Article Text

Abstract
Objectives To establish reference intervals (RIs) for spinal mobility measures as recommended for patients with axial spondyloarthritis, and to determine the effect of age, height and gender on spinal mobility, in normal individuals.
Methods A cross-sectional study (MOBILITY) was conducted among normal individuals aged 20–69 years. Recruitment was stratified by gender, age (10-year categories) and height (10 cm categories). Eleven spinal mobility measures were assessed. Age specific RIs and percentiles were derived for each measure.
Results 393 volunteers were included. All spinal mobility measures decreased with increasing age. Therefore, age specific RIs were developed. The 95% RIs (2.5th and 97.5th percentiles), as well as the 5th, 10th, 25th, 50th, 75th and 90th percentiles for each spinal mobility measure and different ages are presented. Mobility percentile curves were also plotted for each of the measures. For instance, the 95% RI for lateral spinal flexion was 16.2–28.0 cm for a 25-year-old subject, 13.2–25.0 cm for a 45-year-old subject and 10.1–21.9 cm for a 65-year-old subject. After adjustment for age, there was no need for gender specific RIs, while RIs of some measures are height-adjusted.
Conclusions Age specific RIs and percentiles were derived for each of the spinal mobility measures for normal individuals. These may guide clinicians when assessing the mobility of patients with axial spondyloarthritis. The RIs may serve as cut-off levels for ‘normal’ versus ‘abnormal’, whereas the mobility percentile curves may be used to assess the level of mobility of patients with axial spondyloarthritis.
- spondyloarthritis
- outcomes research
- epidemiology
Statistics from Altmetric.com
Introduction
Axial spondyloarthritis (SpA) is a chronic rheumatic disease that comprises both non-radiographic axial SpA and radiographic axial SpA, the latter known as ankylosing spondylitis (AS). The natural history of axial SpA (axSpA) is associated with a progressive restriction in spinal mobility, a hallmark of the disease.1 Restriction in spinal mobility is one of the most commonly used outcome measures in axSpA follow-up and treatment studies2 ,3 and is, at the same time, a predictor of poor long-term prognosis.2 The importance of spinal mobility in the follow-up of patients with axSpA is also emphasised by its inclusion in the core set of domains that have been defined by the Assessment of SpondyloArthritis international Society (ASAS).4
Throughout the last decades spinal mobility has been measured by numerous techniques in patients with AS.5–13 Efforts have been made to homogenise these measures and to identify the most clinically relevant. A composite score was developed, the Bath AS Metrology Index (BASMI), including five measures.14 Subsequently, clinically relevant spinal mobility measures were identified and recommendations were made on assessment in a standardised way for patients with axSpA as incorporated in the ASAS core set.4 ,14 ,15
Several studies have been performed among normal individuals with the aim of describing the normal range of spinal movements, and also of identifying factors associated with mobility.5–9 ,12 ,13 From these studies, it is known that spinal mobility decreases with age6 ,8 ,9 and also that there are some differences in spinal mobility with respect to gender.6 However, the ASAS recommends (slightly) different mobility measures than those previously tested in normal individuals. Consequently, knowledge is lacking on how the ASAS recommended mobility measures behave in normal individuals, which hampers the interpretation of spinal mobility among patients with axSpA. The behaviour of measures in normal individuals is usually established through the determination of reference intervals (RIs). These are commonly used in medical practice for determining unusual or extreme measurements, the premise being that if an individual's value is outside the interval, further clinical investigation may be required. To construct RIs, a reference sample assumed to consist of ‘normal’ individuals is needed.16 ,17
The aim of the present study was to derive RIs of spinal mobility measures among normal individuals, assessed as recommended by the ASAS. In order to adequately derive RIs, we first assessed the effect of demographic factors such as age, height, weight and gender on each spinal mobility measure.
