Article Text

Abstract
Objective: To compare ultrasonography (US) with clinical examination in the detection of entheseal abnormality of the lower limb in patients with spondyloarthropathy (SpA).
Methods: 35 patients with SpA (ankylosing spondylitis 27; psoriatic arthritis 7; reactive arthritis 1) underwent independent clinical and ultrasonographic examination of both lower limbs at five entheseal sites—superior pole and inferior pole of patella, tibial tuberosity, Achilles tendon, and plantar aponeurosis. US was performed using an ATL (Advanced Technology Laboratories, Bothell, Washington, USA) high definition imaging 3000 machine with linear 7–4 MHz and compact linear 10–5 MHz probes to detect bursitis, structure thickness, bony erosion, and enthesophyte (bony spur). An enthesitis score was formulated from these US findings giving a possible maximum total score of 36.
Results: On clinical examination 75/348 (22%) entheseal sites were abnormal and on US examination 195/348 (56%) sites were abnormal. In 19 entheseal sites with bursitis on US, only five were detected by clinical examination. Compared with US, clinical examination had a low sensitivity (22.6%) and moderate specificity (79.7%) for the detection of enthesitis of the lower limbs. There was no significant correlation between the US score of enthesitis and acute phase parameters such as erythrocyte sedimentation rate (ESR) or C reactive protein (CRP). The intraobserver κ value for analysis of all sites was 0.9.
Conclusions: Most entheseal abnormality in SpA is not detected at clinical examination. US is better than clinical examination in the detection of entheseal abnormality of the lower limbs in SpA. A quantitative US score of lower limb enthesitis is proposed but further studies are required to validate it in SpA.
- enthesitis
- ultrasonography
- clinical examination
- spondyloarthropathy
- CRP, C reactive protein
- ESR, erythrocyte sedimentation rate
- GUESS, Glasgow Ultrasound Enthesitis Scoring System
- MRI, magnetic resonance imaging
- SpA, spondyloarthropathy
- US, ultrasound
Statistics from Altmetric.com
- CRP, C reactive protein
- ESR, erythrocyte sedimentation rate
- GUESS, Glasgow Ultrasound Enthesitis Scoring System
- MRI, magnetic resonance imaging
- SpA, spondyloarthropathy
- US, ultrasound
Enthesitis—inflammation of the origin and insertion of ligaments, tendons, aponeuroses, annulus fibrosis, and joint capsules—is a widely accepted clinical, histopathological, and imaging feature of spondyloarthropathy (SpA). Inflammation may occur at any enthesis in SpA, though it is most common in the entheses of the lower limbs.1,2 Pathological examination of enthesitis in SpA demonstrates local inflammation, fibrosis, erosion, and ossification.3,4 Bursitis and synovitis may also occur adjacent to the entheses, and it has been recently postulated that the enthesis may be the initial site of joint inflammation in SpA.5,6
The assessment of enthesitis in SpA is predominantly performed by eliciting tenderness at the enthesis.7,8 An enthesitis index of tenderness assessed at 66 entheseal insertions correlates with pain and stiffness scores in SpA but is time consuming with poor interobserver reliability.7 Histological examination of the enthesis is the potential “gold standard” for evaluation of enthesitis but is rarely obtained owing to ethical and practical constraints. Plain radiography, ultrasound (US) and magnetic resonance imaging (MRI) demonstrate soft tissue thickening, cortical bone breakage, new bone proliferation, and bone structure alterations at inflamed entheses9–11 and allow quantification of enthesitis. Radiological scoring of the progression of enthesitis in SpA has principally focused on plain radiography of the spine.12 MRI is useful in the evaluation of enthesitis but is limited by its availability and expense.6 The resolution of MRI for superficial structures is not better than US, which achieves 200–450 μm in-plane resolution at 10 MHz insonation frequency.13
Musculoskeletal US is widely available, inexpensive, and readily demonstrates superficial tissue inflammation such as fluid collections, soft tissue lesions, and bone surface lesions with a sensitivity comparable to MRI.14,15 Three studies of US of the lower limbs in SpA suggest a discrepancy between clinical and sonographic enthesitis. These studies do not provide an exact description of the different imaging features of enthesitis such as erosion, enthesophyte, and thickness of tendon, ligament or aponeurosis nor do they report intraobserver variability or specificity and sensitivity of the relative examination techniques.10,16,17
The application of US in rheumatology may be limited by a lack of standardised techniques and protocols and the time required to examine multiple sites. In SpA the commonest sites of enthesitis are the knee, heel, and ischial tuberosity.18 As the ultrasonographic features of the normal ischial tuberosity have not been described, US examination was limited to the entheses of the knee and heel using a standard midline, or long axis in the case of the plantar aponeurosis (which is not a midline structure), plane for US examination, selecting structures for which a normal definition and thickness had been previously described.19–22 US examination was more sensitive and specific than clinical examination in the detection of enthesitis of the lower limbs in SpA and may provide a more objective and reliable index of enthesitis than clinical examination.
