Article Text

Abstract
Objectives Recently published research suggests that statins may have beneficial structural effects in persons with knee osteoarthritis (OA). The potential effects of statins on patient-reported knee pain and function have not been examined. We studied a large prospective community-based cohort of persons with knee OA to determine if statin usage was associated with changes in knee structure, pain and function trajectories.
Methods Data were obtained from the Osteoarthritis Initiative using a subset of 2207 persons with radiographically suspected or confirmed knee OA. The changes in Western Ontario and McMaster Universities Arthritis Index (WOMAC) Pain and Physical Function scores, pain intensity and Kellgren-Lawrence radiographic grade over 4 years were examined. Data from persons were coded based on whether they were incident users of statins over the 4-year period. Outcome trajectories and probability of statin use were examined over the 4-year study period using parallel processing growth curve modelling. The analysis adjusted for potential confounders and determined if statin use predicted outcome trajectories.
Results Statin users accounted for 6.7% of the sample in year 1 and 16.4% in year 4. Statin use was not associated with improvements in knee pain, function or structural progression trajectories. The only significant finding indicated that increased duration of statin use was associated with worsening in WOMAC Physical Function scores over the study period (β=0.161, p=0.005).
Conclusions Statin use was not associated with improvements in knee pain, function or structural progression over the 4-year study period.
- Knee Osteoarthritis
- Epidemiology
- Health services research
Statistics from Altmetric.com
Research efforts have been focused for many years on the identification of osteoarthritis (OA) interventions that favourably influence patients’ OA status, pain and function. Several researchers have referred to disease-modifying osteoarthritis drug (DMOAD) development efforts as a quest akin to the search for the Holy Grail.1–3 These potentially promising efforts have yet to advance clinical practice.1 ,2 ,4 ,5 Clockaerts et al have added 3-hydroxy-3-methylglutaryl-coenzyme A (HMGCoA)-reductase inhibitors (statins) to the list of potentially promising DMOADs with their recent study of the association between statin use and radiographic knee OA incidence and progression.6 The authors found, in a 6-year population-based cohort study of 2921 older adults, that statin use was associated with a 57% reduction in OR of radiographic knee OA progression relative to non-users of statins (OR 0.43, 95% CI 0.25 to 0.77). Yet radiographic measures of OA are only imperfectly correlated with OA symptoms and function.7
Statins are widely used to lower low-density lipoproteins (LDL) cholesterol, a surrogate marker of risk for cardiovascular morbidity and mortality.8 Evidence of biological effects of statins has shown potentially therapeutic anti-inflammatory and antioxidative effects as well as improved chondrocyte, synovial and bone cell health.1 ,9 ,10 These cellular effects have led some to speculate that statins could be DMOADs, but person-level evidence has been lacking. The work by Clockaerts et al aside, we are not aware of evidence suggesting that statins may alter knee OA related pain and function. Conaghan's accompanying editorial also noted the absence of evidence of effects on pain and functional status: ‘Studies on symptoms may be a feasible step before structural modification trials are considered.’p634
Our purpose was to examine the association between incident statin use and symptoms of knee pain, activity-related pain, functional status or structural progression over a 4-year period in a sample of community-based persons with suspected or radiographically confirmed knee OA. Specifically, we aimed to document the natural course of statin use, pain, functioning and structural progression over 4 years in this population and then predict the pain, function and OA disease status trajectories from statin use trajectories.
Methods
The Osteoarthritis Initiative (OAI) is a publicly and privately funded prospective longitudinal cohort study of community-based persons with or at high risk for knee OA. The study was approved by the Institutional Review Board (IRB) at the OAI Coordinating Center, the University of California, San Francisco. All OAI study details are available on the internet (http://oai.epi-ucsf.org/datarelease/About.asp).
Key exclusion criteria for OAI included presence of rheumatoid arthritis, bilateral knee arthroplasty or pre-existing plans to undergo bilateral knee arthroplasty within 3 years, comorbid conditions that might interfere with 4-year participation, unlikelihood of residing in clinic area for at least 3 years, and unwillingness to sign informed consent. In addition, because the study measured MRI-based changes, men weighing more than 130 kg and women weighing more than 114 kg were excluded because they were unable to fit within a 3.0 Tesla MRI opening.
