Article Text

Abstract
Objectives: The safety and potential efficacy of rituximab was examined in diffuse cutaneous systemic sclerosis (dc-SSc).
Methods: A 24 week open-label study in which eight patients with dc-SSc received an infusion of 1000 mg rituximab administered at baseline and day 15, together with 100 mg methylprednisolone at each infusion. Assessment included CD19+ peripheral blood lymphocyte number, skin sclerosis score, indices of internal organ functioning, the health assessment questionnaire disability index, the 36-item Short Form health survey and histopathological evaluation of the skin.
Results: Ritixumab induced effective B-cell depletion in all patients (<5 CD19+ cells/μl blood). There was a significant change in skin score at week 24 (p<0.001). Also, significant improvements were measured in the dermal hyalinised collagen content (p = 0.014) and dermal myofibroblast numbers (p = 0.011). Two serious adverse events occurred, which were thought to be unrelated to the rituximab treatment.
Conclusions: Rituximab appears to be well tolerated and may have potential efficacy for skin disease in dc-SSc.
This study is registered with ClinicalTrials.gov, number NCT00379431.
Statistics from Altmetric.com
Diffuse cutaneous systemic sclerosis (dc-SSc) has a poor prognosis. In recent years, clinical trials with B-cell-depleting agents unveiled a role for B lymphocytes in the pathogenesis of several autoimmune diseases. Multiple elements point to a role for B cells in systemic sclerosis (SSc) pathogenesis.1 2 Communications concerning the use of rituximab in this indication are scarce.3 4
In this study, we explored the safety and potential efficacy of B-cell depletion with rituximab in patients with dc-SSc in an open-label trial, using clinical as well as histopathological endpoints. Data on efficacy were only used to generate hypotheses.
Patients and methods
Study design
Rituximab (1000 mg) together with 100 mg methylprednisolone was administered at day 1 and day 15. Skin biopsies were obtained at baseline and at 12 weeks. Indices of internal organ functioning, the health assessment questionnaire disability index (HAQ-DI), the 36-item Short Form health survey (SF-36) were evaluated at weeks 0, 2, 12 and 24. The protocol and patient informed consent forms were approved by the Ethics Committee of Ghent University Hospital.
Study patients
Patients with dc-SSc, fulfilling the American College of Rheumatology preliminary criteria for SSc,5 were screened at Ghent University Hospital.
Inclusion criteria were: age older than 18 years, disease duration (time passed since the first non-Raynaud’s disease manifestation) of 4 years or less, a modified Rodnan skin score (mRSS) of 14 or greater or a disease activity score of 3 or greater.6 Low-dose prednisolone (⩽10 mg/day) was allowed, provided that the patients were on a stable dose at least 12 weeks before inclusion in the trial. All disease-modifying antirheumatic drugs (except methotrexate) were stopped 12 weeks before screening and were replaced by methotrexate 15 mg per week (unless contraindicated). Exclusion criteria were: forced vital capacity 50% or less, a diffusing capacity of the lung for carbon monoxide of 40% or less, echocardiographically assessed left ventricular ejection fraction 40% or less, serious and uncontrolled coexisting diseases, infection, immunodeficiency, or a history of cancer.
Clinical measurements
Primary outcome was skin involvement assessed by the 17-site mRSS (0–3 scale), which was done by the same investigator throughout the study (VS). Lung involvement was assessed by high resolution computed tomography and pulmonary function tests. Cardiac involvement was assessed by echocardiography. Renal function was determined by the estimation of the creatinine clearance with the MDRD formula. All subjects completed the disability index of the HAQ-DI and the SF-36 to evaluate the influence on daily functioning and quality of life.7
Skin histology and histological assessment of skin involvement
Full-thickness skin biopsies (approximately 1.5 cm long and 0.5 cm wide) were surgically obtained at baseline and 12 weeks. Samples taken at 12 weeks were obtained within 1 cm of the original biopsy site. Skin was taken from the dorsal side of the forearm and the inner side of the upper arm. A normal reference set was included in the analysis. This set contained the skin biopsy from the inner upper arm of nine persons who were referred for a lupus band test and in whom further evaluation excluded any specified autoimmune disease.
Blinded Masson’s trichrome and anti-α-smooth muscle actin-stained slides were scored three times by two independent observers (BVdC and JTVP). A score was assigned on a 10-cm visual analogue score scale.8 The average score was used for statistical analysis. The interrater correlations for hyalinised collagen and myofibroblast scores were 0.74 (p<0.01) and 0.86 (p<0.01), respectively. CD20-positive cells were counted in 10 randomly chosen fields (640–860 μm), which were orientated perpendicular to the epidermis.
Biochemistry
Screening for antinuclear antibodies was performed with indirect immunofluorescence on HEp-2000 cells (Immunoconcepts, Sacramento, California, USA) at a 1 : 40 dilution with a FITC-labelled goat anti-human IgG (heavy and light chain). All samples were analysed with INNO-LIA Update (Innogenetics NV, Zwijnaarde, Belgium). Serum anti-RNA polymerase III antibodies (MBL International, Woburn, Massachusetts, USA) and anti-topoisomerase I antibodies (Varelisa, Phadia GmbH, Freiburg, Germany) levels were quantified with a commercial ELISA kit. B-cell depletion was analysed by flowcytometry (FC500, Beckman Coulter, Fullerton, California, USA).