PATIENTS AND METHODS
Patients
Patients satisfying the European Spondylarthropathy Study Group criteria for the diagnosis of SpA23 were assessed during routine presentation to the rheumatology outpatient clinic. Patients with previous joint surgery of the knee and ankle, corticosteroid injection of the structures examined within the previous six weeks, or peripheral neuropathy of the lower limbs were excluded from the study.
Clinical examination
The superior pole of the patella (quadriceps tendon insertion), the inferior pole of the patella (patellar ligament origin), the patellar ligament insertion at the tibial tuberosity, the Achilles tendon, and the plantar aponeurosis were examined in both lower limbs of each patient. Clinical examination for tenderness and swelling at each site was performed by an experienced rheumatologist.
Ultrasound evaluation
Real time ultrasonography was performed by an experienced rheumatologist trained in musculoskeletal ultrasonography, using an ATL HDI 3000 machine with linear 7–4 MHz and compact linear 10–5 MHz probes. The linear 7–4 MHz probe was used for detecting suprapatellar bursitis as it allows deeper penetration when a large effusion is present and was preferred for imaging of the plantar aponeurosis. The clinical examination and US measurements were performed separately; one immediately after the other, by different investigators who were unaware of each other's results. The sonographer did not know the clinical details of the patients. Examination of the superior pole of the patella (quadriceps tendon insertion), the inferior pole of the patella (patellar ligament origin), and the patellar ligament insertion at the tibial tuberosity was performed with the patient in the supine position with the knee flexed at 30 degrees. The Achilles tendon and the plantar aponeurosis were examined with the patient lying prone with the feet hanging over the edge of the examination table at 90 degrees of flexion. If the patient was unable to lie prone, the heels were examined with the patient lying supine and the knees and ankles flexed at 90 degrees.
Ultrasonographic assessment of structure thickness and the presence or absence of bony erosion, enthesophyte, and bursitis was recorded at each site. Bursitis was defined as a well circumscribed, localised anechoic or hypoechoic area at the site of an anatomical bursa and which was compressible by the transducer. Bursal dimensions were obtained in the long and short axis with a normal bursa being <2 mm in the short axis.24 Bony erosion was defined as a cortical breakage with a step down contour defect and an enthesophyte was defined as a step up bony prominence at the end of the normal bone contour. Ligament, aponeurosis, and tendon thickness were measured at the point of maximal thickness proximal to the bony insertion. The following criteria were used for abnormal structure thickness: quadriceps tendon thickness ≥6.1 mm,19 proximal and distal patellar ligament ≥4 mm,20 Achilles tendon ≥5.29 mm,21 plantar aponeurosis ≥4.4 mm.22 In this study only thickened enthesis, fluid collection, erosion, and bony spur were accepted as US signs of enthesitis. “Hypoechoic oedema” without any thickness change was excluded, as it is a subjective sign of enthesitis. No control group was selected in this study as the normal ultrasound features and dimensions of the structures examined have already been described.19–22 To reduce subjectivity further the threshold of abnormal thickness was set 0.1 mm above the reported standard deviation of each site in the normal population.