Methods
Study population
A cross-sectional study, MOBILITY, was conducted, aiming at including 400 participants. Participants were recruited at the hospital, universities and also among contacts in the Netherlands and Portugal. Recruitment was stratified for age (10-year categories), height (10 cm categories) and gender in order to guarantee a balanced distribution of these factors in the population, to better take into account their influence on spinal mobility and to enable derivation of more precise estimates for extreme groups (of height or of age), compared to what would occur with a random sample. Female participants were assigned to one of four groups, according to their height: ≤160 cm; 161–170 cm; 171–180 cm; and >180 cm. For male participants, the cut-offs were 10 cm higher, taking into account that men are on average taller than women. According to their age, participants were divided into the following groups: 20–29, 30–39, 40–49, 50–59 and 60–69 years. Across age, height and gender, there were 40 groups, each with 10 individuals. The sample size of 400 participants was mainly based on considerations of convenience, and the requirement that we would like to have at least 10 participants per stratum. Any volunteer agreeing to participate, aged 20–69 years and Caucasian, was a candidate for the study. Exclusion criteria were: (1) history of back surgery; (2) low back pain within the last 3 months that required medical attention; (3) known inflammatory rheumatic disease, osteoporosis, Paget disease or severe osteoarthritis of the spine or hips; (4) more than 3 months’ pregnancy; (5) important scoliosis; (6) symptomatic vertebral disc disease at the moment of the evaluation; (7) hip arthroplasty or any known hip disease; and (8) hypermobility syndrome (defined as ≥4 Beighton criteria, which were tested in each participant).18 All participants gave their informed consent. The study was evaluated by the Ethics Committee of the Maastricht University Medical Center. No formal approval by the Committee was needed, because normal individuals were included and no intervention took place.
Spinal mobility measures
Eleven measurements of spinal mobility were performed (measures marked with an asterisk according to the ASAS recommendations15), in the following order: tragus-to-wall distance* (TTW), occiput-to-wall distance* (OTW), lateral spinal flexion* (ASAS-LSF), LSF according to the INSPIRE method,19 chest expansion (CE), 10 cm Schober test* (10ST), 15 cm Schober test (15ST),5 internal hip rotation (IHR),20 intermalleolar distance* (IMD), cervical rotation lying and cervical rotation sitting*. The best of two tries for each measurement was recorded. All measurements were recorded in centimetres, except for cervical rotation (both lying and sitting) which were recorded in degrees. All measurements were rounded to decimals, except for IHR, IMD and cervical rotation (both lying and sitting) which were rounded to units. For more details on the measurements, see online supplementary text 1.
The BASMI14 was calculated and its performance was analysed in normal individuals. The range of the BASMI is from 0 to 10; the higher the score, the worse the mobility. The formula of the BASMI linear was used to compute the score,21 and two versions of the score were calculated: BASMI-original14 and BASMI-modified.15 BASMI-original includes TTW, ASAS-LSF, IMD, 15ST and cervical rotation in the lying position. BASMI-modified15 includes two changes: cervical rotation is measured in the sitting position instead of the lying position, and the 15ST is substituted by the 10ST.
Spinal mobility measurements were performed by two assessors (SR and CS). The first 100 volunteers were measured by both assessors and their mobility measurements were averaged. After reliability analyses (see online supplementary table S1 and figure S1), agreement between both was considered adequate and each of the assessors proceeded with independently measuring different participants.
Statistical analysis
Descriptive statistics (mean, median, SD, range) and box-plots were used to describe the overall distribution of mobility measurements across age, height and gender categories. Comparison of mobility measurements between groups (eg, women vs men) was performed using t-tests or the Mann–Whitney test, as appropriate. Comparison between more than two groups was performed through one-way analysis of variance or the Kruskal–Wallis test, as appropriate. In case of a significant difference between the multiple groups, post hoc analyses were performed to determine significant between-group changes.
The association between age, gender, height and each of the spinal mobility measures was investigated through linear regression, adjusted for weight when considered relevant. Univariable followed by multivariable analysis was performed, with forward selection; interactions were also tested. This analysis was intended to identify factors influencing spinal mobility that would eventually need to be taken into account in development of the RIs.
Development of age specific RIs
Typically, an RI is defined by the range between two centile values, centred around the median on the probability scale. Standard limits commonly used are the 2.5th and 97.5th percentiles, which correspond to a 95% RI. An extensive description of the methods used to define the age specific RIs is provided in the online supplementary text 2. In summary, to define RIs, a parametric regression method based on fractional polynomials was used.16 Age specific 2.5th, 5th, 10th, 25th, 50th, 75th, 90th and 97.5th percentile curves were calculated. RIs were derived, adjusted for height, gender and weight, where deemed necessary, that is, when this adjustment improved substantially the fit of the data; otherwise, the models for the development of the RIs were kept as simple as possible, which also contributes to their more feasible application in practice. Stata SE V.12 was used.
Results
A total of 393 participants were included in the study. All the age, height and gender categories were complete, except for the category of women aged 60–69 years and >180 cm, due to difficulties in finding eligible volunteers. The descriptive statistics of all measures are presented in table 1. In general, the values are reasonably spread, which reflects the variation in spinal mobility that occurs among normal individuals. Surprisingly, no subject had a BASMI of 0. The lowest BASMI-modified value found in an individual was 0.18; the mean value of all normal individuals was 1.83. Of the five component scores of the BASMI-modified, the 10ST was the one with the highest mean (3.4, SD 1.4), and thus contributing most to the impossibility of achieving a BASMI of 0. This was followed by cervical rotation (1.9, SD 1.2). The component score with the lowest average was the TTW (1.1, SD 0.4).