Data from OAI subjects were included in our study if they: (1) had a Kellgren-Lawrence (KL) grade of 1 or greater on at least one knee, (2) were not taking statins at baseline, (3) did not undergo a hip or knee replacement surgery during the 4-year study period and (4) did not have bilateral end-stage radiographic knee OA based on readings obtained by experts at the central study centre. In total, we had 2207 persons who qualified for the study. These criteria were designed to allow for a cohort that used the same OA disease criteria and were non-statin users at baseline, much like the sample of Clockaerts et al6 The flow of participants leading to the subset under study is depicted in figure 1.

Flow chart illustrating the selection of Osteoarthritis Initiative subjects included in the study.
Statin treatment
Statin therapy was not part of the OAI protocol, but many OAI subjects began statins as a result of routine medical care for lipid disorders. The OAI required participants to bring their medications when attending yearly study visits from baseline to the 4-year follow-up. During these visits, staff reviewed medications and recorded the medication name, self-reported duration and frequency of use (as needed or regular). Because of potential problems associated with recall and bias,11 ,12 we used the yearly in-person visit data to guide coding for statin use. Data related to dosage were not reported in OAI. To capture only incident use of statins, we excluded persons who were using statins at baseline.6
Data were coded in OAI to indicate the type of statin. Lipophilic statins included atorvastatin, simvastatin, fluvastatin and lovastatin while pravastatin was the hydrophilic statin. Because hydrophilic statins accounted for less than 10% of all statin use, we adopted the strategy used by Clockaerts et al6 and did not conduct a separate analysis for each statin type. Because participants brought their medications for each yearly visit, we were able to code duration of use based on whether participants brought their statin medications to each follow-up visit. These data served as surrogate indicators of 1-year, 2-year, 3-year or 4-year statin usage. Persons who did not bring statin medications during a particular follow-up visit were coded as non-users for that visit.
Outcome measures
To quantify pain over all yearly time points, we chose a rating of knee pain measured on a 0–10 scale ranging from 0 indicating ‘no pain’ and 10 indicating ‘pain as bad as you can imagine’ over a 7-day period. These ratings are highly reliable for persons with chronic pain.13 We also used the WOMAC Pain subscale at each time point as a highly reliable and validated measure of activity-related pain, scored on a scale of 0 (no activity-related pain)–20 (severe activity-related pain).14–16 To quantify functional status, we used the WOMAC Physical Function scale which is reliable and valid,14 ,16 ,17 with scores ranges from 0 (normal function) to 68 (severely affected function). We chose the WOMAC Physical Function Scale to measure activity limitation because the scale does not inquire about pain or other symptoms associated with the activities specifically but rather only the extent of difficulty in doing each activity. Patients were asked to complete a WOMAC scale for each knee. Because the WOMAC Pain and Physical Function scales ask about person-level activities and not knee-specific function, we used the higher (worse) WOMAC score at each time point.
Yearly knee OA status was measured using validated flexed knee radiographic procedures that have been described extensively.18 ,19 We used centrally adjudicated KL grades of both knees from the public use data sets. We excluded persons with KL grades 4 or bilateral 0 at baseline much like the work of Clockaerts et al.6 We summed the KL scores for both knees in the analyses and assessed changes in these summed scores over the 4-year period.
Potential confounders
A variety of potential confounders were examined based on the work of Clockaerts et al.6 These were baseline age, gender, body mass index (BMI), smoking status (yes or no), comorbidity (using the validated Charlson comorbidity index which captures diabetes and cardiovascular comorbidity among other disorders),20 presence of high blood pressure (coded as yes if either systolic blood pressure was 160 mm Hg or higher or diastolic blood pressure was 95 mm Hg or higher)6 and education. Extent of education was coded as less than a high school degree, high school degree or at least some college.
