Article Text

Abstract
Objectives: To evaluate the use of MRI and FDG-PET for the diagnosis and measurement of disease activity of inflammatory aortic arch syndrome in patients with complicated giant cell arteritis.
Methods: MRI and FDG-PET were performed for 25 patients with giant cell arteritis who presented with a complicated disease course despite immunosuppressive therapy. Disease activity of the thoracic aorta and the supra-aortic arteries as assessed by both modalities was compared with serological (C-reactive protein (CRP), erythrocyte sedimentation rate (ESR)) and clinical findings (Birmingham vasculitis activity score (BVAS.2)). Additionally, the usefulness of MRI for assessment of vessel wall thickening, aneurysms and stenoses was evaluated.
Results: In 17/25 patients, MRI disclosed structural vessel lesions suspicious for vasculitis. Active disease was detected by MRI, thoracic PET, and whole body PET in 22, 14 and 20 patients, respectively. While serological and clinical findings correlated significantly with each other, there was no concordance with MRI and only low, non-significant correlation of PET with CRP (rs = −0.158, 0.136), ESR (rs = −0.232, 0.320) and BVAS.2 (rs = −0.064, 0.221) for disease activity.
Conclusions: MRI and PET are unreliable for assessing large-vessel inflammation in patients with giant cell arteritis and pre-existing immunosuppressive therapy. MRI is valuable for its ability to detect morphological vessel lesions, such as aneurysms and stenoses.
Statistics from Altmetric.com
About 15–27% of patients with giant cell arteritis (GCA) have extracranial involvement. Typical complications are vaso-occlusive lesions of the upper limb arteries, and aneurysms, especially of the thoracic aorta, in the course of inflammatory aortic arch syndrome.1–3 A limited number of studies using positron emission tomography with fluorodeoxyglucose (FDG-PET) or magnetic resonance imaging (MRI) in patients with GCA and polymyalgia rheumatica, mostly performed during acute disease activity, demonstrated thickening, oedema and increased contrast media uptake in the vessel wall on MRI and increased FDG uptake on PET as features of active vasculitis.4–10 Two studies have compared these modalities in the same patient group, and both found that FDG-PET corresponded with clinical data better than MRI.5 6
The immediate initiation of immunosuppressive treatment upon clinical diagnosis often prevents acquisition of baseline imaging status of the aortic arch. Nevertheless, patients with complications or prolonged disease may require imaging procedures despite the missing baseline examination. The value of MRI and PET in such clinical situations has not been investigated. The aim of this study was to evaluate MRI- and PET-mediated assessment of large-vessel inflammation in patients with GCA and pre-existing immunosuppressive therapy.
PATIENTS AND METHODS
Patients and clinical anamnesis
Twenty-five consecutive patients (20 women and 5 men; mean age 66 years) with complicated courses of GCA despite immunosuppressive therapy (persistent inflammatory markers, n = 18; arm claudication, n = 7; suspicion of aortic aneurysm, n = 4) were evaluated using MRI of the thorax and whole-body FDG-PET. The criteria for GCA were fulfilled in all patients.11 Immunosuppressive drug treatment (average duration 37 months, range 1–72) included prednisolone 7.5–40 mg/day (n = 8), prednisolone 5–15 mg/day combined with methotrexate 15–25 mg/week (n = 12) and prednisolone 8–25 mg/day combined with intravenous cyclophosphamide 800–1000 mg every 15–21 days (n = 5). Mean C-reactive protein (CRP) was 23 mg/l and mean erythrocyte sedimentation rate (ESR) was 40 mm after the first hour. There was no evidence of other causes for increased inflammatory parameters. The Birmingham vasculitis activity score (BVAS.2) was positive in all cases (mean 6.3; table 1).
