Article Text

Abstract
Objective Anticitrullinated protein antibodies (ACPA) are the most predictive factor for the development of rheumatoid arthritis (RA). Epitope spreading towards more citrullinated epitopes occurs before the onset of RA. Here, the authors investigated whether specific epitope recognition allows the identification of specific RA subgroups and whether it is associated with clinical features of RA.
Methods The reactivity of 661 patients with RA from the Leiden Early Arthritis Clinic against several citrullinated antigens was determined by ELISA. Cluster analyses were performed to identify subgroups of patients on the basis of their ACPA recognition profile. The association of the specific reactivities with clinical characteristics was studied.
Results ACPA-positive patients displayed a heterogeneous ACPA recognition profile. After performing cluster analyses, no apparent clustering of patients was found, and on the basis of the reactivities analysed, 64 different subgroups could already be identified. The extent of epitope recognition was associated with anticyclic citrullinated peptide-2 levels. The recognition of specific citrullinated epitopes was not associated with baseline characteristics. Likewise, patients with an extended fine specificity repertoire did not display differences in baseline characteristics or joint damage after 7 years of follow-up using cyclic citrullinated peptide-2 levels as a proxy, compared to ACPA-positive patients recognising fewer peptides.
Conclusion These data show that the ACPA response is highly diverse with respect to recognition of specific citrullinated epitopes. Furthermore, the authors' data indicate that clinical correlates in established ACPA-positive RA are independent from the specific (group of) citrullinated peptides recognised.
Statistics from Altmetric.com
Introduction
Anticitrullinated protein antibodies (ACPA) have been shown to be able to initiate and enhance arthritis in murine models of arthritis1 2 and are able to activate Fc Receptor-positive cells3 4 and the complement system, leading to the argument that they could play a role in disease pathogenesis.5 The detection of ACPA, which is most commonly assessed by reactivity against cyclic citrullinated peptide (CCP)-2, is an accepted diagnostic tool for rheumatoid arthritis (RA).6 ACPA are highly specific for RA, can be detected years before the first clinical manifestation of RA7 8 and are reported to be a good predictor for the development of RA.9 Anti-CCP antibodies recognise multiple citrullinated peptides and proteins and are thus a collection of ACPA.10 Some types of human leucocyte antigens (HLA) alleles, particularly HLA-DRB1 alleles encoding the shared epitope sequence, are known to be associated with RA susceptibility,11 more specifically susceptibility to ACPA-positive RA.12 ACPA-positive and ACPA-negative disease have been shown to be associated with different genetic and environmental risk factors, fuelling the hypothesis that different pathophysiological mechanisms are underlying these two separate disease subsets.13 14
Next to isotype usage15 and avidity,16 the fine specificity of an antibody response is also thought to contribute in determining its efficacy.17 It has been shown that ACPA can recognise a variety of citrullinated antigens, including citrullinated fibrinogen (cFib), α-enolase,18 citrullinated vimentin (cVim) and citrullinated myelin-binding protein (cMBP)—the latter mimicking the Sa antigen.19 20 Levels of specific ACPA are elevated in synovial fluid, suggesting local antibody production and/or retention of ACPA at the site of inflammation.21
However, not all ACPA-positive sera will recognise all citrullinated antigens, as has been shown by analysing the reactivity against different citrullinated peptide antigens.10 22
It has been shown that patients with RA display a much more extended citrullinated epitope recognition pattern compared to ACPA-positive first-degree relatives without symptoms.23 Indeed, epitope spreading with an increase in the recognition of citrullinated antigens occurs before the patients fulfil the 1987 classification criteria of RA. Differences in ACPA fine specificity between patients having undifferentiated arthritis who do or do not develop RA after 1 year are already present at baseline.24 Likewise, patients with arthralgia and with an extended ACPA repertoire have a higher risk of developing arthritis.25
It is conceivable that a certain ACPA recognition profile is associated with the emergence of certain clinical features and possibly pathogenicity, as has been shown in other autoimmune diseases. For example, in pemphigus the reactivity against different desmoglein epitopes is associated with different outcomes.26
Here, we determined the association between the ACPA fine specificity and phenotypic characteristics within ACPA-positive RA and investigated whether specific subsets of RA patients can be distinguished on the basis of their epitope recognition profile.