Characteristics of the spinal measurements in normal individuals (aged 20–69 years, men and women)
Effect of age, gender and height on spinal mobility
Details of each of the spinal mobility measures stratified for age categories, gender or height categories, and corresponding comparisons across categories, are outlined in online supplementary tables and figures S2, S3, S4A and S4B, respectively. The relationship between these factors and each of the spinal mobility measures is summarised in table 2. A significant decrease in all spinal mobility measures was found with increasing age. For example, an increase of 10 years was associated with a decrease of 1.5 cm in ASAS-LSF. Age was therefore included in all multivariable models. The last column of table 2 presents our (subjective) judgement on the clinical relevance of the effect based on the magnitude of the effect size. The age effect was considered clinically relevant for almost all the measures.
Effect of age, gender and height on spinal mobility measures
Height was associated with TTW, ASAS-LSF, CE, IMD and IHR, with a higher height being associated with better mobility. For example, every increase in height of 10 cm resulted in an increase in IMD of 4.3 cm (men) or 5.6 cm (women). The effect of height on TTW and ASAS-LSF was not considered clinically relevant.
Gender was associated with some of the spinal mobility measures. Female gender was associated with lower values of CE and cervical rotation sitting, but higher values of IHR.
Age (and height) specific RIs
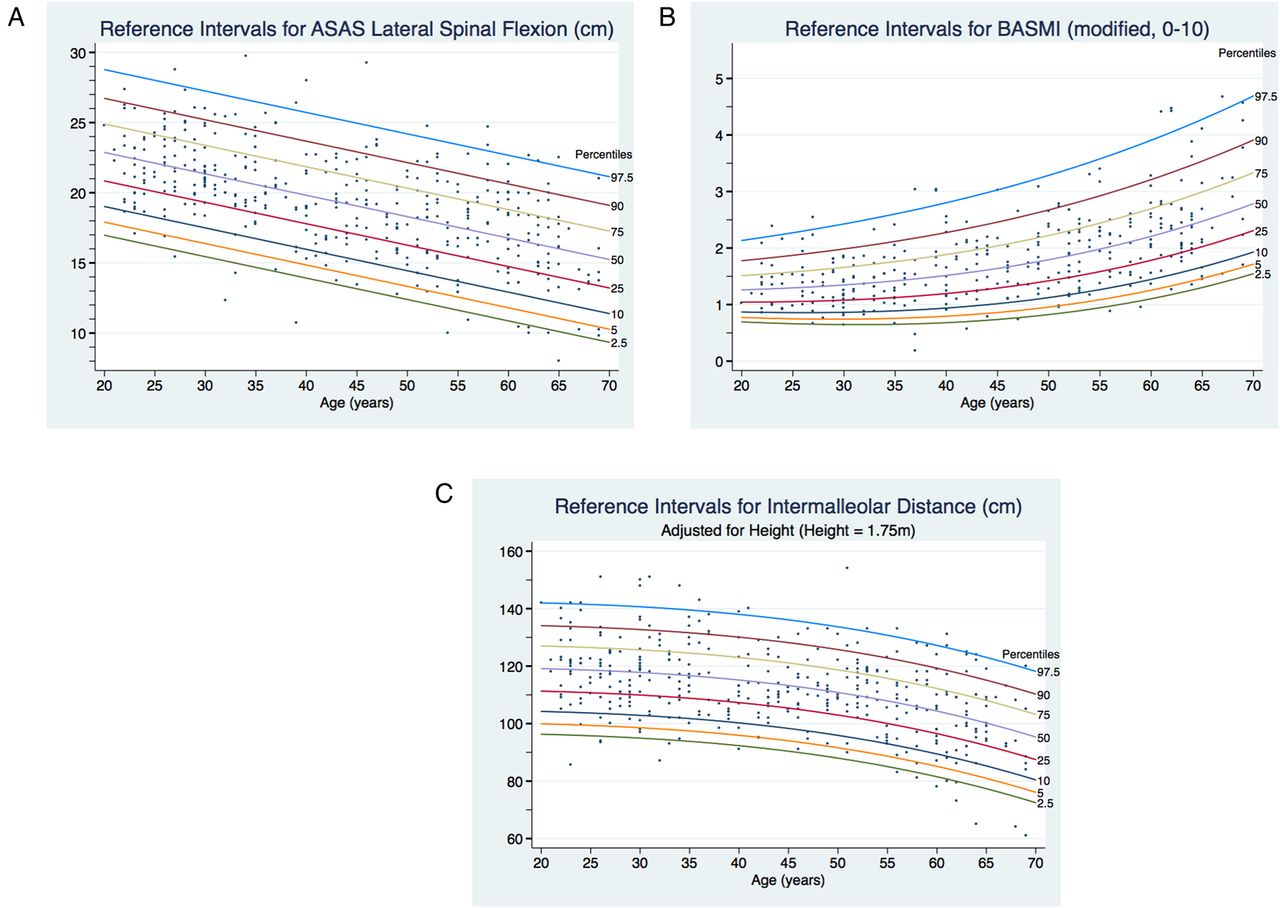
For the development of RIs, an equation best fitting the data was derived for each of the measures (see online supplementary table S5). From those equations, RIs can be computed for any age, and examples were chosen for ages at 10-year intervals (25, 35, 45, 55 and 65 years old). For some measures, namely CE, IMD and IHR, age and height specific percentiles were derived, as these fitted the data best because height influenced those measures. Gender and weight were not taken into account when deriving the RIs, as, after adjustment for age (and in some cases for height), they did not substantially contribute to improve the fit of the models. Age (and height) specific percentiles for each of the measures are presented in table 3. For instance, for a 25-year-old person the 2.5th percentile for ASAS-LSF was 16.2 cm, which means that 2.5% of the participants had a result below this value. The corresponding 95% RI was 16.2–28.0 cm.
Reference intervals for spinal mobility measures
The corresponding percentile curves were derived and are presented in figure 1, and in more detail and in online supplementary figure S5. For the measures for which an adjustment for height was made, RIs were derived for the mean height (175 cm) (table 3); further calculations for other heights (160 cm and 185 cm) are presented in the online supplementary table and figure S6. A potential non-linear relationship between age and spinal mobility measures was taken into account and accommodated when deriving the age-specific percentiles. For measures whose distribution deviated from normal (ie, Gaussian), that is, cervical rotation lying, 10ST, BASMI-original, BASMI-modified, percentile curves were derived through an extended model accommodating the skewness of the data. The relationship between the spinal mobility measure and age was non-linear for the cases of cervical rotation lying, IMD, BASMI-original and BASMI-modified. In these cases, the impairment in mobility with increasing age is even clearer, especially above the age of 50.