An ultrasonographic score of lower limb enthesitis was calculated as follows: one point was scored for each abnormality at each site examined, giving a possible maximum total score of 36 (box 1). The US score was also calculated separately as a soft tissue score and as a bone score. The soft tissue score included entheseal thickness and bursitis. The bone score included erosions and enthesophytes. Interobserver error was not measured in this study, but we have already demonstrated a high degree of intraobserver repeatability and interobserver reproducibility of US measurements of ligament thickness.25 Sonographic images were stored on magneto-optical disks for offline analysis. After three months, the investigator rescored every patient to calculate intraobserver reliability.
Box 1 Glasgow Ultrasound Enthesitis Scoring System (GUESS)
Superior pole of the patella—quadriceps tendon enthesis
-
Quadriceps tendon thickness ≥6.1 mm
-
Suprapatellar bursitis
-
Superior pole of patella erosion
-
Superior pole of patella enthesophyte
Inferior pole of the patella—proximal patellar ligament enthesis
-
Patellar ligament thickness ≥4 mm
-
Inferior pole of patella erosion
-
Inferior pole of patella enthesophyte
Tibial tuberosity—distal patellar ligament enthesis
-
Patellar ligament thickness ≥4 mm
-
Infrapatellar bursitis
-
Tibial tuberosity erosion
-
Tibial tuberosity enthesophyte
Superior pole of the calcaneus—Achilles tendon enthesis
-
Achilles tendon thickness ≥5.29 mm
-
Retrocalcaneal bursitis
-
Posterior pole of calcaneus erosion
-
Posterior pole of calcaneus enthesophyte
Inferior pole of the calcaneus—plantar aponeurosis enthesis
-
Plantar aponeurosis thickness ≥4.4 mm
-
Inferior pole of calcaneus erosion
-
Inferior pole of calcaneus enthesophyte
Each item scores one point. Total possible score on both lower limbs is 36.
Statistical analysis
All values are given as mean (median) (standard deviation). Statistical analysis was performed using Statview software. A p value <0.05 was deemed significant. Intraobserver agreement was calculated using a κ test. Sensitivity, specificity, negative and positive predictive value, false negative and false positive rates of clinical examination were also calculated.
RESULTS
Patient characteristics
Thirty five patients (25 male, 10 female) were examined (ankylosing spondylitis 27; psoriatic arthritis 7; reactive arthritis 1). The patients had a mean age of 48 (median 49.3) (SD 14), mean age of disease onset of 20.8 (median 19) (SD 13.1) years and a mean duration of disease of 24.9 (median 21) (SD 10.4) years. The mean erythrocyte sedimentation rate (ESR) was 16.2 (median 10) (SD 18) mm/1st h and the mean C reactive protein (CRP) was 18 (median 6) (SD 20.8) mg/l. Six (17%) patients had a family history of spondyloarthropathy, 14 (40%) had previous uveitis, 21 (60%) had peripheral joint disease, one (3%) had inflammatory bowel disease, nine (26%) had psoriasis, and two (6%) had joint replacement surgery not affecting the lower limbs. Twenty four (69%) patients were HLA-B27 positive, three (9%) were negative, and the HLA status of eight (23%) was not known.
Clinical examination
A total of 350 entheseal sites were examined (10 sites×35 patients) clinically, of which, 71/350 (20%) entheseal sites were tender and 13/350 (4%) entheseal sites were swollen. Table 1 gives the clinical findings at individual sites. On clinical examination 61.7% of entheses were symmetrically involved.
Ultrasonographic and clinical examination of the entheseal insertions at five lower limb entheses
Ultrasonographic examination
A total of 350 entheseal sites were examined by US. Two sites were obscured by overlying psoriatic plaques (one over the inferior pole of the patella and one over the tibial tuberosity in two separate patients) and are not included in the analysis. Table 1 gives the ultrasound findings at individual sites. On US examination 195/348 (56%) entheses were abnormal and 54% of the entheses were symmetrically involved. Figure 1 shows the ultrasonographic features of the five normal entheseal sites and fig 2 the ultrasonographic features of enthesitis. The intraobserver κ value for analysis of all sites was 0.9. κ Values for analysis of the separate lesions were (bony erosion κ=0.97, bursitis κ=1.00, enthesophyte κ=0.83) and for analysis of separated locations were (superior pole of the patella κ=0.92, inferior pole of the patella κ=0.7, tibial tuberosity κ=0.82, superior pole of the calcaneus κ=0.97, inferior pole of the calcaneus κ=0.8).