Materials and methods
Patient population
All patients who fulfilled the American College of Rheumatology 1987 revised criteria for the classification of RA27 within 1 year of follow-up from the Leiden Early Arthritis Clinic were analysed (n=661). The Leiden Early Arthritis Clinic is an inception cohort of patients with recent onset arthritis (symptoms duration, <2 years) that was started at the Department of Rheumatology of the Leiden University Medical Center in 1993 and was described in detail previously.28 Sustained disease-modifying antirheumatic drug (DMARD)-free remission was defined as having no current use of DMARDs, no swollen joints and classification as DMARD-free remission by the patients' rheumatologist.29
Anti-CCP2 assays
Total IgG anti-CCP2 was measured in baseline sera by ELISA (Immunoscan RA Mark 2; Eurodiagnostica, Arnhem, The Netherlands). Samples with a value >25 units/ml were considered positive according to the manufacturer's instructions. Individuals with antibodies against CCP2 were considered ACPA-positive. From patients with antibody levels reaching the plateau of the standard, we further diluted the serum to determine ACPA levels.
ACPA fine specificity assays
ELISA assays were developed, as previously described,30 against peptides derived from cVim, cFib and citrullinated α-enolase (cEno)5-20. Antibody reactivity against the citrullinated (Cit) and the uncitrullinated form of two linear peptides derived from vimentin (Vim 1-16: STCitS VSSS SYCitCit MFGG and Vim 59-74: VYAT CitSSA VCitLCit SSVP), two linear peptides derived from fibrinogen (Fibα 27-43: FLAE GGGV Cit GPR VVER H and Fibβ 36-52: NEEG FFSA CitGHR PLDK K) and one linear peptide derived from α-enolase (Eno 5-20: KIHA CitEIF DSCitG NPTV) were determined by ELISA as described previously23 31 Citrullination of myelin basic protein (MBP) (Sigma-Aldrich, Zwijndrecht, Netherlands) and the specific ELISA were performed as previously described.20 Antibodies reactive with citrullinated MBP were determined in 1:100 diluted sera.
Although there are also other targets for ACPA,32 33 we chose primarily to investigate epitopes from these proteins because they have been most consistently identified as citrullinated autoantigens.18 19 34 We analysed reactivity to citrullinated MBP, as its ELISA has been previously standardised to be the clinical equivalent (positive versus negative) of the original anti-Sa (cit-Vimentin) western blot assay.20
Cut-off values for the citrulline-specific responses were calculated as previously described.24 31 IgM-rheumatoid factor (RF), anti-CCP3 autoantibodies (IgA and IgG subforms) and anti-mutated citrullinated vimentin (MCV) autoantibodies were also measured by ELISA as described previously.31 Sera were tested for antinuclear factor (ANF) using indirect immunofluorescence at a 1:40 dilution on Hep-2000 cells (biomedical diagnostics).
Statistical analysis
Differences between groups were analysed with the Mann–Whitney test or the t test, or χ2 test where appropriate. Association between anti-CCP2 antibody levels and number of peptides recognised was studied by linear regression of log-transformed anti-CCP2 antibody levels on number of recognised peptides. Principal component analyses (PCA)35 were applied to covariance matrices and included the different fine specificity epitopes. In order to normalise distributions, all variables were log-transformed concentration levels plus one. Based on scree plots and eigenvalues, components with an eigenvalue ≥0.4 were selected.
The association of the specific reactivities with baseline characteristics and joint damage over time was studied. Annual radiographs of hands and feet were assessed chronologically for radiographic damage according to the Sharp–van der Heijde score 36 by one experienced reader. For this, a repeated measurement analysis was applied. This method takes advantage of the longitudinal, repetitive character of the data and does not exclude patients with incomplete follow-up data, avoiding selection bias. In a multivariate normal regression model with radiological score as response variable, the effect of time was entered as factor to fit the non-linear slope of joint destruction. The components were entered with an interaction term with time as continuous variable to test the effect of the components over time. Age, gender and inclusion period (a proxy for treatment strategy) were entered in the model to correct for possible confounding effects. Analyses were performed using SPSS version 17.0, and p values below 0.05 were considered to be statistically significant.