{kind=link}
Reference intervals and percentile curves for lateral spinal flexion, BASMI and intermalleolar distance, all measured as recommended by ASAS; (A) lateral spinal flexion; (B) BASMI; (C) intermalleolar distance (measure dependent on height, and here curves are presented for the mean height, height=175 cm). Reference intervals for other spinal mobility measures can be found in online supplementary figures S5 and S6 (in the latter are the different curves for different heights for measures dependent on height). ASAS, Assessment of Spondyloarthritis international Society; BASMI, Bath Ankylosing Spondylitis Metrology Index.
All 10-year age group graphs for all measures can be found at http://www.asas-group.org.
Discussion
In the present study, age (and in some cases height) specific RIs and also different percentile curves have been derived in normal individuals for the different spinal mobility measures currently used in patients with axSpA. This is, to our knowledge, the first study defining RIs for these measures, in which two trained assessors have performed all the measures in a systematic approach and including all ASAS recommended measures.
A wide range of values was found for all spinal mobility measures. This emphasises the variation of mobility across participants, even among normal individuals from a sample in which any subject in whom an ‘abnormal’ spinal mobility could be expected was excluded following the rigorous eligibility criteria. Surprisingly, no subject had a BASMI value of zero, and being a sample composed of normal individuals, it seems that it is technically (almost) impossible to have a BASMI score of zero.
An important age effect was found on all spinal mobility measures. This is in line with previous studies.6–9 Nevertheless, the effect is so striking that we consider it deserves to be emphasised. When following patients with axSpA throughout time, this age effect on spinal mobility should be taken into account as it might, to some extent, explain a potential impairment in mobility developing, which should likely not be completely attributed to the disease.
Comparison between the results of our study and of previous studies performed in normal individuals is hampered by several factors, such as different recruitment strategies, inclusion criteria and mobility measurement techniques. Furthermore, no other study developed RIs, so we can only compare sample or subgroup mean values. Our values for 10ST lie in between those previously reported.8 ,9 Moll et al6 described values of 15ST across age categories very similar to ours. In another study, CE values were slightly lower than ours.7 A more recent study among 20–29-year-old Turkish men (n = 1982) reported slightly lower values for CE and higher values for 10ST and 15ST.22 Our study seems to be unique in the recruitment stratified for age, height and gender, in order to obtain a sample in which these factors are balanced. Despite the fact that no reference values had been previously defined, a 5 cm cut-off for the 10ST is frequently used in clinical practice. Several of the participants included in our study had a 10ST below this cut-off, and for some age categories, even the average (and median) value was below this cut-off. This finding should be integrated into clinical practice, so that a value below 5 cm is not necessarily considered abnormal.
