat lower than in non-switchers.
Statistics from Altmetric.com
Inhibitors of tumour necrosis factor α (TNFα) have constituted a major advance in the treatment of ankylosing spondylitis (AS), and infliximab, etanercept, adalimumab and golimumab have all been proved to be efficacious in reducing signs and symptoms of AS.1,–,4 However, some patients fail to respond to treatment and others may experience adverse events (AEs) necessitating treatment discontinuation. The three TNF inhibitors (TNFi) which have been commercially available until recently have a different chemical structure, half-life and administration, and also somewhat different mechanisms of actions.5 This gives support to the idea that lack of efficacy or AEs after treatment with one TNFi do not preclude successful treatment with one of the other available drugs.
The efficacy of switching to a second TNFi after failing a first TNFi has been widely studied in rheumatoid arthritis (RA).6,–,15 Results from these and other observational studies show that switching can benefit some patients.16 A pilot open-label randomised controlled trial (RCT) in patients with an incomplete response to etanercept found superior efficacy of switching to in-fliximab versus continuation of etanercept.17 A recently published consensus statement suggests that switching between TNFi may be a worthwhile approach in RA.18
The efficacy of switching between TNFi in AS has been examined in a limited number of studies including fewer than 25 patients who switched.19,–,24 However, 326 of the 1250 patients with AS (26.1%) included in a 12-week open-label adalimumab study had been previously treated with etanercept and/or infliximab, and response rates were lower in these patients than in the TNF naïve patients.25 26 The recommendations for management of AS have so far not specifically addressed switching between TNFi.27,–,29
The objective of this study was to assess the effectiveness of switching to a second TNFi in patients who had discontinued the first TNFi due to insufficient response (IR) or AEs. We also determined whether there was a relationship between the reason for switching and the subsequent effectiveness of the second TNFi and reason for discontinuation of the second TNFi.
Methods
Setting
Since December 2000, adult patients (>18 years of age) with inflammatory arthropathies starting synthetic and biological disease-modifying antirheumatic drugs (DMARDs) in five Norwegian rheumatology departments have been included in the NOR-DMARD register. The study design is a prospective multicentre longitudinal observational study with assessments at baseline, after 3, 6 and 12 months and yearly thereafter. The completeness of the register has been approximately 85%; the remaining 15% were either missed for inclusion, refused enrolment or were excluded because of language barriers or inclusion in ongoing RCTs. By March 2009, 8849 treatment courses in 5896 individual patients had been included in the NOR-DMARD register (figure 1).

Overview of the NOR-DMARD register and selection of patients for the current study. *Number of patients for each type of TNFi switch. ADA, adalimumab; AS, ankylosing spondylitis; DMARDs, disease-modifying antirheumatic drugs; ETN, etanercept; IFX, infliximab; JIA, juvenile idiopathic arthritis; PsA, psoriatic arthritis; RA, rheumatoid arthritis; TNF, tumour necrosis factor; TNFi, TNF inhibitor; UA, undifferentiated arthritis.
Patients
TNFi naïve patients with AS enrolled in the NOR-DMARD register before March 2009 and starting treatment with a TNFi were selected for the current analyses. Follow-up data up to July 2009 were studied, including information about treatment with a second TNFi. Rheumatologists in the respective departments made the diagnosis of AS by clinical judgement (ie, International Statistical Classification of Diseases and Related Health Problems 10th Revision code M45).
Assessments
Scores from assessments at baseline and after 3 months of treatment were included in the analyses. Assessments included erythrocyte sedimentation rate, C reactive protein (CRP), 100 mm Visual Analogue Scale (VAS) for physician's assessment of global disease activity and patient's assessment of pain, fatigue and global disease activity (100 mm = worst disease activity, fatigue and pain, respectively), the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), the Bath Ankylosing Spondylitis Functional Index (BASFI) and the Medical Outcomes Study 36-item Short-Form Health Survey (SF-36).30,–,33 The SF-6D is a utility measure derived from the SF-36 with scores ranging from 0 (dead) to 1 (perfect health).34 The recently developed Ankylosing Spondylitits Disease Activity Score (ASDAS) was calculated from BASDAI questions 2, 3 and 6, as well as the patient global assessment and CRP.35 36 Proportions of patients achieving a BASDAI 50, Assessments of Spondyloarthritis International Society 20 (ASAS20) and ASAS40 responses as well as ASDAS Clinically Important Improvement (ΔASDAS ≥1.1) and ASDAS Major Improvement (ΔASDAS ≥2.0) were calculated.37 38 BASDAI and BASFI were included as assessment tools in 2006, and consequently these measures as well as ASDAS data and ASAS responses were not available for all patients. Information about date of and reason(s) for treatment termination was recorded in patients who discontinued treatment.