Statistical analysis
Mixed models analyses (MMA) with random intercept and slopes were used to evaluate changes in clinical parameters over time.9 Histological data were analysed by multilevel methods taking into account two levels: time and place of biopsy. For continuous data with normal or nearly normal distribution, MMA was used. Data with more skewed distributions and on–off phenomena were, after dichotomisation, analysed with generalised estimating equations (GEE) and a logit link function. GEE and MMA were calculated without imputation of missing data as these methods are the best way to handle missingness under the assumption of missingness at random.9 Interreader correlation coefficients were calculated using Spearman’s correlation coefficient. Differences between normal and diseased skin were analysed by Mann–Whitney U.tests. All analyses were performed with SPSS 15.0.
Results
Characteristics of the study subjects
Nine patients were screened and eight were included in the trial. The patient characteristics are shown in table 1.
Demographics of the study population
The normal reference set for skin histology included six women and three men. Median age was 38 years (range 16–68).
Safety and tolerability
Two serious adverse events, considered to be probably unrelated to the study drug, occurred. Patient 2 underwent coronary artery bypass surgery just before the 24 week evaluation. The postoperative condition of the patient made the 24 week evaluations impossible. Therefore this patient was excluded from the 24 week evaluation. Patient 3 reported a 2-day low-grade fever occurring 2 weeks after the second infusion of rituximab, for which he was hospitalised. Upon hospitalisation, the fever had spontaneously subsided and no infectious focus could be found. The minor adverse events were: one infectious exacerbation of existing polyposis nasi and initiation of antihypertensive therapy, in patient 1, who had known hypertension; an episode of nausea, after the initiation of rifampycine for prevention of exacerbation of latent tuberculosis (in patient 3), and one episode of non-infusion-related nausea and of depressive mood (in patient 5).
Clinical efficacy
Over 24 weeks the clinical skin score improved from a mean mRSS of 24.8 (SD 3.4) to 14.3 (SD 3.5) (MMA p<0.001), which is a mean percentage improvement of 43%, and from a median of 24.5 to 15, which is a median percentage change of 40%. Parameters of internal organ involvement and functioning remained stable. These are depicted in table 2.
Changes in clinical and laboratory parameters in the study upon treatment with rituximab
Skin histology
The myofibroblast and hyalinised collagen scores could not be determined in one baseline patient sample, as well as in one normal reference sample due to technical reasons.
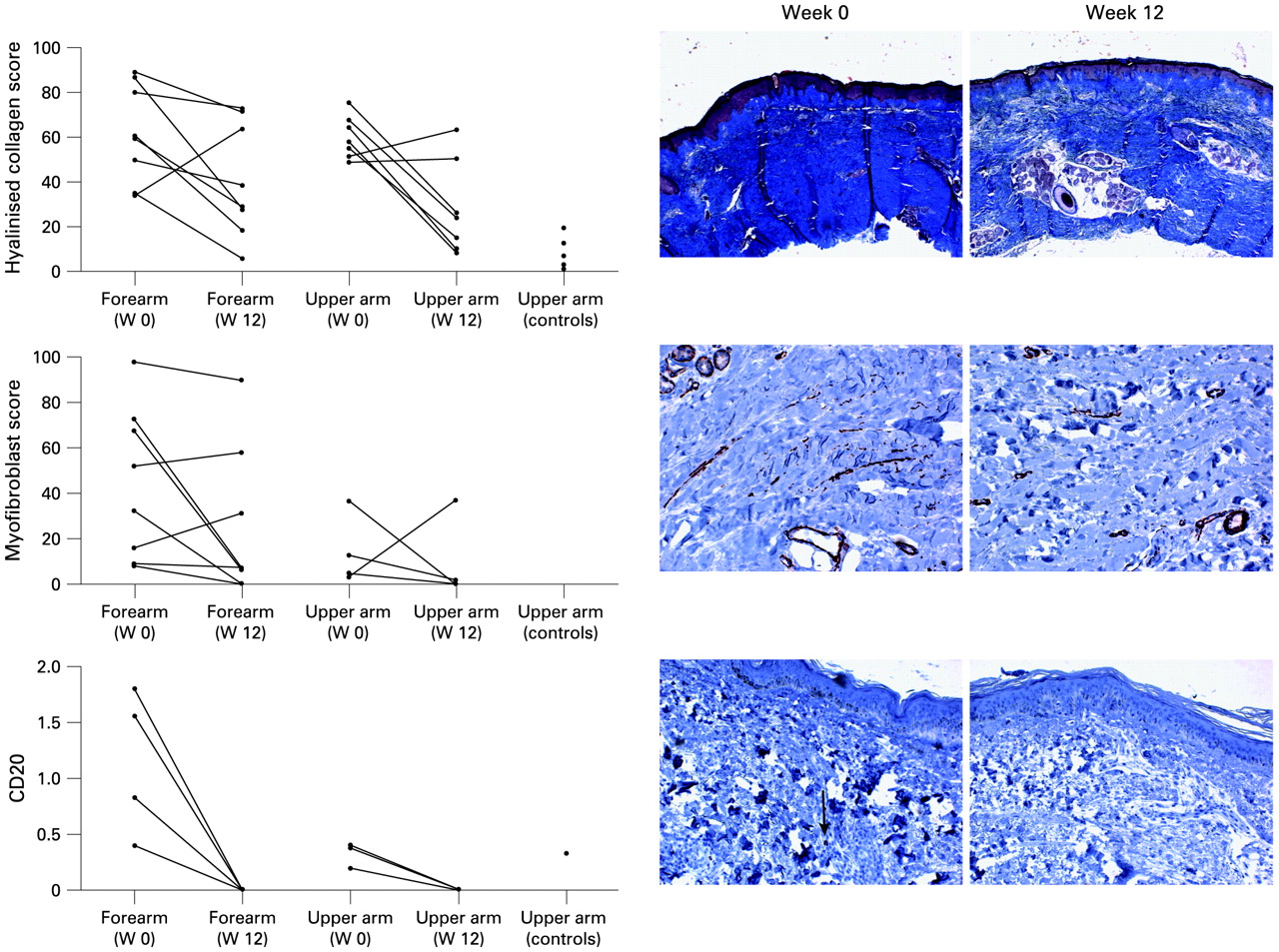
The hyalinised collagen content and myofibroblast positivity were increased in the upper arm of the SSc patients at baseline compared with the normal reference set. The mean hyalinised collagen score was 60 (SD 9.5) versus 7.1 (SD 7.2) (p<0.001). Myofibroblast positivity was 4/7 versus 0/8 (χ2 test p = 0.013).