Age specific RIs and percentiles were derived for each of the spinal mobility measures for normal individuals. For some measures (ie, CE, IMD and IHR), age and height specific RIs and percentiles were derived. The derivation of the RIs confirmed the previous findings of the regression analysis (table 2), and only for these measures was it necessary to adjust the RI for height. For measures dependent on height, the mean height has been used to derive the RI presented in this paper, but in case of a patient with an ‘extreme’ height, appropriate mobility curves (see online supplementary appendices) can be used. Despite the fact that gender and weight were associated with some of the mobility measures, they did not seem to have an additional contributory effect to explaining spinal mobility values, compared to age (and in some cases also height), and were therefore not taken into account when deriving the RIs.
The development of RIs for a given measure is common practice in other areas.17 These RIs may guide clinicians when assessing the mobility of patients with axSpA. These measures are not diagnostic tests (ie, to diagnose a patient with axSpA on the basis of an ‘abnormal mobility’). The RIs and percentile curves can be of use in the assessment of patients with axSpA, in a similar approach to use of the reference values for dual-energy X-ray absorptiometry bone mineral density assessments as recommended by the WHO23 ,24 or the use of growth curves for monitoring children's growth.25 In practice, it may be of value to assess a patient rigorously when he starts deviating from his ‘personal curve’. This hypothesis needs to be further investigated, but looks to be a promising use of these mobility curves.
The RIs and percentiles may also serve as cut-off levels for ‘normal’ versus ‘abnormal’. For that purpose, the lowest percentiles are the most important, as they are the ones that may define an important impairment in spinal mobility; therefore more percentiles (ie, 2.5th, 5th, 10th, 25th) are presented in the lower range. The cut-off used for the definition of ‘abnormal’ depends on how specific we want to be. If we want to be specific we can use the lowest cut-off, that is, the 2.5th percentile, which is also the lowest border of the 95% RI, and label only those patients with definitely abnormal spinal mobility. If we want to be sensitive, and identify all the cases with ‘potentially abnormal spinal mobility’, then we will choose a higher cut-off (eg, 10th or 25th percentile). The ultimate definition of such a cut-off should be based on evidence and should have some prognostic value, which needs to be assessed in further research, having these proposed percentiles as a reference.
Some limitations of the present study should be addressed. The sample size is relatively small. Nevertheless, the stratified recruitment gave the study a higher power. Although it is not certain to what extent these results are generalisable to other populations, we do not expect large differences. We accepted any volunteer, but the eligibility criteria—which focused on factors eventually affecting spinal mobility—were strictly assessed to ensure we would have a population composed of individuals with normal spinal mobility. A factor potentially influencing spinal mobility that was not taken into account was each subject's level of physical activity. However, it is a difficult factor to measure, especially by self-report. Furthermore, RIs are usually derived as being only age-specific and not taking many other factors into account, mainly because of feasibility purposes of their application. The study sample was restricted to Caucasians, which may limit the generalisability of the findings. Nevertheless, this was preferred, in order to control for another factor eventually influencing spinal mobility. Strengths of the study are the solid methodology used for the statistical analysis (analogous to the methodology used for the development of the growth curves by the WHO25); having a homogeneous sample in terms of factors influencing mobility (especially age and height, but also gender) and also a population of normal individuals; having two well-trained observers assessing a quarter of the participants with good reliability; and including all ASAS recommended mobility measures.
In summary, age (and height) specific RIs and percentiles were derived for each of the spinal mobility measures for normal individuals. These RIs may help clinicians when assessing the mobility of patients with axSpA.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online appendix
Footnotes
Handling editor Tore K Kvien
Contributors SR, AvT, DvdH and RL designed the study. SR and CS collected the data. SR, AvT, PR, DvdH and RL analysed the data and critically interpreted the results. SR prepared the first version of the manuscript. All authors reviewed the draft versions and gave their approval of the final version of the manuscript.
Competing interests None.
Funding SR was supported by the Fundação para a Ciência e Tecnologia (FCT) grant SFRH/BD/68684/2010.
Patient consent Obtained.
Ethics approval The study was evaluated by the Ethics Committee of the Maastricht University Medical Center. No formal approval by the Committee was needed, because normal individuals were included and no intervention took place.
Provenance and peer review Not commissioned; externally peer reviewed.