Cluster analyses were used to identify subgroups of patients on the basis of their ACPA recognition profile. Clustering illustrates the relationship between different patients and reactivities, as described by Eisen et al.37 Hierarchical clustering was performed using average linkage clustering where patient correlation was performed centred and the reactivities uncentred. To illustrate the influence on anti-CCP2 level, we performed a supervised cluster analysis where the patients were fixed and the reactivities correlated uncentred.
Results
ACPA recognition profile
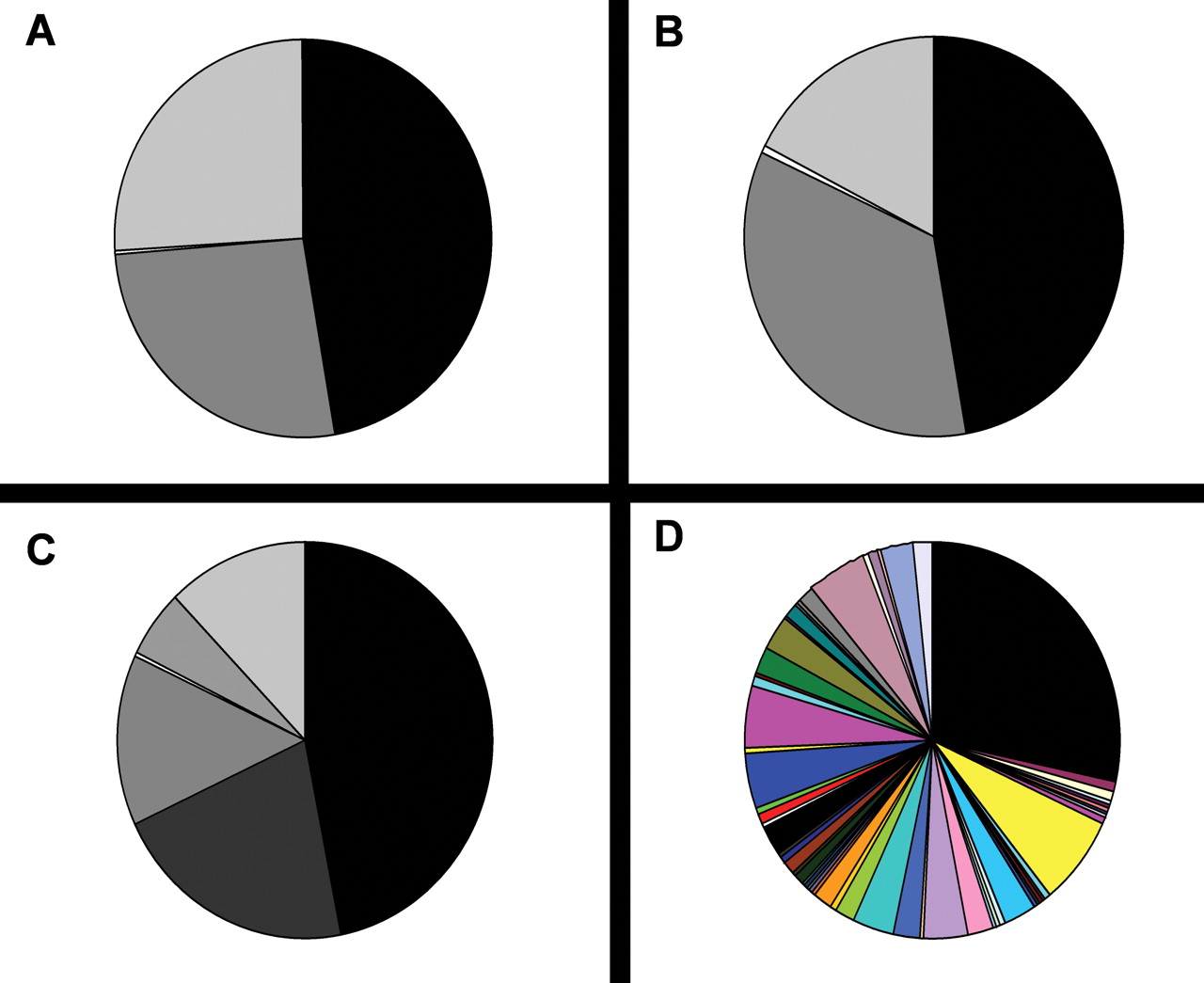
Baseline characteristics of the 661 patients with RA who fulfil the American College of Rheumatology criteria 1987 are shown in table 1. To analyse whether the ACPA recognition profile would allow for the identification of specific antibody positive subgroups, we wished to perform cluster analyses as well as PCA to investigate whether specific subgroups can be identified on the basis of epitope recognition. If so, such subgroups could then be used to analyse possible clinical association. First, we described patients on the basis of their ACPA status and their ability to recognise one specific citrullinated peptide (ie, cVim59-74 and cEno5-20). This analysis resulted in the identification of different subsets of patients (figure 1A,B). Combining the two reactivities against these two peptides resulted in more different subgroups (figure 1C). Remarkably, when using all nine reactivities included in this study, 64 subgroups could already be identified (figure 1D).