Normal ultrasonographic appearance on lower limb entheseal insertions. (A) Quadriceps tendon enthesis: PR, proximal; DI, distal; S, skin; Q, quadriceps tendon; P, patella; *, tendon attachment. (B) Proximal patellar ligament enthesis: PR, proximal; DI, distal; S, skin; L, patellar ligament; P, patella; H, Hoffa fat pad; F, femur; *, ligament attachment. (C) Distal patellar ligament enthesis: PR, proximal; DI, distal; S, skin; L, patellar ligament; H, Hoffa fat pad; T, tibia; *, ligament attachment. (D) Achilles enthesis: PR, proximal; DI, distal; S, skin; A, Achilles tendon; C, calcaneus; K, Kager fat pad; *, tendon attachment. (E) Plantar aponeurosis enthesis: PO, posterior; AN, anterior; S, skin; A, plantar aponeurosis; C, calcaneus; H, heel fat pad; *, aponeurosis attachment.

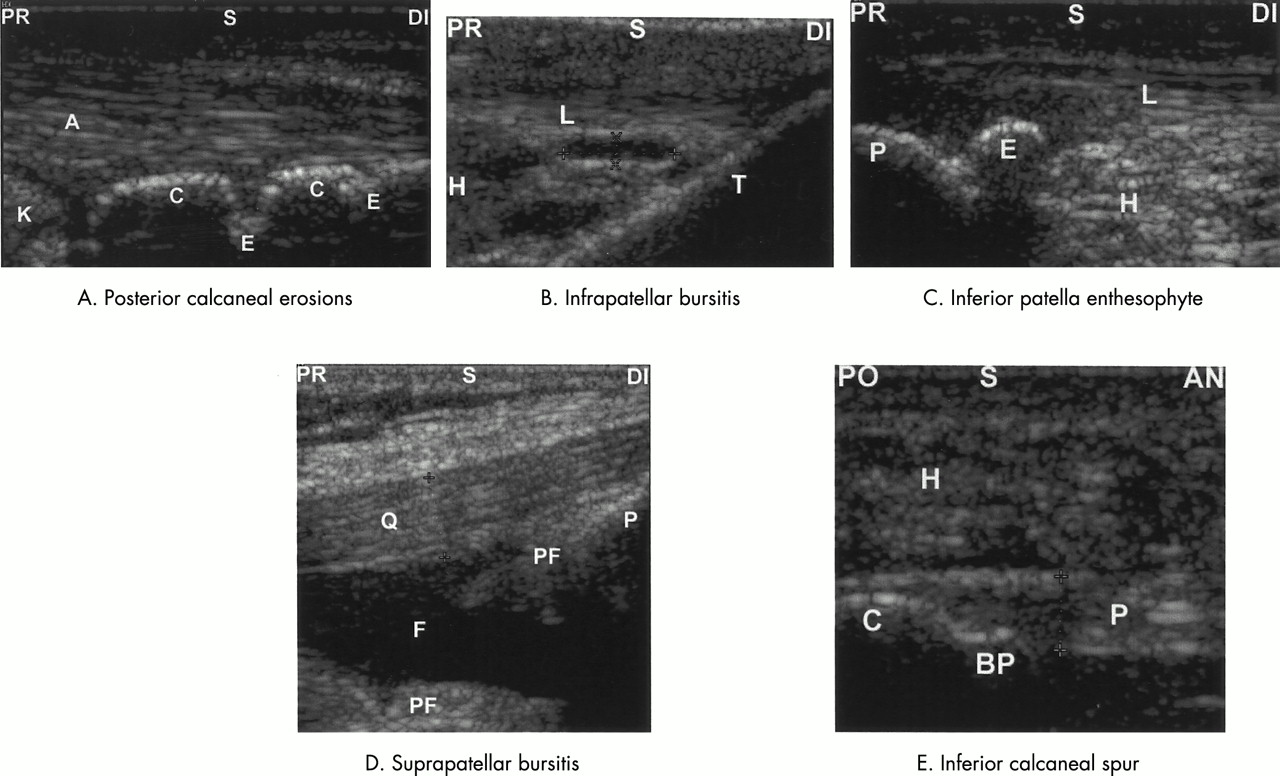
Ultrasonographic appearances of lower limb enthesitis. (A) Posterior calcaneal erosions: PR, proximal; DI, distal; S, skin; A, Achilles tendon; K, Kager fat pad; C, calcaneus; E, erosion. For comparison with the normal image see fig 1D. (B) Infrapatellar bursitis: PR, proximal; DI, distal; S, skin; L, patellar ligament; T, tibia; H, Hoffa fat pad; the crosses mark infrapatellar bursa. For comparison with the normal image see fig 1C. (C) Inferior patella enthesophyte: PR, proximal; DI, distal; S, skin; L, patellar ligament; P, patella; H, Hoffa fat pad; E, enthesophyte. For comparison with the normal image see fig 1B. (D) Suprapatellar bursitis: PR, proximal; DI, distal; S, skin; Q, quadriceps tendon; F, fluid collection in the suprapatellar bursa; P, patella; PF, perifemoral fat. For comparison with the normal image see fig 1A. (E) Inferior calcaneal spur: PO, posterior; AN, anterior; S, skin; P, plantar aponeurosis; C, calcaneus; H, heel fat pad; BP, bony spur. For comparison with the normal image see fig 1E.
Relationship of clinical and ultrasonographic findings in the lower limb entheses
Entheseal abnormality was detected by US in 195/348 (56%) entheseal sites and by clinical examination in 75/348 (22%) sites. Figure 3 shows the relationship between clinical and ultrasonographic findings at individual sites.

{kind=link}
{kind=link}
{kind=link}
Correlation of clinical abnormality (either swollen or tender) with any US abnormality at entheseal sites in the lower limbs. SP, superior pole of the patella; IP, inferior pole of the patella; TT, tibial tuberosity; SC, superior pole of the calcaneus; IC, inferior pole of the calcaneus.