Statistical analyses
Continuous variables are presented as medians with IQR. For demographics and baseline disease measures the Mann–Whitney U test and χ2 test were used for comparison between groups of different patients, and the Wilcoxon signed rank test and McNemar test were used for comparisons within the group of switchers. Three-month response rates were compared by χ2 test and McNemar test as appropriate. For the comparison of 3-month disease status between non-switchers and switchers' second TNFi, we performed analysis of covariance (ANCOVA) with the van der Waerden normal scores of each disease measure as dependent variables, adjusting for the van der Waerden normal scores of the respective baseline values (ie, ranked ANCOVA). We applied mixed modelling analysis to handle the lack of independence in the data when comparing the switchers' first TNFi regimen with the switchers' second TNFi regimen, and we fitted subject-specific (random intercept) models with the van der Waerden normal scores of the 3-month disease measures as the dependent variables, the respective van der Waerden normal scores of the baseline measures as covariates and the treatment number (first or second TNFi) as a factor. Continuation of treatment (‘drug survival’) was compared by Kaplan–Meier analysis, and the main survival analysis was based on 0–2 years follow-up. Variables associated with discontinuation of the first TNFi were assessed by Cox regression analysis.
Statistical tests were two-sided with level of significance set at 0.05 without correction for multiple comparisons. Statistical analyses were performed using SPSS Version 15.0 (SPSS, Chicago, Illinois, USA).
Results
Demographics and medication
A total of 514 patients treated with their first TNFi were identified, 77 of whom switched to a second TNFi after discontinuing the first. The remaining 437 patients are referred to as ‘non-switchers’. Demographics and medication were similar between the groups (table 1). Adalimumab constituted a higher percentage among the second TNFi than among the first. Synthetic DMARD co-medication, which was given in a minority of cases (23% overall), was mainly methotrexate (80%) and was more commonly given to patients treated with infliximab. Etanercept was given as subcutaneous injections 25 mg twice a week or 50 mg once a week. Infliximab was given as intravenous infusions at weeks 0, 2, 6 and then every 6–8 weeks, with a mean dose ranging from 4 to 5 mg/kg. Adalimumab was given as subcutaneous injections 40 mg every other week.
Demographics and disease characteristics at start of TNFi therapy
The reason for switching to a second TNFi was AEs in 44 patients (most frequently skin reactions related to injections or infusions or drug-related systemic symptoms), IR in 30 patients and not reported in the remaining 3 patients. The switchers were treated with the first TNFi for a median of 266 days (range 1–1392), and the second TNFi was started at a median of 77 days (range 0–1608) after discontinuation of the first TNFi.
Baseline disease characteristics
Baseline median values for various disease activity and health-related quality of life (HRQoL) measures were similar at the start of the first TNFi for the non-switchers and switchers, and also for the switchers when they started their second TNFi (table 1). BASDAI, BASFI and related data were available in 58% of the non-switchers, 39% of the switchers for the first TNFi regimen and 75% for the second TNFi regimen.
Three-month responses and disease status
Tables 2 and 3 show the 3-month responses and health status for the non-switchers and for switchers before and after switching TNFi. For the first TNFi treatment course of the switchers, we have also included information recorded at the last study visit during treatment (range 3 months to 4 years); these responses and states were generally inferior to the 3-month responses and states within the group (tables 2 and 3). The effectiveness of the first TNFi in the switchers is further detailed in table 1 in the online supplement, which shows response rates and disease activity on the first TNFi in the switchers categorised according to the reason for terminating it. The indication of loss of response seemed to be clearer for the IR switchers.
Response rates*
Disease states on treatment
After 3 months of treatment with the second TNFi, BASDAI 50, ASAS20 and ASAS40 responses were achieved by 28%, 40% and 30%, respectively (table 2). Three-month response rates and disease states were compared between the non-switchers and the second TNFi of the switchers, as well as between the first and second TNFi regimen within switchers. The non-switchers had a higher BASDAI 50 response rate (table 2) and, on a group level, lower disease activity and better HRQoL (table 3). There was no clear difference between first and second TNFi within switchers. Adjusting for disease duration in these analyses did not influence the results (data not shown). Three-month changes from baseline are shown in table 2 in the online supplement. The changes in non-switchers were superior to those in switchers receiving the second TNFi, and the statistical significance of these differences was accentuated when adjustments for baseline differences were performed (see table 2 in online supplement).