Different subsets of patients based on the epitope recognition profile. Patients were grouped on the basis of recognition of CCP2 and cVim59-74 (depicted in black are patients CCP2-cVim-; in white, CCP2-cVim+; in light grey, CCP2+cVim-; and in dark grey, CCP2+cVim+ (figure 1A)), grouped on the basis of recognition of CCP2 in cEno5-20 (depicted in black are patients CCP2-cEno-; in white, CCP2-cEno+; in light grey, CCP2+cVim-;and in dark grey, CCP2+cEno+ (figure 1B)) and on the combination of those two peptides (cVim59-74 and cEno5-20) and CCP2 (figure 1C). Dividing patients based on all tested reactivities (including cVim1-16, cVim59-74, cFibα27-43, cFibβ36-52, cEno5-20, MBP, MCV, mutated citrullinated vimentin; CCP2 and CCP3 resulted in 64 different subsets of patients, indicating a heterogeneous epitope recognition pattern. Depicted in black are patients negative for all the tested citrullinated antigens (figure 1D). CCP, cyclic citrullinated peptide; cEno, citrullinated α-enolase; cVim, citrullinated vimentin; cFib, citrullinated fibrinogen; MBP; myelin-binding protein.
Baseline characteristics
These data show that within ACPA-positive patients, a large heterogeneity is present in the ACPA recognition profile. More importantly, this large heterogeneity seems to preclude the identification of specific subgroups. To investigate the possibility that specific peptide reactivities would cluster together, we generated a heatmap after an unsupervised hierarchical cluster analysis. A heatmap groups patients who resemble each other the most, based on their fine specificity recognition repertoire. This analysis did not lead to the identification of apparent subgroups of patients harbouring a specific ACPA recognition profile (supplementary figure 1). Together, these analyses did not point to the presence of a clear pattern of recognition of citrullinated peptides by ACPA.
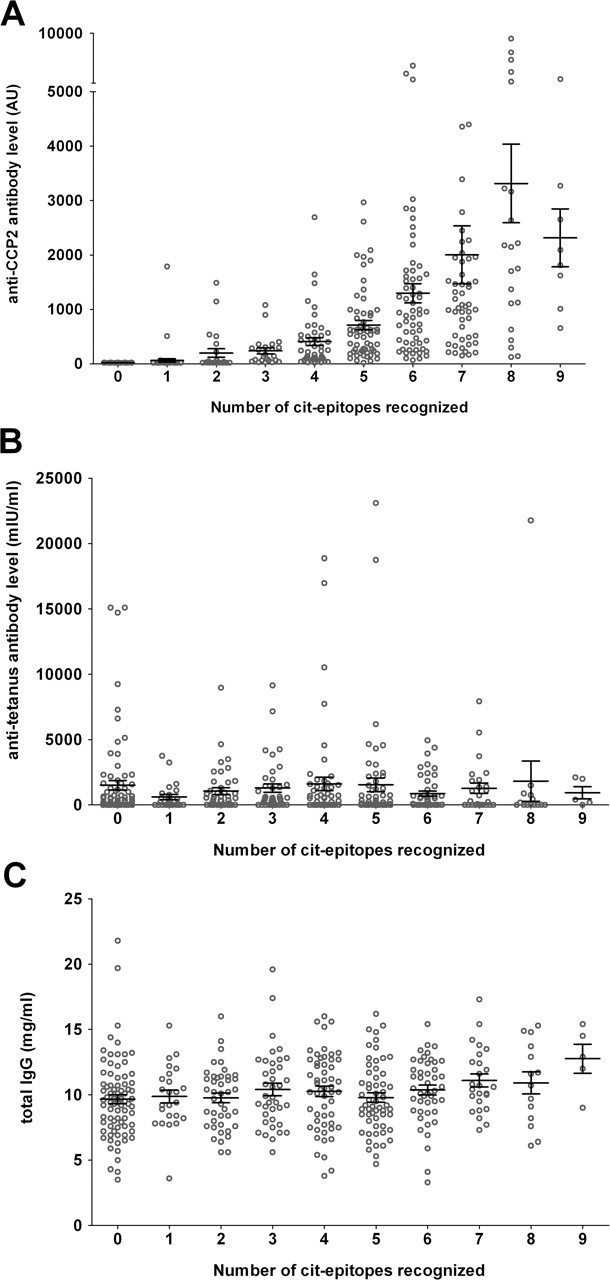
Interestingly, when we performed a similar analysis in a supervised manner by ordering patients on anti-CCP2 levels and subsequently analysed the recognition to specific peptides, an association was found between levels of anti-CCP2 antibodies and the number of recognised peptides by ACPA-positive patients with RA (figure 2). The association between levels and the epitope recognition profile was also confirmed with a linear regression analysis (p<0.001). As control, the relation to RF or ANF status (figure 2) was also analysed. In this case, no relation between anti-CCP2 levels and the antibody status of RF and ANF was found. Likewise, no association was found between the presence of antibodies against citrullinated epitopes and antibody levels against tetanus (figure 3B) or total IgG levels (figure 3C). Together, these data indicate that anti-CCP2 antibody levels specifically correlate with the number of citrullinated epitopes recognised by ACPA (figure 3A).