Data analysis
Baseline characteristics of subjects with and without statin use were compared using Student's t test and Pearson's χ2. We used structural equation modelling (SEM) to estimate the effect of change in statin use on changes in pain, physical functioning and structural progression measured at four occasions (yearly visits from 1 to 4 years following the baseline visit). In all SEM models, the following covariates are included: age, sex, smoking, high blood pressure, education, comorbidity and BMI; by including such covariates in multivariate modelling, the results represent effects independent of covariates. Mplus V.6 was used to fit the SEM.21 We used the full information maximum likelihood method to handle the missing data. The full information maximum likelihood allows for estimating the SEM using all available data without imputing values for missing data and has been shown to outperform existing missing-data-handling methods.22
Initially, we estimated the latent growth curves (LGC)23 separately for statin use, WOMAC Physical Function, WOMAC Pain, verbal pain rating measures and KL scores without covariates using four yearly repeated measurements for each variable. We repeated these analyses with covariates. Use of LGC allows for the modelling of trajectories of improvement and worsening in outcomes over the four time periods and we were interested in determining if changes in pain, function and structural progression were predicted by changes in statin use over time. By using LGC, we were able to take full advantage of all data to determine if statin use trajectories predicted changes in the trajectories of pain, function or radiographic disease progression, independent of covariates.
The LGC is parametrically equivalent to the random regression model, multilevel model and PROC MIXED in SAS. The growth parameters included random intercept, random linear slope and random quadratic slope. The orthogonal polynomials were used to represent time in the model. Because statin use was measured as a binary variable at each time point, the logistic link was used to estimate the model. For the outcome measures, we used the Gaussian link function. The full SEM specification, also known as parallel processing growth curve models, included path coefficients relating the statin use growth parameters to four outcomes separately, that is, the growth parameters reflecting physical function, the two pain measures and the disease progression measure.
The best fitting LGC model was used in the full SEM. In the model specification of the full SEM, the statin growth parameters (ie, slope and intercept) were used to predict the growth parameters (ie, slope and intercept) of the four outcome measures separately. The full SEM models also included covariates. Model fit was evaluated with χ2, Root Mean Square Error of Approximation (RMSEA) and 90% CI, Comparative Fit Index (CFI), and Tucker-Lewis Index (TLI).
In the full SEMs, the intercept for statin use describes the duration of statin use. For example, the intercept for a person who used statins for 1-year would be less as compared with a person who used statins for 3-years. The slope for statin use describes changes in statin use over the study period. For the outcome measures, the intercept describes the initial outcome scores. For example, one person might have WOMAC Physical Function scores of 5, 7, 11 and 13 at four occasions with a lower intercept than another person with scores of 20, 16, 14 and 10 measured at the same four occasions. The slope for outcome measures, whether linear or quadratic, describes the change in outcome scores over the study period. Increasing outcome scores over time reflect worsening and decreasing scores indicate improvement.
Results
A total of 2207 persons were included in the study, of whom 448 (20.3%) were statin users for at least one year. The statin user group was slightly older (by a mean of 1.8 years), heavier (by a mean BMI of 1.1 kg/m2), more frequently hypertensive, and had a higher comorbidity score than the non-user group. Statin users also had worse WOMAC Pain, Physical Function and 7-day knee pain scores at all time periods as compared with non-users. KL scores were no different between statin-user and non-user groups. Rate of follow-up exceeded 90% for all outcomes with the exception of radiographic measures which ranged from 94.2% in year 1 to 80.8% in year 4. During the study, 7-day pain, WOMAC Pain and WOMAC Physical Function scores varied only slightly over the 4-year period (table 1).
Characteristics of the statin use and statin non-use samples (n=2207)
Initially, we fit quadratic growth curves for the statin, physical functioning, pain and progression measures. Because the quadratic term for statin use was not significant, we used only the linear growth curve for statin use. We retained the quadratic growth models for the WOMAC Pain, WOMAC Physical Function, 7-day Pain and structural progression measures. The LGC models fit the observed data well: (a) Statin use: χ2=14.633, df=2, p<0.001; RMSEA=0.053; 90% CI=0.030 to 081; CFI=0.999; TLI=0.998; (b) WOMAC Pain: χ2=0.076, df=1, p>0.10; RMSEA=0; 90% CI=0 to 0.037; CFI=1.000; TLI=1.001; (c) WOMAC Physical Function: χ2=2.860, df=1, p>0.05; RMSEA=0.029; 90% CI=0 to 0.071; CFI=1; TLI=0.998; (d) 7-day Pain: χ2=0.012, df=1, p>0.10; RMSEA=0; 90% CI=0 to 0.022; CFI=1.000; TLI=1.002, and (e) KL Grades: χ2=5.421, df=1, p>0.05; RMSEA=0.029; 90% CI=0 to 0.060; CFI=1.000; TLI=.999. The estimated LGC for statin use and four outcomes are depicted in figure 2, Panels A–E.
