Article Text

Abstract
Objective: To investigate time trends, geographical variation, and seasonality in the incidence of diagnosis of polymyalgia rheumatica (PMR) and temporal arteritis (TA) in the United Kingdom.
Methods: Analysis of computerised medical records from UK general practices. Participants were registered with a practice contributing to the General Practice Research Database during the period 1990–2001. The main outcome measures were rates of diagnosis by year, age, sex, geographical region, and calendar month.
Results: 15 013 people had a first diagnosis of PMR and 3928 a first diagnosis of TA during 17 830 028 person-years of observation. The age adjusted incidence rate of PMR was 8.4/10 000 person-years (95% CI 8.3 to 8.6), rising from 6.9/10 000 person-years in 1990 to 9.3/10 000 in 2001. The age adjusted incidence rate of TA was 2.2/10 000 person-years (95% CI 2.1 to 2.3) with no increase observed. Both PMR and TA were more common in the south than in the north of the UK, and both were more commonly diagnosed in the summer months.
Conclusions: The explanation for the findings is unclear. Variations in diagnostic practice and accuracy are likely to have contributed in part to the patterns seen. However, the findings are also likely to reflect, at least in part, variations in the incidence of disease. The striking geographical pattern may be partly attributable to a risk factor which is more prevalent in the south and east of the United Kingdom.
- CI, confidence interval
- ESR, erythrocyte sedimentation rate
- GPRD, General Practice Research Database
- PMR, polymyalgia rheumatica
- TA, temporal arteritis
- incidence
- polymyalgia rheumatica
- temporal arteritis
- United Kingdom
Statistics from Altmetric.com
- CI, confidence interval
- ESR, erythrocyte sedimentation rate
- GPRD, General Practice Research Database
- PMR, polymyalgia rheumatica
- TA, temporal arteritis
The causes of polymyalgia rheumatica (PMR) and temporal arteritis (TA) are not known.1,2 Age and female sex are established risk factors, a genetic component seems likely, and infection may have a role. The relationship between the two conditions is uncertain.3 Many authorities consider them to be different manifestations of the same disease process, while others see them as closely related but different diseases.3 The term giant cell arteritis is sometimes used to describe TA only, but is sometimes used to refer to both TA and PMR.
The variable clinical course of these conditions, particularly in response to steroid treatment, makes the assessment of prevalence difficult to interpret. Incidence rates therefore provide a better guide to disease occurrence. Patients, especially those with PMR, are rarely referred to secondary or tertiary care. This has limited the opportunities for descriptive epidemiology. The two previous published studies of incidence of these conditions in the United Kingdom come from single general practices.4,5 We investigated time trends and regional variation in the incidence of the diagnosis of PMR and TA using data obtained from the UK General Practice Research Database (GPRD).
MATERIALS AND METHODS
General Practice Research Database
The GPRD was set up in 1987, then known as the VAMP (Value Added Medical Products) Research Bank.6 It consists of the electronic clinical records of patients registered with contributing general practices and aims to include complete prescribing and diagnostic information. The practices included in the GPRD are broadly representative of all practices in England and Wales in their geographical distribution, practice size, and the age and sex distribution of registered patients.7 Contributing practices must meet a range of data quality criteria before they are included in the GPRD. The quality of the information in the database, including the completeness of recording of diagnoses made in medical facilities outside the practice, has been validated in a number of independent studies and has been found to be high.6 There is excellent agreement between prescribing data from the GPRD and national data from the Prescription Pricing Authority.8 Each person is assigned a unique identification number, and all data that might identify an individual patient are removed from the records before they are incorporated into the GPRD.
Study population and denominators
The information analysed in this study comprised the electronic medical records of people registered with general practices contributing data to the GPRD during the period 1 January 1990 to the 31 December 2001.
For a specific general practice, the start of the observation period for this study was taken as the later of either 1 January 1990 or the date at which the practice started contributing data to the GPRD. The end of the observation period was the earlier of the date at which the practice stopped contributing data to the GPRD or the 31 December 2001. The number of practices included in the GPRD varied during the study period, rising from 444 in 1990 to 557 in 1996, then falling to 380 by 2001.