Imaging
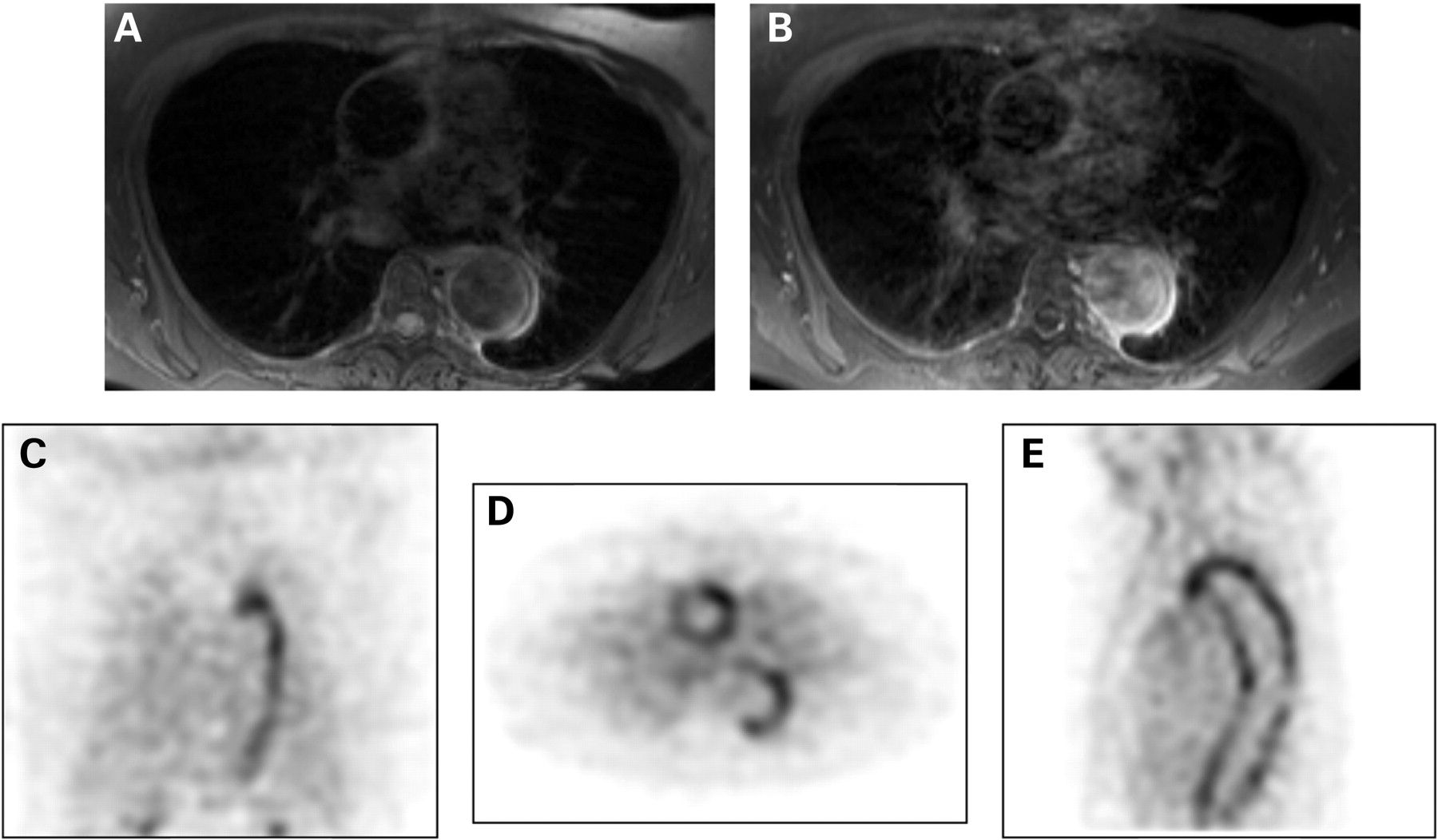
MRI and PET (figs 1 and 2) were performed within 3–14 days without change in treatment. All patients provided prior informed consent. The local ethics committee was consulted; however, they declined involvement because MRI and PET were clinically indicated.


{kind=link}
{kind=link}
MRI
MRI of the thoracic aorta and the supra-aortic arteries was performed using the 1.5 Tesla Magnetom Vision, (Siemens, Germany). ECG-gated MRI was acquired with a transverse T1-weighted FLASH two-dimensional sequence, a transverse fat-suppressed T2-weighted fast spin-echo sequence, and an oedema-sensitive TIRM sequence in the oblique sagittal plane. MR angiography and transverse fat-suppressed ECG-gated T1-weighted spin-echo sequence were performed with gadolinium-DTPA (Magnevist, Schering AG, Germany). Images were assessed by two experienced radiologists (MBo, MR) who were unaware of PET results and clinical data.
Ascending aorta, aortic arch, descending aorta and supra-aortic arteries were evaluated for morphological changes (table 1). A visual, semiquantitative scoring system was applied to each region. Scoring ranged from 0 to 3 (disease activity: 0, none; 1, slight; 2, marked; 3, intense). Total disease activity was defined with a comprehensive activity score (range 0–12).
FDG-PET
PET was performed with a gamma camera-based Marconi/Philips AXIS. Patients fasted for at least 4 hours before tracer application ([18F]FDG activity 320–360 MBq). Corticosteroids were withheld on the day of investigation. The ascending aorta, aortic arch, descending thoracic aorta, supra-aortic branches, abdominal aorta and lower extremity arteries were evaluated. Scans were read by two experienced nuclear medicine doctors (MBä, OD) who were unaware of MRI and clinical data. Visual evaluation of FDG uptake was scored from 0 to 3, as described for MRI. To compare MRI and PET, a comprehensive PET-activity score was determined with regard to the thoracic aorta and the supra-aortic branches only (“thoracic” PET; range 0–12) and with regard to all vascular regions (“whole-body” PET; range 0–18).
Statistical analysis
The non-parametric Spearman’s correlation coefficient, rs, was calculated to compare the disease activity determined by MRI and PET. Wilcoxon signed-rank test was used to investigate differences between these scores. A value of p<0.05 indicated significance. The correlation between CRP, ESR and BVAS.2 and the correlations of these measures with MRI and PET were evaluated using Spearman’s coefficient.