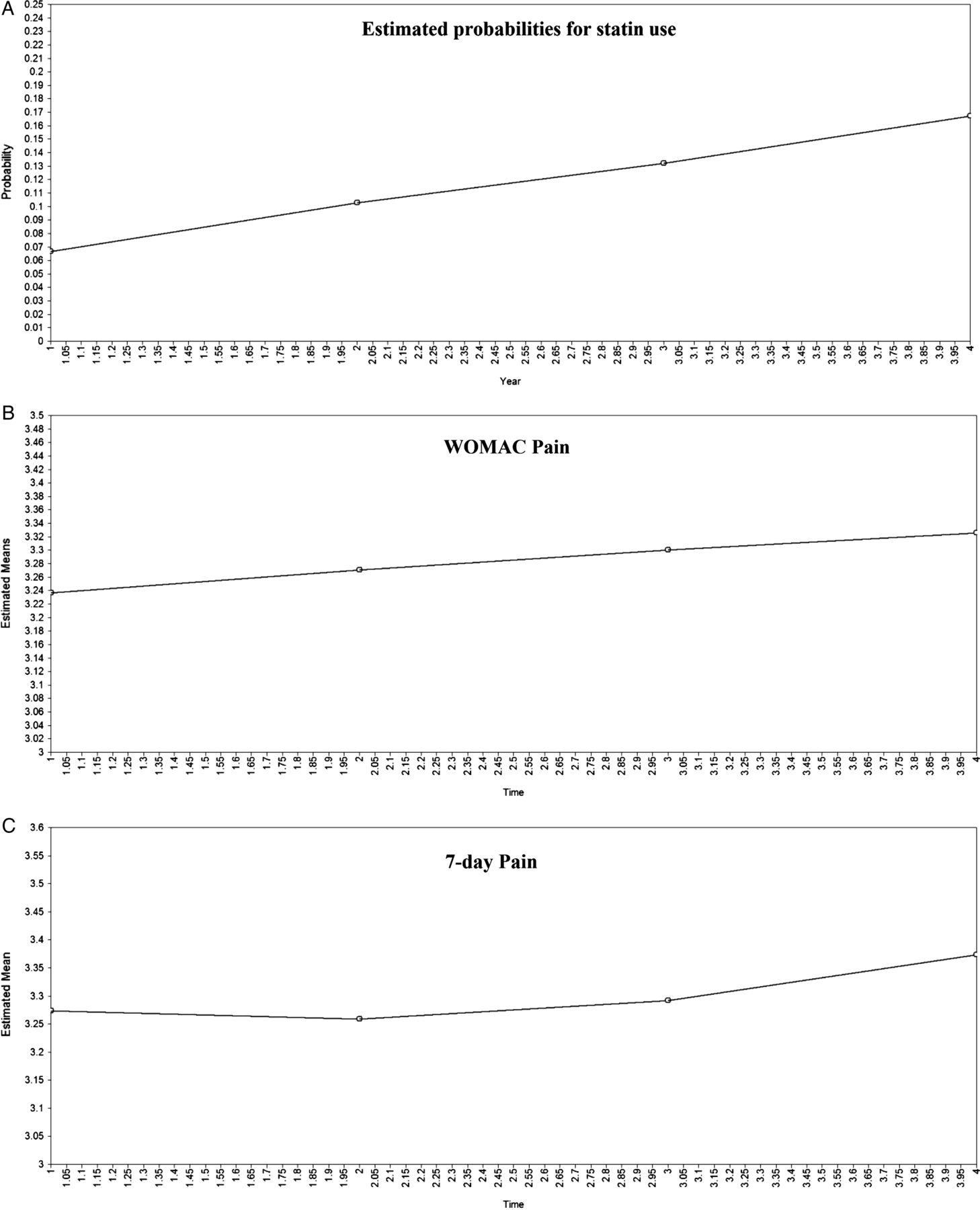

The 4-year growth curves of statin use and the four outcome measure probabilities are illustrated. The x-axis in all panels indicates time in years. The y-axis in all panels indicates the scale for each measure. The growth curves were generated without inclusion of the covariates summarised in table 2. Panel A shows the statin use growth curve, panel B shows the WOMAC Pain growth curve, Panel C shows the 7-day pain growth curve, Panel D shows the WOMAC Physical Function growth curve and Panel E shows the radiographic progression growth curve.