Age- and sex-specific rates were calculated for people registered with contributing general practices during each calendar year using the mid-year registered population as the denominator for each year. People were classified by geographical location of their general practice by country for Wales, Northern Ireland, and Scotland, and by the eight former administrative National Health Service regions for England.
Identification of cases
Cases were defined as people aged 40 years or older who had a first diagnosis of polymyalgia rheumatica or temporal arteritis entered into their general practice record while registered with a practice contributing to the GPRD during the study period (the codes used are available on request). People with diagnosed PMR were included in the PMR analysis even if they had a previous diagnosis of TA and vice versa. To be included, cases had to have at least two prescriptions for oral corticosteroids: one within 6 months of the diagnosis date, with the two prescriptions being within 6 months of each other, used to indicate a clinical response to corticosteroids. When a patient first registers with a practice contributing to the GPRD, past medical events and diagnoses judged to be clinically important by the general practitioner are recorded in the electronic record, with the date of each diagnosis where available. However, such past diagnoses may be erroneously recorded as occurring on the date of data entry.9 Therefore, diagnoses recorded within the first week of registration or at registration health screening consultations during the first 6 months of observation for each patient were not included.
Validation of a recorded diagnosis of temporal arteritis
Some of the general practices contributing data to the GPRD provide anonymised copies of hospital letters and specialist reports on individual patients. Hospital letters were requested for a sample of 50 cases with a diagnosis of TA recorded in their electronic GPRD record. Of the 50 notes requested, 45 (90%) were obtained. The extent of investigation of patients varied and was insufficient to allow us to apply strict diagnostic criteria. Overall, on the basis of typical symptoms and a clinical response to corticosteroids, the physician diagnosis of TA was supported in 41/45 (91%) cases. There was no further information to support the recorded diagnosis of TA in two cases, one case was a speculative diagnosis only, and the symptoms of one case were later ascribed to hydrocephalus, not TA. Only 5/45 cases had a recorded temporal artery biopsy: three positive and two negative. Both patients with negative results had symptoms typical of TA, a raised erythrocyte sedimentation rate (ESR), a clinical response to steroids, and were considered by hospital clinicians to have TA even though the biopsy was negative. A recorded ESR result was available for 29/45: this was raised in all but two cases, but for one of these the ESR was measured several months after the diagnosis of TA. Ten of 45 cases were not referred to hospital, but were investigated and managed in primary care.
Analysis
Crude rates, age standardised incidence ratios, and age adjusted incidence rates of first diagnosis were calculated by year of diagnosis and sex and for different geographical regions.10 Because of the small numbers of cases in some years, indirect standardisation was used, with rates during the whole study period as the standard rates. To investigate seasonality, a Poisson model was fitted to the average rate of diagnosis by calendar month. Likelihood ratio tests were used to assess the effect of adding a factor for seasonality to the model for the observed monthly rates over the study period.
Ethical approval
Ethical approval for the study was obtained from the Scientific and Ethical Advisory Group of the GPRD and the ethics committee of the London School of Hygiene and Tropical Medicine.
RESULTS
The total observation period was 17 830 028 person-years. We identified 15 013 people with a first diagnosis of PMR during the study period who met the inclusion criteria, with a mean age at diagnosis of 72.7 years. Table 1 shows the crude rates of first diagnosis of PMR, age standardised incidence ratios, and age adjusted rates by year of diagnosis.
Rates of first diagnosis of PMR, age standardised incidence ratios, and age adjusted rates by year of diagnosis
The overall age adjusted incidence rate of PMR was 8.4/10 000 person-years (95% confidence interval (CI) 8.3 to 8.6) with the female to male ratio being 2.0. There was a marked increase in the incidence of PMR throughout the 1990s, from 6.9/10 000 person-years in 1990 to 9.3/10 000 person-years in 2001. There was little variation in the sex ratio.
We identified 3928 people with a first diagnosis of TA during the study period who met the inclusion criteria. The mean age at diagnosis was 72.8 years. Table 2 shows the crude rates of first diagnosis of TA, age standardised incidence ratios, and age adjusted rates by year of diagnosis.