Efficacy of second TNFi according to reason for switching
IR switchers had been treated with the first TNFi (etanercept n=15, infliximab n=14, adalimumab n=1) for a median of 294 days (range 56–1392) and started the second TNFi 32 days (range 0–1608) after discontinuation of the first TNFi. For AE switchers, treatment time with the first TNFi (etanercept n=17, infliximab n=25, adalimumab n=2) was somewhat shorter (median 171 days (range 1–1211)), while time between treatments was 119 days (range 0–1468). For the IR switchers, the second TNFi was etanercept in 11 (36.7%), infliximab in 8 (26.7%) and adalimumab in 11 (36.7%) patients, and for the AE switchers the second TNFi was etanercept in 19 (43.2%), in-fliximab in 10 (22.7%) and adalimumab in 15 (34.1%) patients. Baseline disease activity was similar for the IR switchers and the AE switchers, and 3-month responses and disease states were also similar (table 4).
Baseline and 3-month disease states and response rates of the second TNFi according to reason for switching
Retention to therapy
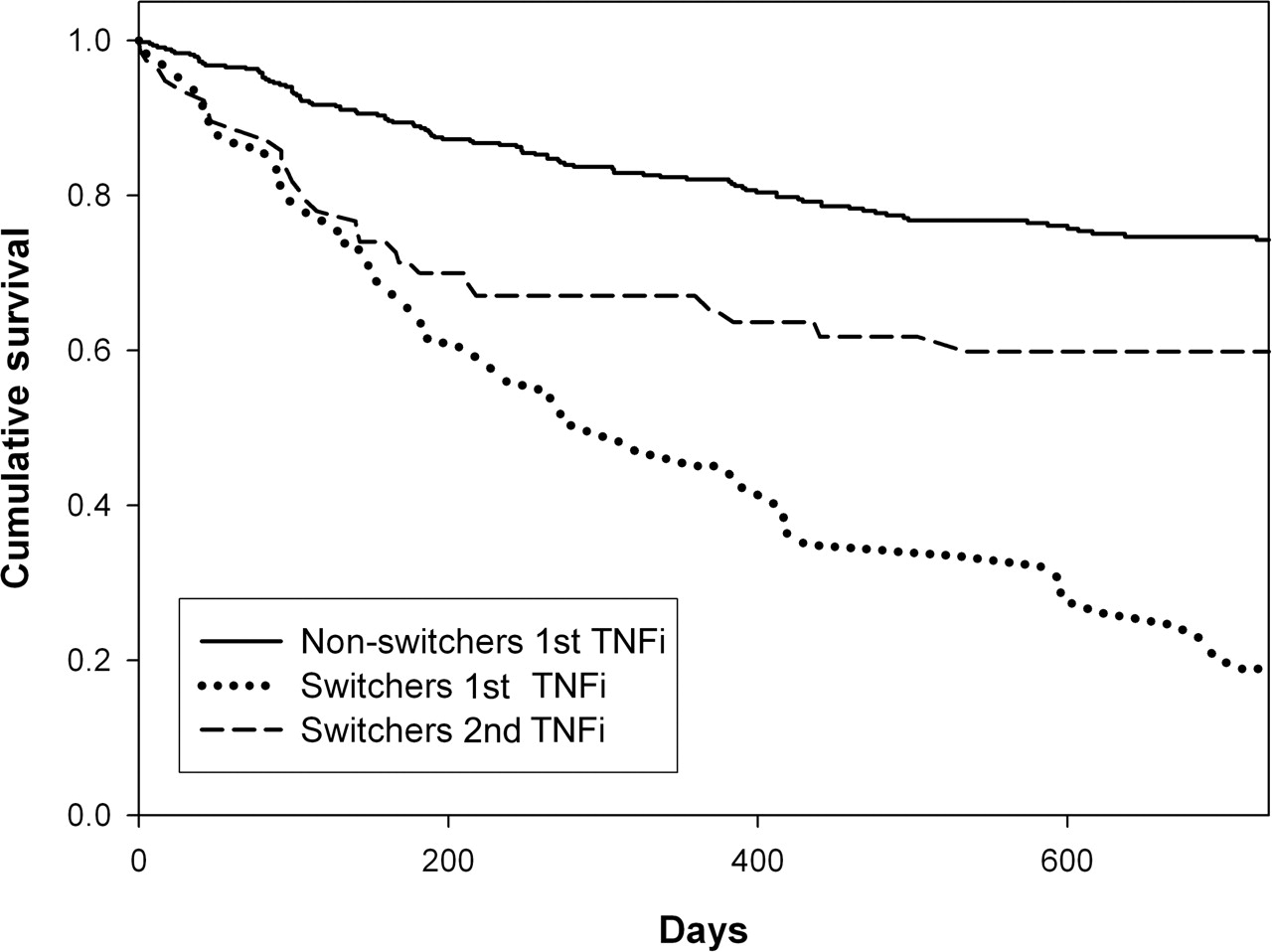
Retention to therapy was superior for non-switchers compared with switchers' second TNFi (log rank test p=0.001, figure 2). For the first TNFi, overall 1- and 2-year drug survival rates were 76% and 65%, respectively, compared with 67% and 60% for the second TNFi. Baseline fatigue VAS was the single statistically significant predictor of discontinuation of the first TNFi (HR 1.08, 95% CI 1.02 to 1.15 per 10 mm increase; p=0.007) adjusted for age and sex. We also stratified the second TNFi group according to the reason for switching and found somewhat better drug survival among the IR switchers than the AE switchers (p=0.27).