Four full SEMs were estimated with the growth parameters of statin use, WOMAC Pain, WOMAC Physical Function, 7-day pain and progression. For each model, the predictors were the growth parameters of statin use and covariates. The fit statistics indicated good fit for these models: (a) WOMAC Pain: χ2=52.082, df=35, p<0.05; RMSEA=0.015; 90% CI=0.005 to 0.023; CFI=0.999; TLI=0.997; (b) WOMAC Physical Function: χ2=28.950, df=35, p<0.01; RMSEA=0.024; 90% CI=0.012 to 0.035; CFI=0.999; TLI=0.997; (c) 7-day Pain: χ2=68.027, df=35, p<0.001; RMSEA=0.021; 90% CI=0.013 to 0.028; CFI=0.998; TLI=0.994, and (d) KL Grades: χ2=46.989, df=35, p>0.05; RMSEA=0.013; 90% CI=0 to 0.022; CFI=0.999; TLI=0.998. To illustrate, the full SEM for WOMAC Physical Function is provided in figure 3.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
The figure illustrates the full Structural Equation Model for WOMAC Physical Function and statin use. Statin-1, Statin-2, Statin-3, and Statin-4 represent the observations of statin use at each yearly follow-up visit, and Function-1, Function-2, Function-3, and Function-4 are the corresponding observations of WOMAC Physical Function. Covariates are illustrated at the top of the figure. The relationship among the four measurements of statin use is captured by random intercept and linear slope parameter estimates, each of which are represented as latent variables (ie, the STATIN circles in the figure) whereas the relationship among the four measurements of WOMAC Physical Function is captured by random intercept, linear slope and quadratic slope parameter estimates (ie, the FUNCTION circles in the figure). The arrows from the covariates to five growth parameter estimates (ie, STATIN and FUNCTION circles) are used to partial out the covariate effects in the predictions of FUNCTION parameters from the STATIN parameters. The arrows from the STATIN growth parameters to the FUNCTION growth parameter estimates indicate that the probability of Statin use over time was used to predict the stability and change in Function over time. Analogous models were developed for 7-day pain rating, WOMAC Pain and radiographic knee osteoarthritis progression using the follow-up visit observations.
Parameter estimates from the four full models appear in table 2. The relationship between the statin use intercept and the linear slope of WOMAC Physical Function was significant (β=0.161, p=0.005). Longer duration of statin use predicted greater worsening of physical functioning over the 4-year period. There were no other significant relationships between statin growth parameters and the growth parameters for function, pain or radiographic progression outcomes. Covariates were most consistently associated with the intercepts of the outcome and statin use growth parameters in the full SEM growth curves. There were only very minor differences among the univariate and covariate adjusted growth curve estimates (data not provided).
Standardised parameter estimates from the parallel processing growth curve models with covariates
Discussion
This study was prompted by the recent report by Clockaerts et al who found reduced risk for radiographic knee OA associated with statin use.6 If statins truly reduce structural knee OA development or progression, one could predict that statins may also reduce OA-related pain and improve function. The full SEM growth curve models incorporating statin use, outcomes and covariates fit our data well. The models indicated that, after adjustment for confounding, statin use or duration does not predict knee pain, function or radiographic progression trajectories in a positive fashion over the 4-year period (see table 2).