After treatment, the hyalinised collagen content decreased in the upper arm from 60 (SD 9.5) at baseline to 28 (SD 21) at week 12, and in the forearm from 62 (SD 22) at baseline to 41 (SD 25) at 12 weeks (MMA p = 0.014). Myofibroblast positivity decreased in the upper arm from 4/7 to 2/7 and in the forearm from 8/8 to 6/8 (GEE p = 0.011) (fig 1).
{kind=link}
Hyalinised collagen content (Masson’s trichrome staining, upper panel), myofibroblast score (α-smooth muscle actin staining, middle panel) and lymphocyte numbers (CD20 staining, lower panel) in the skin before and 12 weeks after rituximab treatment. Representative pictures are shown (upper panel original magnification 40×, middle panel original magnification 400×, lower panel original magnification 100×). W, week.
B cells, which were immunostained with an antibody directed against an intracytoplasmatic epitope of the CD20 molecule,10 could be detected at baseline in the dermis of the forearm in four out of eight patients and in the dermis of the upper arm in three out of eight patients. In the normal reference set, B cells were present in one out of nine subjects. After rituximab treatment, in none of the patients could B cells be detected in their dermis (GEE p = 0.03) (fig 1). All eight patients had effective depletion of CD 19+ B cells in the peripheral blood at week 2 (<5 CD19+ lymphocytes/μl). Anti-topoisomerase I and anti-RNA polymerase III antibody titres did not change significantly over the study period.
Discussion
Our trial was a safety study of rituximab in dc-SSc. As the serious adverse events were probably unrelated to the study medication and as we had no other unexpected adverse events, we can state that rituximab was well tolerated. Even though the use of steroids caused no renal crises, one should always consider its potential harmful effects in this patient group.11 12 The skin score dropped 10.5 points at week 24 (mean at baseline was 24.8), which largely exceeds the minimal clinically relevant treatment effect estimate for the skin as provided by a recent Delphi exercise,13 and which is more than can be expected as a spontaneous improvement in patients with similar disease duration.14 This leads us to hypothesise that rituximab may be a potential efficacious drug in the treatment of dc-SSc, although one must emphasise this is an open trial. Encouragingly, blinded histopathological analysis of the skin led us to postulate in the same direction. Parameters of internal organ involvement remained stable, but further follow-up is needed before drawing any conclusions.
Acknowledgments
The continuous commitment of our patients, the excellent feedback of the trial bureau (by Ms Annick Broekaert), the technical assistance of Ms M De Decker, Ms N Degryse, Ms A Herssens and Ms R Heyse is greatly appreciated by the authors.
REFERENCES
Footnotes
The first three authors contributed equally to this work.
J-MN is deceased.
Funding JTVP is supported by a research grant from the Fund for Scientific Research, Flanders. SD is supported by a grant from the Nationale Vereniging voor Steun aan Gehandicapte Personen. BVdC is supported by a postdoctoral grant from the Fund for Scientific Research, Flanders.
Competing interests None.
Ethics approval The protocol and patient informed consent forms were approved by the Ethics Committee of Ghent University Hospital.
Patient consent Obtained.