{kind=link}
{kind=link}
Crude 2-year retention to tumour necrosis factor inhibitor (TNFi) therapy (Kaplan–Meier analysis; log rank test p=0.001 for non-switchers vs switchers' second TNFi; log rank test p<0.001 for non-switchers vs switchers' first TNFi). Numbers of patients in the study were 437/77/77 at baseline, 411/64/67 at 3 months, 375/47/51 at 6 months, 294/32/40 at 12 months and 189/13/22 at 24 months for non-switchers, switchers' first TNFi and switchers' second TNFi, respectively.
At July 2009, 37 (48%) of the 77 switchers were still on their second TNFi for a median 673 days (range 159–1644), 8 patients (10%) were lost to follow-up (most patients had moved to another region), while 32 patients (42%) had discontinued their second TNFi after a median 112 days (range 1–1472). Nineteen patients discontinued the second TNFi because of IR, 12 because of AEs (mostly skin reactions) and 1 because of patient preference. We could not demonstrate a clear relationship between reasons for discontinuing first and second TNFi: Among the 45 AE switchers, 13 patients discontinued the second TNFi because of IR (29.5%), 8 because of AEs (18.2%) and 1 because of patient preference (2.3%) while, among the 30 IR switchers, 5 patients (16.7%) discontinued the second TNFi because of IR and 4 (13.3%) because of AEs (p=0.77, χ2 test).
Discussion
In this study we found that switching to a second TNFi could benefit some patients and up to one-third of patients showed a good response. However, disease activity and health status 3 months after initiation of treatment were generally worse for switchers on their second TNFi than for non-switchers.
Only a few reports with detailed information about switching to a second TNFi in prospectively followed patients with AS have so far been published.19,–,21 However, one large study, the RHAPSODY study, provides information about efficacy of the second TNFi in AS.25 In this study, 1250 patients with active AS, of whom 326 patients had previously been treated with etanercept and/or infliximab, were treated with adalimumab for 12 weeks. Anti-TNF naïve patients achieved greater treatment responses than patients previously exposed to TNFi (BASDAI 50: 63% vs 41%; ASAS40: 59% vs 38%), and TNF naïvety was also found to be an independent predictor of treatment response.25 Other studies addressing the topic of switching TNFi in AS have included 7–23 switching patients.19,–,21 23 24 The mode of reporting responses in these studies was heterogeneous, encumbering the summarisation of efficacy results but, in general, responses were comparable or somewhat superior to results from this study.19,–,21 23 24 In the present study the reason for switching to a second TNFi was more often AEs (n=44) than IR (n=30), and this observation is different from previous reports on switching between TNFi in AS.19 20 23 24
The decision to discontinue and switch in our study was made by the treating rheumatologist and was not standardised. Nonetheless, observational studies give valuable information about ‘real life’ effectiveness of treatment. One could argue that the threshold for IR might be different for the first and second agent, and also that the threshold might have changed over the years. The current study was not sufficiently powered to examine this issue further, neither did we have power to compare the effectiveness of switches between TNFi with different mechanisms of action. In RA it has been shown that switching from etanercept to infliximab or vice versa,8 11 12 17 39,–,41 as well as switching from both etanercept and infliximab to adalimumab,7 10 42 43 can be effective approaches.