Table 2 gives the sensitivity, specificity, negative and positive predictive value, false negative and false positive rate of clinical examination. Compared with US, clinical examination had a low sensitivity (22.6%) and moderate specificity (79.7%) for the detection of enthesitis of the lower limbs.
Clinical examination versus US as the “gold standard”. Data showing sensitivity, specificity, false positive (FPR) and false negative rate (FNR), positive (PPV) and negative predictive value (NPR). Results are shown as percentages
Ultrasonographic score of enthesitis
To quantify lower limb enthesitis a US score of enthesitis was formulated. A maximum of 36 was possible in each patient. The mean score was 6.9 (median 6) (SD 4.3) with a soft tissue US abnormality score of 5 (median 4) (SD 2.8) and a bone (erosion or/and enthesophyte) US score of 1.9 (median 2) (SD 1.8). There was no significant correlation between the US score of enthesitis and the ESR or CRP.
Clinically detected and undetected bursitis
There was no correlation between the sizes of the bursae on US and clinical findings and only 5/19 bursa were clinically detected. Two large bursae were detected clinically but two equally large bursae were not detected by clinical examination. No bursa under 13.8×4.7 mm was detected on clinical examination.
DISCUSSION
On clinical examination, 75/348 (22%) entheseal insertions were determined to be inflamed, which is similar to a previous study of calcaneal entheses.26 Lehtinen et al noted less clinical enthesitis in lower limbs in SpA (56/372 (15%)),10 which may reflect differences between the two patient groups. The presence of tenderness was more sensitive than swelling in the detection of enthesitis, being present at 14–28% of entheseal sites while swelling was present at 0–14% of entheseal sites. US detected enthesitis at 51.4–63.8% of entheseal sites and was more sensitive than clinical examination for tenderness and swelling taken together or separately. If US is taken as the gold standard, neither tenderness nor swelling was specific in the detection of enthesitis, with just 44/75 clinically inflamed entheses confirmed by US. Some of these sites might have had minor degrees of inflammation not amenable to detection on US. Possibly, certain features of enthesopathy such as plantar spur were overestimated as they may be found in normal subjects, though the presence of erosion and bursitis at the enthesis is relatively specific. In this study, swelling was not a useful sign in detecting enthesitis at the tibial tuberosity or plantar aponeurosis.