Rates of first diagnosis of TA, age standardised incidence ratios, and age adjusted rates by year of diagnosis
The overall age adjusted incidence rate was 2.2/10 000 person-years (95% CI 2.1 to 2.3) with the female to male ratio being 2.6. There was no increase in the incidence of TA during the study period and little variation in the sex ratio.
Table 3 shows the age-specific rates of first diagnosis of PMR and TA by sex.
Rates of first diagnosis of PMR and TA by age at diagnosis
The rates of both PMR and TA rose sharply with increasing age. For both conditions, the female to male sex ratio in incidence rates became much less marked as age increased.
Among the 15 013 people with incident PMR, 774 (5.2%) had previously been diagnosed with TA. A further 382 people (2.5%) were diagnosed with TA after being diagnosed with PMR, and 39 people (0.26%) were diagnosed with both PMR and TA on the same day. Among the 3928 people with incident TA, 585 people (14.9%) had previously been diagnosed with PMR. A further 558 people (14.2%) were diagnosed with PMR after being diagnosed with TA. During the observation period, the number of people diagnosed with both PMR and TA was around 38 times greater than would have been expected if there was no association between the two diseases.
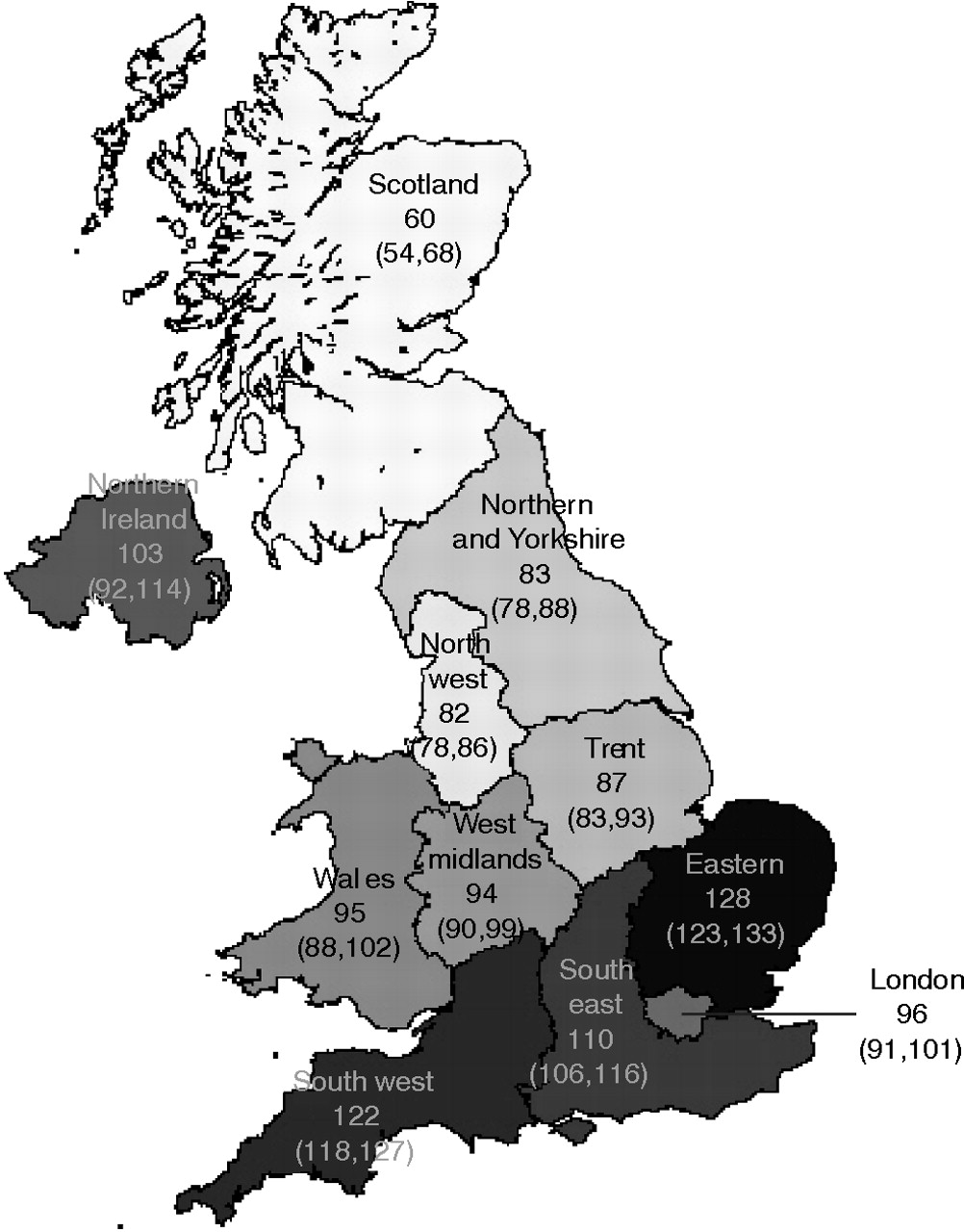
Figures 1 and 2 show the age standardised incidence ratios of PMR and TA by region of the UK. There were marked geographical variations in the incidence of both PMR and TA (p<0.001 for test of heterogeneity of rates by region). Both conditions were much more common in the south than in the north of the UK, with rates in Scotland being around half the rates seen in south and east England.