The association between anti CCP2 levels and the recognition of multiple citrullinated epitopes. A supervised cluster analysis showed an association between the anti-CCP2 levels and number of recognised peptides (including cVim1-16, cFibα27-43, cEno5-20, cVim59-74, cMBP, cFibβ36-52, CCP3 and MCV, mutated citrullinated vimentin). There was no apparent association between levels and RF or ANF. Each column represents one patient, and each row, one tested fine specificity peptide or protein. Depicted in red are patients being positive for the recognition of a specific reactivity; depicted in green are the patients who did not recognise that epitope. Depicted in grey are missing values. ANF, antinuclear factor; cEno, citrullinated α-enolase; CCP, cyclic citrullinated peptide; cFib, citrullinated fibrinogen; cVim, citrullinated vimentin; RF, rheumatoid factor.

Association between CCP2 level and number of citrullinated epitopes recognised. The number of epitopes recognised was positively associated with the anti-CCP2 levels (figure 3A). This association is citrulline-specific rather than antibody-level-specific, as it was not found for antitetanus antibody levels (figure 3B). Also, total-IgG levels were not associated with the number of epitopes recognised by patients with RA (figure 3C). Graphs are depicted with mean±SEM. Epitopes included in these analyses were cVim1-16, cVim59-74, cFibα27-43, cFibβ36-52, cEno5-20, cMBP, MCV, mutated citrullinated vimentin; CCP2 and CCP3. CCP, cyclic citrullinated peptide; cEno, citrullinated α-enolase; cFib, citrullinated fibrinogen; cMBP, citrullinated myelin-binding protein; cVim, citrullinated vimentin; RA, rheumatoid arthritis.
As our analyses described above did not identify defined subgroups, we performed PCA thereafter. PCA are an exploratory tool to unravel unknown trends in the data; however, this method also did not provide indications for the presence of patient subsets that can be grouped on the basis of the ACPA recognition profile (data not shown). Together, these analyses show that within these reactivities, no apparent patterns of recognition of citrullinated peptides by ACPA are present.