RESULTS
Activity scores
MRI, thoracic PET and whole-body PET detected signs of active vasculitis in 22, 14 and 20 of 25 patients, respectively (table 1).The correlation between disease activity scores of MRI and PET was low (rs = 0.350, p = 0.086). For most patients (n = 14), total MRI scores were higher than PET scores (higher PET scores, n = 4; equal scores, n = 7; significance of differences, p<0.05).
Serological and clinical parameters
A comparison of each patientś serological and clinical findings of inflammatory process showed significant correlations between BVAS.2 and CRP (rs = 0.698, p<0.001), between BVAS.2 and ESR (rs = 0.707, p<0.001) and between CRP and ESR (rs = 0.514, p<0.01).
Serological and clinical parameters compared with imaging scores
There were no correlations between MRI activity scores and CRP (rs = −0.158, p = 0.45), ESR (rs = −0.232, p = 0.27) or BVAS.2 (rs = −0.064, p = 0.76). Thoracic PET scores showed a weak correlation with serological and clinical parameters (CRP: rs = 0.136, p = 0.52; ESR: rs = 0.320, p = 0.12; BVAS.2: rs = 0.221, p = 0.29). The concordance of “whole-body” PET with CRP (rs = 0.032, p = 0.88), ESR (rs = 0.248, p = 0.23), and BVAS.2 (rs = 0.258, p = 0.21) was similar to that for “thoracic” PET.
Follow-up
Synopsis of imaging findings and clinical data prompted intensified immunosuppressive treatment in 20 of 25 patients (table 1). In 12 patients, results of follow-up MRI (n = 11) and PET (n = 9) could be compared with changes in CRP (from 10 to 6 mg/l), ESR (from 34 to 28 mm/1st h) and BVAS.2 (from 5.7 to 2). Only the course of the thoracic PET activity score correlated significantly with changes in ESR (rs = 0.680, p<0.05). There was a moderate but non-significant correlation between courses of thoracic PET and CRP (rs = 0.540, p = 0.13) and BVAS.2 (rs = 0.553, p = 0.12). Courses of whole-body PET and MRI correlated moderately with ESR (rs = 0.619, p = 0.08 and rs = 0.469, p = 0.15, respectively), CRP (rs = 0.544, p = 0.13 and rs = 0.485, p = 0.13) or BVAS.2 (rs = 0.519, p = 0.15 and rs = 0.193, p = 0.57).
Morphological signs of vasculitis
MRI disclosed signs of large-vessel vasculitis in 17 of 25 patients, and included stenotic lesions of the upper extremity arteries (n = 9) and thickening of the aortic wall ⩾4 mm (n = 12). Aortic aneurysm (transversal diameter 4.2–5.6 mm) was found in three patients. Owing to the limited spatial resolution of PET, only MRI detected these structural vessel lesions.
DISCUSSION
FDG-PET and MRI are useful for the initial diagnosis and assessment of inflammatory aortic arch syndrome in patients with GCA.4–9 Nevertheless, the use of both methods in patients with pre-existing immunosuppressive therapy and complicated disease course has not been previously evaluated.
In the majority of our patients, both PET and MRI detected large-vessel activity, demonstrating that this entity is much more common in patients with GCA than historically has been appreciated.1 However, a selection bias towards severe cases has to be considered in our study. We found that neither MRI nor PET correlated significantly with ESR, CRP or BVAS.2. Correlation between MRI and PET was limited (rs = 0.350, p = 0.086) with MRI providing significantly higher activity scores (fig 1). This finding agrees with data from Scheel et al (2004) that described static MRI findings of aortic inflammation despite improved laboratory parameters during the course of treatment and better correlation between PET and laboratory measures during follow-up.6 Contrarily, Blockmanns et al (2006) found no correlation between vascular FDG uptake and any biochemical parameter.9 Interestingly, a study with findings similar to ours has cast doubt on the utility of MRI in measuring disease activity in Takayasús arteritis.12 Activated arteriosclerosis should be considered as a differential diagnosis, especially in cases of lower extremity involvement.13 Nevertheless, in our study, the limited correlation of “thoracic” PET with serological und clinical variables was similar to “whole-body” PET.
Because we did not evaluate arterial wall biopsies from our patients, we can only speculate as to why disease activity was defined differently by both imaging methods as compared with clinical and serological data. Possibly, persistent neovessels in the aortic wall mimicked continuing inflammation, especially in MRI. Negative findings of acute phase reactants in active GCA have been described, and residual disease activity due to limited suppression of inflammation despite medical treatment must be considered.14 15
In conclusion, PET and MRI are inadequate for assessing disease activity of large-vessel GCA in patients with pre-existing immunosuppressive therapy. However, MRI is valuable for detecting morphological vessel lesions such as aneurysms and stenoses.
REFERENCES
Footnotes
Competing interests: None.