Adalimumab was more often the second TNFi, which was expected as it was introduced at a later stage than the other two TNFi which have been available until now. Treatment decisions and the threshold for stopping therapy are related to factors other than efficacy and AEs—for example, access to other therapies and the expectations of patients as well as the physicians. Thus, the external validity of some of the findings, particularly ‘drug survival’, may be limited. In Norway there is generally good access to TNFi treatment for patients with AS who have active disease and in whom ‘conventional therapy’ (non-steroidal anti-inflammatory drugs) is insufficiently effective, and the costs are covered by the government.
There are several potential pitfalls when interpreting findings from observational studies of switching between TNFi.16 The disease activity of both AS and RA tends to fluctuate, whereas therapeutic interventions tend to be initiated at times of high disease activity and the improvement may be due to chance and not the intervention in itself. Also, the definition of ‘failure’ should ideally be more sophisticated than the dichotomisation ‘AEs’ and ‘lack of efficacy’. Lack of efficacy could mean primary lack of efficacy (ie, no response at all), a partial although not sufficient response as well as secondary loss of efficacy (eg, due to human anti-chimeric antibodies (HACA) or human anti-humanised antibodies). We chose the term ‘IR’ to cover all three of these possibilities. A study in RA indicated that adalimumab might be more effective in patients with a secondary loss of efficacy on infliximab (allegedly due to HACA) than patients with a primary lack of efficacy with infliximab or etanercept.10 A recent publication elaborating on the findings from the RHAPSODY study showed that 3-month response rates on adalimumab were higher in patients who had discontinued the prior TNFi (etanercept or infliximab) because of intolerance or loss of response than because of (primary) lack of response.26 Ideally, we would have differentiated between patients with a primary lack of efficacy on the first TNFi and patients with a secondary loss of efficacy in this study. However, this differentiation was not a part of the data collection and we could not easily make the distinction from the efficacy data. Furthermore, with only 30 patients switching because of IR, a division into primary lack and secondary loss of efficacy would result in very few patients in each group. However, the data in table 3 and in table 1 in the online supplement show that median disease activity was generally lower at 3 months than at last study visit. Even though this observation could be a result of naturally fluctuations in disease activity, the difference could also indicate that at least some patients experienced secondary loss of efficacy.
The most valid disease activity and response measures (BASDAI, ASDAS and ASAS responses) were not available for all patients as BASDAI and BASFI were not part of the data collection from the start of the NOR-DMARD study. The percentage of patients for whom these data were available was therefore particularly low for the first TNFi course of the switchers. This fact contributes to the potential power problems of this study, which included a limited number of TNFi switches.
In a recent study where 245 switchers with RA were divided into three groups according to reason for switch—namely, primary non-responders, secondary loss of response and AEs—the improvement in disease activity did not differ when correcting for baseline disease activity and corticosteroid use.14 However, patients who discontinued the first TNFi because of non-response or loss of response were more likely to discontinue the second TNFi because of IR, while the AE switchers more often discontinued the second TNFi for AEs. In another study on switching between TNFi in RA, the reasons for discontinuing the second TNFi was related to reasons for discontinuing the first TNFi.9 We could not demonstrate such a relationship in our study in AS.
In conclusion, this real-life study shows that switching to a second TNFi can be an effective approach in AS, with around one-third of patients showing a good clinical response and more than half of patients continuing the treatment for more than 2 years. A larger study, ideally an RCT, is needed to establish the efficacy of switching to a second TNFi.
Acknowledgments
The authors thank the patients for participating in this study, the local rheumatology staff for data collection and Inge C Olsen for helpful discussions regarding the statistical analyses.
References
Supplementary materials
Web Only Data
Files in this Data Supplement:
Footnotes
-
Funding The work was supported by Eastern Norway Regional Health Authority. The Norwegian disease-modifying antirheumatic drug study has received unrestricted grant support from Abbott, Amgen, Wyeth, Aventis, MSD, Schering-Plough/Centocor, BristolMyers Squibb, Roche and the Norwegian Directorate for Health and Social Affairs.
-
Ethics approval This study was conducted with the approval of the regional ethics committee and by the Data Inspectorate. Patients gave written informed consent before participation.
-
Competing interests The NOR-DMARD register is financially supported by pharmaceutical companies but the sponsors are not involved in the analyses and presentation of data. Most of the authors have received speaker and/or consultancy honoraria from companies marketing biological DMARDs. Johannes WJ Bijlsma was the handling editor for this manuscript.
-
Provenance and peer review Not commissioned; externally peer reviewed.