ACPA fine specificity and clinical characteristics
As outlined above, no specific subgroups of patients could be identified based on the presence of different ACPA characteristics. Therefore, we wished to analyse associations between baseline characteristics and the recognition of specific epitopes. To determine whether the baseline characteristics are associated with the recognition of specific citrullinated epitopes, we performed these analyses in the ACPA-positive stratum only. In doing so, we control the possibility that the results described above are explained by the known association between baseline characteristics and ACPA status, rather than by an influence of specific epitope recognition on baseline characteristics (ie, all ACPA reactivities are almost exclusively found within the ACPA-positive stratum). We observed essentially no association with any of the reactivities in relation to any of the baseline characteristics tested (figure 4 and supplementary figure 2). Although an association between reactivity against anti-cMBP-reactivity and C reactive protein (CRP) was observed (p=0.008), this association did not remain after the Bonferroni correction for multiple testing (figure 4). In line with these data, patients with an extended fine specificity repertoire (defined by the recognition of more than two citrullinated epitopes) also did not display significant differences in baseline characteristics compared to ACPA-positive patients recognising fewer peptides (figure 4), as the difference in CRP levels (p=0.018) could not withstand correction for multiple testing.
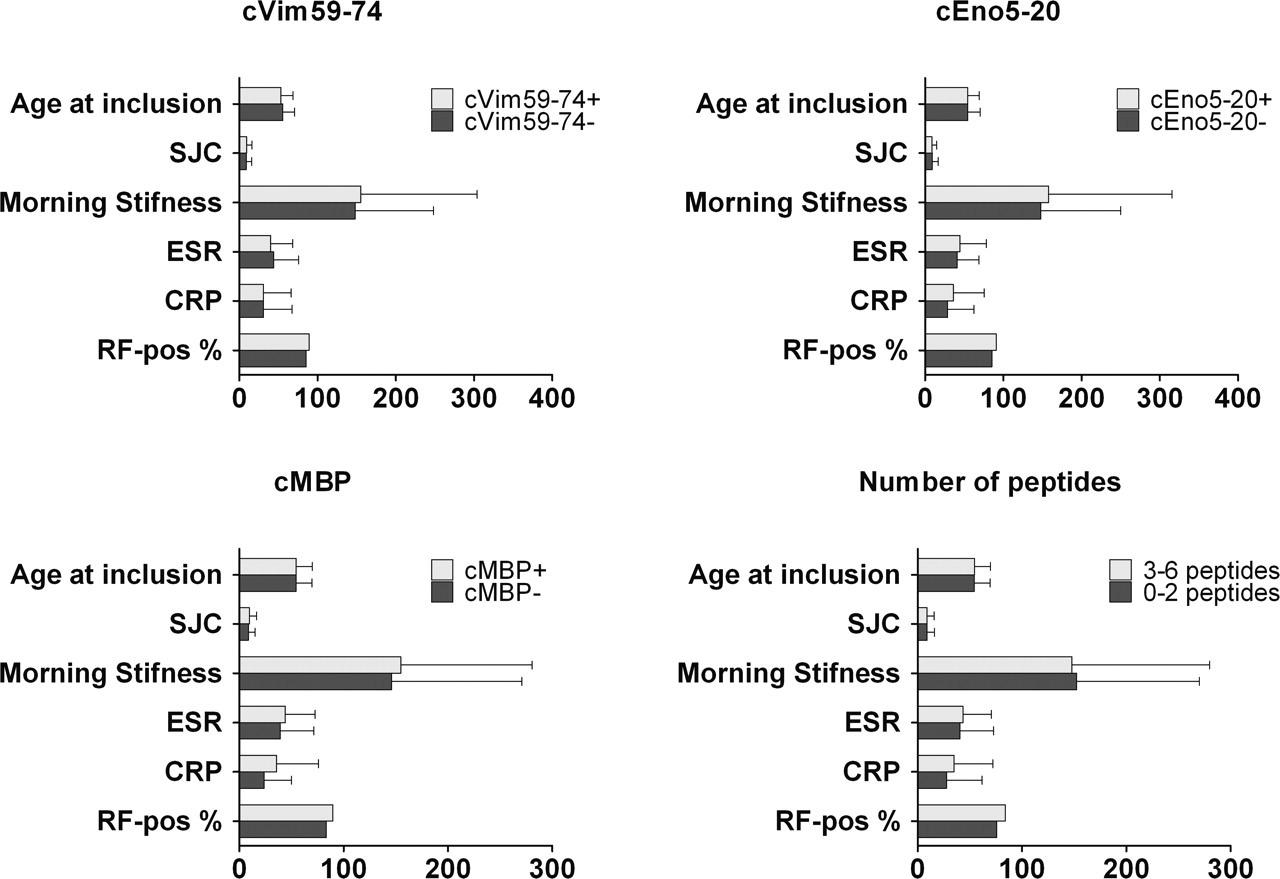
The association between epitope recognition and baseline characteristics. We observed essentially no association with any of the reactivities in relation to any of the baseline characteristics tested. An association was found between the recognition of cMBP and higher CRP levels at baseline (p=0.008) and recognition of more citrullinated peptides with CRP levels (p=0.018). However, after correction for multiple testing, no association between the recognition of specific citrullinated epitopes and baseline characteristics remained. Depicted are the mean and the SD between different citrullinated epitopes and baseline characteristics within ACPA-positive patients. Age of inclusion is depicted in years, swollen joint count with number of swollen joints, morning stiffness in min, ESR in mm/h, CRP in mg/l and RF in percentage positivity. ACPA, anticitrullinated protein antibodies; cMBP, citrullinated myelin-binding protein; CRP, C reactive protein; ESR, erythrocyte sedimentation rate; RF, rheumatoid factor; SJC, swollen joint count.