Our study has several strengths but also some limitations. The OAI is a prospective community-based cohort study with a large sample size, rigorous case definition, a 4-year follow-up rate of approximately 90% for most measures, and an extensive number of validated covariate and outcome measures. Much like the study by Clockaerts et al, we only included persons with evidence of statin use during the 4 years of follow-up but no statin use at baseline.6 Our study had almost double the percentage (20.3%) of statin users compared with the Clockaerts et al6 study (10.85%) and this appears to be an adequate sample size for assessing effects of statins on progression. There are also notable limitations. The extent of pain and reduced function in our sample generally represents a less severe symptom spectrum which may have made identification of changes associated with statin use more difficult to identify. We cannot rule out the possibility that statin use may impact pain and functional status in samples of persons with more severe symptoms. However, radiographic changes at baseline were clear with mean summed KL scores at approximately 3 (SD=1.5) on the 0–8 scale. A total of 59.5% of the right knees and 56.2% of the left knees in our sample had KL grades of ≥2 while the sample of Clockaerts et al6 were less involved with approximately 11% of knees with KL scores of ≥2. It is unclear to us whether these differences may have influenced our findings. In addition, the percentage of knees in our sample that demonstrated progression to a ≥2 KL score over the 4-year study period was 4.8%. In the Clockaerts et al study, 6.9% of knees progressed to a ≥2 KL score over a 6.5 year study period. While these percentages are not directly comparable given the different time periods, we find these estimates to be reasonably similar, after accounting for our shorter study period. Rates of progression in both studies are somewhat low but not substantively different from one another.
While our analysis accounted for variation in duration of statin use, our study did not examine the potential impact of intrinsic biological differences that may contribute to disease progression. Unlike the study by Clockaerts et al,6 we did not have data indicating statin dosage. Typically, statin doses are titrated to reduce LDL cholesterol to a specified level, and so the therapeutic statin dose for cholesterol lowering could differ from a theoretical optimum for OA-related benefits. It is thus possible that some subjects in our study were underdosed which may have influenced our findings. In addition, because OA development and progression may occur over periods longer than the OAI follow-up, measurable effects on improved OA pain and functional status could be apparent with follow-up longer than 4 years. Statin use also may be associated with increased muscle or soft tissue related pain among persons without arthritis though statin users with arthritis had no increased muscle and soft tissue pain relative to non-users.24 Knee pain and reduced function also may reflect processes other than OA-related structural changes, such as development of local inflammation, periarticular disorders, referred pain, bone marrow lesions and nociceptor sensitisation.25 Statins would likely have no effect on symptoms associated with these processes. Therefore, a beneficial joint-cartilage structural alteration with statin use might not directly lead to reduced pain and improved function.
Our study has potential implications for policymakers and clinicians. If statins do not consistently influence OA progression or symptom status in large sample cohort studies, one must question their potential for future trial funding. If symptom status must change with statin use to justify more definitive trials as Conaghan suggests,1 our study provides disappointing results. While far from definitive, our study fails to support statin influence on OA structural progression, conflicting with work of Clockaerts et al, and provides evidence that symptom status over a period of 4-years is not affected by statin use. To overcome limitations in our study, future research should examine samples with more severe symptoms over at least a 4-year period and preferably longer. Statin dosage should be measured to assure that recommended levels were achieved.
In sum, this study demonstrated that statin use did not influence radiographic progression, pain or self-reported function in a large cohort of persons with confirmed or suspected knee OA. Taken in the context of the study of Clockaerts et al,6 our study suggests that whatever structural effects in radiographic OA that statins might have, statin use appears to have no significant effect on OA-related pain or self-reported functional status.
References
Footnotes
-
Contributors All authors contributed to the conception and design of the study and interpretation of the findings. LD conducted the analysis. All authors assisted in drafting the article and gave final approval of the current draft.
-
Funding The OAI is a public-private partnership comprised of five contracts (N01-AR-2-2258; N01-AR-2-2259; N01-AR-2-2260; N01-AR-2-2261; N01-AR-2-2262) funded by the National Institutes of Health, a branch of the Department of Health and Human Services, and conducted by the OAI Study Investigators. Private funding partners include Merck Research Laboratories; Novartis Pharmaceuticals Corporation, GlaxoSmithKline; and Pfizer, Inc. Private sector funding for the OAI is managed by the Foundation for the National Institutes of Health. This manuscript was prepared using an OAI public use data set and does not necessarily reflect the opinions or views of the OAI investigators, the NIH, or the private funding partners. The authors are not part of the OAI investigative team and have no other competing interests.
-
Competing interests None.
-
Ethics approval University of California, San Francisco IRB.
-
Provenance and peer review Not commissioned; externally peer reviewed.