Age standardised incidence ratios for PMR by region with 95% CIs. Overall average is 100.

Age standardised incidence ratios for TA by region with 95% CIs. Overall average is 100.
Figures 3 and 4 show rates of PMR and TA by calendar month, both observed and fitted values. Both conditions were considerably more likely to be first diagnosed in the warmer summer months, and this was true for every individual year in the study period (1990–2001 inclusive). Adding a factor for seasonality improved the fit of the models for both PMR (p<0.001) and TA (p = 0.0022), suggesting the seasonal effects observed were unlikely to be due to random error.

Monthly rates of first PMR diagnosis. Observed values with 95% CIs, and fitted values linked by the dashed line.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Monthly rates of first TA diagnosis. Observed values with 95% CIs, and fitted values linked by the dashed line.
DISCUSSION
We found that between 1990 and 2001 in the United Kingdom, the incidence of diagnosis of PMR increased by around one third while the incidence of TA remained stable. For both conditions there were marked regional variations in incidence rate, and the rate of first diagnosis was higher in the summer months. Variations in ascertainment and diagnostic practices may explain, in part, the patterns seen, but trends in the incidence of these diseases might also have contributed.
In previous studies, the incidences of both PMR and of TA have shown marked geographical variations, with higher rates at northern latitudes. The highest rates have been found in Scandinavia. In Norway in the period 1987–94, the annual rate of PMR among people aged 50 years and over was estimated to be 11.2/10 000 and that of TA to be 2.9/10 000.11 Much lower rates have been found in southern Europe and Israel; for example, the annual rate of PMR among people aged 50 years and over in Spain was estimated to be 1.9/10 00012 and that of TA to be 1.0/10 00013 This geographical variation is widely thought to be due to genetic factors,14,15 a hypothesis supported by the high rates of both conditions seen in Olmsted County, Minnesota, where the population has a northern European ethnic background.16,17 Our estimates for incidence from the UK seem consistent with the variation in rates with latitude found elsewhere in Europe, being in between the rates for northern and southern Europe. The two previous published population based studies of incidence of these conditions in the UK came from single general practices. The first identified nine new cases of TA over a period of 4½ years in the early 1950s, with an estimated incidence of 5.4/10 000 person-years 4 The second identified 19 incident cases of either PMR or TA during the late 1970s and early 1980s and estimated the annual incidence among people aged 65 years and over to be 40/10 000.5 Both these estimates were somewhat higher than the incidences we obtained, but were derived from small localised populations.
As far as we are aware, the marked regional variations in incidence of diagnosis rates for both conditions observed within a country is a new finding. The direction of the gradient, with higher rates in the south, is in the opposite direction from that previously seen when comparing rates between countries. Although regional variations in ascertainment might have contributed to the patterns we observed, it seems unlikely that differential ascertainment could explain all the variation. Genetic factors are also unlikely to explain much of the regional variations observed. The possibility of unidentified aetiological factors that vary by region warrants further research. Social class might be one such contributing factor, with, on the whole, higher rates seen in better off areas of the country.