Another goal for making subgroups is to identify patients who will reach remission or will develop more joint destruction over time. Therefore, we wished to analyse sustained DMARD-free remission and joint damage over time within the ACPA-positive stratum. Only nine out of 306 ACPA-positive patients with RA achieved remission. As a consequence of this low number of patients, we did not perform further analyses into the association of the ACPA recognition profile and remission. Recently, we have shown that different fine specificities or an extended ACPA recognition profile was not associated with joint destruction over time.38 We now extended these findings by analysing additional citrullinated epitopes, but this analysis also did not indicate an association between the recognition of a specific citrullinated epitope with radiological progression. Nonetheless, it is possible that an association exists for another, not in our study tested, epitope. Our data show a strong correlation between anti-CCP2 levels and the number of peptides recognised by patients (figures 2 and 3). Therefore, we wished to use anti-CCP2 levels as a proxy for the peptides that we did not analyse. Intriguingly, we did not observe an association between rate of joint destruction over time and the anti-CCP2 levels within the ACPA-positive patients (p=0.66) (figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Rate of joint destruction over time and anti-CCP2 levels. Anti-CCP2 positive patients developed significantly more joint destruction over time (p <0.001) compared to anti-CCP2-negative patients. Within the anti-CCP2-positive patients the rate of joint destruction between patient with high levels (>620 arbitrary units (AU)) and low levels (<620AU) did not differ (p=0.66). The ACPA-positive patients were divided into two groups based on the median of 620 AU. ACPA, anticitrullinated protein antibodies; CCP, cyclic citrullinated peptide.
Together, our data indicate that although the ACPA recognition profile is highly diverse, the number of epitopes recognised correlates with ACPA level. Interestingly, the recognition of these citrullinated peptides, irrespective of their differences in peptide-backbone structure, all correlated with similar clinical characteristics.
Discussion
Epitope spreading is a phenomenon in which the (auto)immune response is extended to include new epitopes within the same molecule or towards different molecules and is thought to be involved in disease onset of autoimmune disorders. For example, pemphigus is one of the most clearly defined autoimmune diseases mediated by autoantibodies. The involvement of epitope spreading in pemphigus pathogenesis was first demonstrated in endemic pemphigus foliaceous.26 Subjects in the preclinical stage harbour antibodies recognising different epitopes on desmoglein 1 compared to patients after disease onset.39 In several cases of pemphigus, it has been described that intermolecular epitope shifting occurs along with the transition of pemphigus phenotype.