Two principal features of soft tissue inflammation—tendon thickening and bursitis—were examined on ultrasonography. To reduce the subjectivity of previous studies of enthesitis in SpA, tendon thickness was determined using standardised US views according to previously published protocols. In addition, the threshold of normal tendon thickness was set at 0.1 mm above the reported standard deviation above the mean as measured in normal populations. We have already demonstrated a high degree of intraobserver repeatability and interobserver reproducibility of US measurements of ligament thickness.25 Increased tendon or ligament thickness was the most common feature of soft tissue inflammation, being present at 20–57% of entheses examined. This study may underestimate enthesitis as it did not include hypoechoic changes in tendons or ligaments, which are an important but subjective feature of enthesitis and may be influenced by transducer position,27 particularly when parallel fibrils change their directions as is the case at the entheses. Tendon thickening may be due to either oedema or fibrosis, and longitudinal studies are required to assess its reversibility. Significant qualitative and quantitative ultrasonographic changes were demonstrated in a case study of Achilles tendonitis and retrocalcaneal bursitis followed up for one year,28 whereas Lehtinen et al found no reduction in the frequency of ultrasonographic enthesitis in a six month follow up of 23 patients.16 Bursitis was present at 4–13% of sites examined, being most common at the suprapatellar and retrocalcaneal sites.
Enthesophyte formation was the most common US bony abnormality, being present at 3–30% of entheseal sites while bony erosion was present at 1–13% of sites. This is in keeping with previous radiological studies of SpA where entheseal ossification is a common feature. In addition to entheseal ossification, US also demonstrated intratendinous and interligamentous calcifications adjacent to the point of entheseal insertion. These may represent the end stage of inflammation or may relate to other pathology such as trauma or degenerative changes which are common in the general population. Erosive changes at the enthesis may have been underestimated owing to the presence of an enthesophyte which obscures adjacent erosions on US. Clinical examination is not useful in determining the presence of these bony lesions and does not provide this potentially diagnostic information.
This study confirms that there is considerable subclinical enthesitis in SpA, which can be objectively measured by US using standardised protocols. At present, only clinical evidence of enthesitis of the heels is included in the European Spondylarthropathy Study Group preliminary classification criteria for the diagnosis of SpA,23 and clinical enthesitis is included in the preliminary core sets to be used as end points in clinical trials in ankylosing spondylitis.29 US detection of enthesitis is more sensitive and more specific than clinical examination and soft tissue US has a high degree of reproducibility. Ultrasonography is now widely practised by rheumatologists and should be used to define classification criteria and outcome measures in SpA.
Although established treatments of SpA have not been proved to reduce spinal entheseal manifestations of disease,30 newer treatments such as anti-tumour necrosis factor have been shown to reduce spinal entheseal inflammation.31,32 Studies of treatments specifically targeting entheseal inflammation will need objective measures of peripheral enthesitis to confirm efficacy. Plain radiography is limited in that established scores12 provide little information about soft tissue inflammation, which is most amenable to treatment. MRI and US have similar sensitivity in demonstrating superficial soft tissue and bony surface abnormality.14,15 US does not detect insertional bone oedema, but the significance of this lesion is not yet determined in SpA and bone oedema may also co-exist in overuse syndrome with enthesopathy.33
By using a limited series of easily reproducible, fixed reference points and established normal parameters we devised an enthesitis score of the lower limbs: GUESS, which can be applied to the evaluation of treatments in SpA. US did not correlate with systemic parameters of disease activity in SpA (as it does in rheumatoid arthritis34), though these are less sensitive markers of disease activity in SpA.35 Ultrasonographic assessment is more time consuming than clinical examination but can be reliably performed in 15 minutes by an experienced musculoskeletal ultrasonographer. Further multicentre studies of GUESS in the assessment of enthesitis are required.