Previous large studies from several different countries of time trends in incidence have been inconsistent. Most studies have found that the incidence of PMR is fairly stable2,16 while that of TA is increasing.13,18 We found just the opposite: an increasing rate of PMR and stable TA. However, recent data from the USA suggest that the incidence of TA has stabilised during the past 20 years after three decades of increase,17 a finding consistent with our own study in the UK. The time trends in incidence we observed for the two conditions may reflect a true variation in incidence or may be due to changes in ascertainment of the two conditions. However, why changes in ascertainment would be different for PMR and for TA is unclear. Various diagnostic and classification criteria for PMR and TA were published at the beginning of the study period or before.19–23 It seems unlikely that publication of these criteria could explain the patterns of incidence we observed.
Seasonal patterns of incidence of these conditions have been proposed as evidence to support an infectious aetiology, although the previous findings relating to seasonality have been somewhat inconsistent. Clustering of diagnoses in the early summer months similar to that seen in our study has been reported,24–26 while other studies have reported peaks in the winter months.27,28 Other studies have reported no seasonal effect.29–31 However, none of the previous studies approached the size of the current study. As in previous studies, the higher rates we observed in the summer months were of first recorded clinical diagnosis, not of onset. We are not therefore in a position to estimate the exact relationship between season and biological onset. However, our findings support a seasonal variation in incidence, and thus support an aetiological or precipitating factor that itself varies throughout the year. A marked seasonal variation in diagnostic practice seems an unlikely explanation for this finding.
The main weakness of this study is the validity of recording of diagnoses of PMR and TA. As well as a recorded diagnosis, included cases had to have had at least two prescriptions for oral corticosteroids: one within 6 months of the diagnosis date, with the two prescriptions being within 6 months of each other. This criterion suggests a clinical response to corticosteroid and supports the accuracy of the diagnosis.32–34 However, it is likely that the use of steroids and likelihood of diagnosing these conditions varies considerably between individual general practitioners. For people with both PMR and TA diagnoses, the first diagnosis might have increased the likelihood of ascertainment of the second diagnosis, and thus the number of people with both diagnoses might have been inflated.
For TA, we obtained hospital letters for a sample of cases in order to try to validate the recorded diagnosis. The intensity of clinical investigation was insufficient to allow us to apply strict diagnostic criteria, but on the basis of typical symptoms and a clinical response to corticosteroids, the recorded diagnosis of TA was supported in 41.45 (91%) cases.
The validity of diagnoses recorded in the GPRD has been found to be high for a diverse range of other chronic conditions, including, for example, cataract, myocardial infarction, schizophrenia, fibrosing alveolitis, and dementia.6 However, most of these conditions are clearly defined. For less well defined conditions (such as PMR) the validity of the data in GPRD may possibly be lower. Although there is some evidence to support the validity of a recorded diagnosis of PMR or TA, it is clear that the level of investigation of patients in routine clinical practice would not allow the application of rigorous diagnostic criteria. Wide variations in the diagnosis of PMR and TA among both general practitioners35,36 and hospital specialists35 have been found and are likely to have been present in this study. An additional consideration is our use of date of diagnosis, not of clinical onset. However, this would have had little impact on the patterns seen in the study.
We have shown that PMR and TA are relatively commonly diagnosed in the UK and confirmed that increasing age and female sex are major risk factors. The explanation for the rising rates of PMR and stable rates of TA is not clear, but changing patterns of diagnostic practice with time may have contributed. The seasonal variations observed seem unlikely to be due to seasonal variation in diagnostic factors. The striking geographical pattern might be influenced by variations in diagnostic practice but may not entirely result from this. The pattern suggests the influence of a risk factor which is more prevalent in the south and east of the UK.
Acknowledgments
We thank Kate Lachowycz for drawing the maps and EPIC for supplying the data.
REFERENCES
Footnotes
-
Published Online First 13 January 2006
-
Funding: the study was funded as part of a United Kingdom Medical Research Council Clinician Scientist Fellowship awarded to LS.