In RA, the association between epitope spreading in a predisease phase with RA development had been described as well. For example, it has been shown that epitope spreading of the ACPA response occurs before clinical disease onset and that it is associated with the disease course of early arthritis.23 Likewise, at time of disease onset, ACPA-positive patients with undifferentiated arthritis who will subsequently develop RA and those that will not already have an immunological distinct immune response, although these differences were not confined to specific citrullinated epitopes. The relevance of epitope spreading before disease onset raised the question as to whether a different epitope recognition pattern would be associated with different clinical phenotypes as has been described in pemphigus. This question was also based upon the findings that HLA shared epitope alleles predispose for the development of antibodies against some but not for other citrullinated epitopes, suggesting that reactivity towards some epitopes plays a more relevant role than others in disease pathogenesis.30 40 41
Here, we investigated whether specific subsets of RA patients could be distinguished on the basis of an autoimmune response to specific citrullinated epitopes and investigated the effects of the ACPA fine specificity on clinical features of RA. The analyses were performed within the ACPA-positive stratum to exclude the influence of ACPA status on disease outcome, as published before.42
As subgrouping patients based on their epitope recognition profile could be potentially useful to get more homogenous patient groups, we analysed different recognition profiles in detail. Unsupervised clustering of patients based on their epitope recognition resulted in many different subgroups, making it unrealistic to analyse all those subgroups in detail. Therefore we analysed the data with the use of several methods to obtain indications as to whether specific patient groups can be formed based upon the (cumulative) occurrence of specific antibody reactivities. The PCA did not point to specific reactivities as a discriminative factor within the variables. Likewise, the cluster analysis also did not result in clustering of specific patients. These data suggest that the recognition profile of patients with RA displays a large heterogeneity and that patients are not characterised by a unique and specific epitope recognition pattern.
The data described above might not be surprising, given the observation that even the baseline differences between ACPA-positive and ACPA-negative patients with RA are rather small. Nonetheless, these latter subgroups differ considerably with respect to disease course as measured by radiological progression.42 We feel that it is unlikely that ACPA fine specificity within ACPA-positive disease will have a similar impact as found for ACPA status within RA. This notion is supported by our observation that a similar rate of joint destruction is observed between ACPA-positive patients with high- and low-baseline anti-CCP2 levels as proxy for the extent of epitope recognition. Likewise, recent observations made by our group and others analysing the possible connection between reactivity against a specific citrullinated epitope provided similar indications.38 43
Remarkably, these findings contrast observations made in early/predisease RA, as it has been shown that ACPA-positive subjects who are still healthy or have early arthritis are more likely to develop arthritis when harbouring a more extended generalised citrullinated epitope recognition pattern.24 The reason why ‘maturation’ of the ACPA response with respect to its epitope recognition profile is associated with transition to disease but, once disease is established, not with disease outcome, is not known. However, it is tempting to speculate that once a certain threshold is reached, disease manifestations become apparent. In case ACPA would be involved in disease pathogenesis, it is conceivable that over this threshold, higher levels or a more extended recognition profile does not contribute further to disease progression, as the response is already maximally involved in creation of the harmful inflammatory milieu underlying the signs and symptoms associated with RA.
Although our data indicate that no clear link exists between clinical features and autoimmunity against specific citrullinated antigens, we cannot exclude that antibodies against other citrullinated antigens will correlate with clinical outcome once the disease has emerged. Obviously this could lead to two phenotypically different subgroups. However, we feel that it is more likely that inclusion of more citrullinated epitopes will result in more subgroups as analysing nine reactivities already led to a division into 64 subgroups, each displaying a unique ACPA recognition profile. Likewise, we cannot exclude that associations could be found with a more extended samples size; however, based on our sample size, the effect would still remain small, and increasing sample size further will unlikely result in a meaningful clinical difference.
Altogether, our data indicate that the epitope recognition profile is highly diverse. The recognition of different citrullinated peptides at baseline correlated with similar clinical characteristics, irrespective of differences in peptide-backbone structure, indicating that the breaking of tolerance towards citrullinated proteins as such provides more information than the recognition of a particular peptide or set of peptides.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Web Only Data - This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Web Only Data - This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval METC LUMC.
-
Provenance and peer review Not commissioned; externally peer reviewed.