Article Text

Abstract
Objective A systematic review and meta-analysis of data from cohort studies to analyse the diagnostic performances (ie, sensitivity and specificity) of ultrasound (US) for diagnosis of calcium pyrophosphate deposition (CPPD) disease with microscopic crystal detection used as a gold standard.
Methods We performed a systematic review of articles published up to December 2014 using EMBASE, MEDLINE and Cochrane databases and abstracts from the past two EULAR and ACR annual meetings. Only studies reporting the performance of US for diagnosis of CPPD disease were selected. A meta-analysis involved the inverse variance method to evaluate global sensitivity and specificity of US. Statistical heterogeneity was assessed by the Cochran Q-test and I2 values.
Results The search resulted in 85 articles and 11 abstracts; 17 and 4, respectively, were selected for the systematic review. A total of 262 patients with CPPD disease and 335 controls from 4 original articles and 4 abstracts were included in the meta-analysis. The US diagnostic patterns most frequently recorded were thin hyperechoic bands in the hyaline cartilage (8 articles); hyperechoic spots in fibrous cartilage or in tendons (7 articles); and homogeneous hyperechoic nodules localised in bursa or articular recesses (4 articles). The meta-analysis revealed a heterogeneity of the data, with a sensitivity of 87.9% (95% CI 80.9% to 94.9%) and specificity of 91.5% (95% CI 85.5% to 97.5%) using a random model.
Conclusions This meta-analysis confirmed that US has high sensitivity and specificity for the diagnosis of CPPD and may be a promising tool for the diagnosis and management of CPPD.
- Ultrasonography
- Chondrocalcinosis
- Synovial fluid
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Ultrasound has a high diagnostic performance for CPPD.
What does this study add?
This study pooled all original articles and abstracts currently available to accurately evaluate this diagnostic performance.
How might this impact on clinical practice?
The results might encourage rheumatologists to incorporate ultrasound in the diagnostic process of CPPD.
Introduction
Calcium pyrophosphate deposition (CPPD) disease is one of the two main crystal-related arthropathies associated with gout and one of the most common inflammatory joint diseases.1 It involves the formation of chronic or acute calcium pyrophosphate crystals in joints, fibrous cartilage, tendons or bursa/recesses. Recognised risk factors are ageing, osteoarthritis (OA), previous joint trauma/injury, metabolic disease (haemochromatosis, hyperparathyroidism, hypomagnesaemia) and familial predisposition.1 The clinical presentation can vary, from asymptomatic to chronic or acute arthritis, frequently associated with OA. Since both acute and chronic CPPD disease can mimic with other severe arthritis such as septic arthritis and rheumatoid arthritis (RA), a precise diagnostic is of capital importance.
CPPD is definitively diagnosed by microscopy identification of characteristic calcium pyrophosphate crystals and was retained in the McCarty criteria for diagnosis of CPPD.2 However, synovial fluid aspiration or synovial biopsy is sometimes difficult to perform, especially with small joints. Therefore, assessment of imaging techniques to diagnose CPPD can be useful. Although X-rays remain widely prescribed by rheumatologists, they are not of great diagnostic value.3
Ultrasound (US) has been widely used in daily rheumatology practice for more than 10 years and was recently evaluated in CPPD.4 However, the role of US in the diagnostic and management of CPPD is not well established. The European League Against Rheumatism (EULAR) CPPD task force recommended routine use of US for CPPD diagnosis, and the sensitivity and specificity seemed excellent and possibly better than those of conventional X-rays.5
This study aimed therefore to review the published literature for evidence for US as a diagnostic tool in CPPD, with a focus on validity, reproducibility and feasibility.
Methods
Search method
We performed a systematic review of English articles published up to 31 December 2014 in MEDLINE (via PubMed), EMBASE and Cochrane databases and in the abstracts accepted in the 2013 and 2014 EULAR and American College of Rheumatology annual meetings. Keywords included ‘chondrocalcinosis’, ‘calcium pyrophosphate’, ‘calcium pyrophosphate deposition’, ‘calcium pyrophosphate dihydrate crystal deposition disease’, ‘ultrasonography’, ‘ultrasonography Doppler’, ‘ultrasound imaging’, ‘ultrasonography interventional’ (additional details of the keywords used are in online supplementary figure S1). Studies were included in the systematic review if they used US to scan patients with CPPD and if CPPD was diagnosed by fulfilling the McCarthy criteria or by crystal microscopy or X-rays. We excluded case reports, concise reports, review articles and letters to the editor that were purely commentary or non-human studies. We first screened abstracts and then chose relevant full-text articles. The reference lists of selected articles were manually searched to identify additional relevant reports.
Data extraction
Articles were reviewed independently by two investigators (EG and GM). Then the following information was extracted by use of a predefined data collection form: number of participants, patient characteristics, control group characteristics, follow-up duration, evaluation criteria and main findings. The following methodological features were collected: diagnostic values, US patterns observed, US methodology, comparison with other imaging techniques and reliability. Methodological quality was assessed by the QUADAS tool.6 Disagreements in quality assessment were resolved by consensus by the two investigators. We attempted to contact authors for missing data.
Statistical analysis
All diagnostic studies with microscopy crystal identification as the gold standard were included in the meta-analysis. The diagnosis had to be at the patient level. The primary criteria were the sensitivity (Se) and specificity (Sp) of US for diagnosis of CPPD. These quantitative assessments were estimated for each study included in the meta-analysis. Statistical heterogeneity among selected studies was tested by the Q-test (χ2), with a significance level of 0.05, and reported with the I2 statistic, with high values indicating high heterogeneity. If heterogeneity was rejected, all meta-analysis involved the inverse variance approach (fixed effects model); otherwise, the inverse variance corrected by the interstudy variability was used (random effects model). This method was not relevant for our question because of 100% values for specificity and/or sensitivity. In this case, a correction λ was introduced in the variance calculation:  which allowed for a common weighted Se/Sp estimation with a 95% CI taking into account the weight of different samples. Se/Sp and 95% CIs are shown by forest plots. All computations were performed using R software (R version 2.12.2 (2012-10-26) with the package meta and the function metaprop. The p value <0.05 was considered statistically significant.
which allowed for a common weighted Se/Sp estimation with a 95% CI taking into account the weight of different samples. Se/Sp and 95% CIs are shown by forest plots. All computations were performed using R software (R version 2.12.2 (2012-10-26) with the package meta and the function metaprop. The p value <0.05 was considered statistically significant.
Results
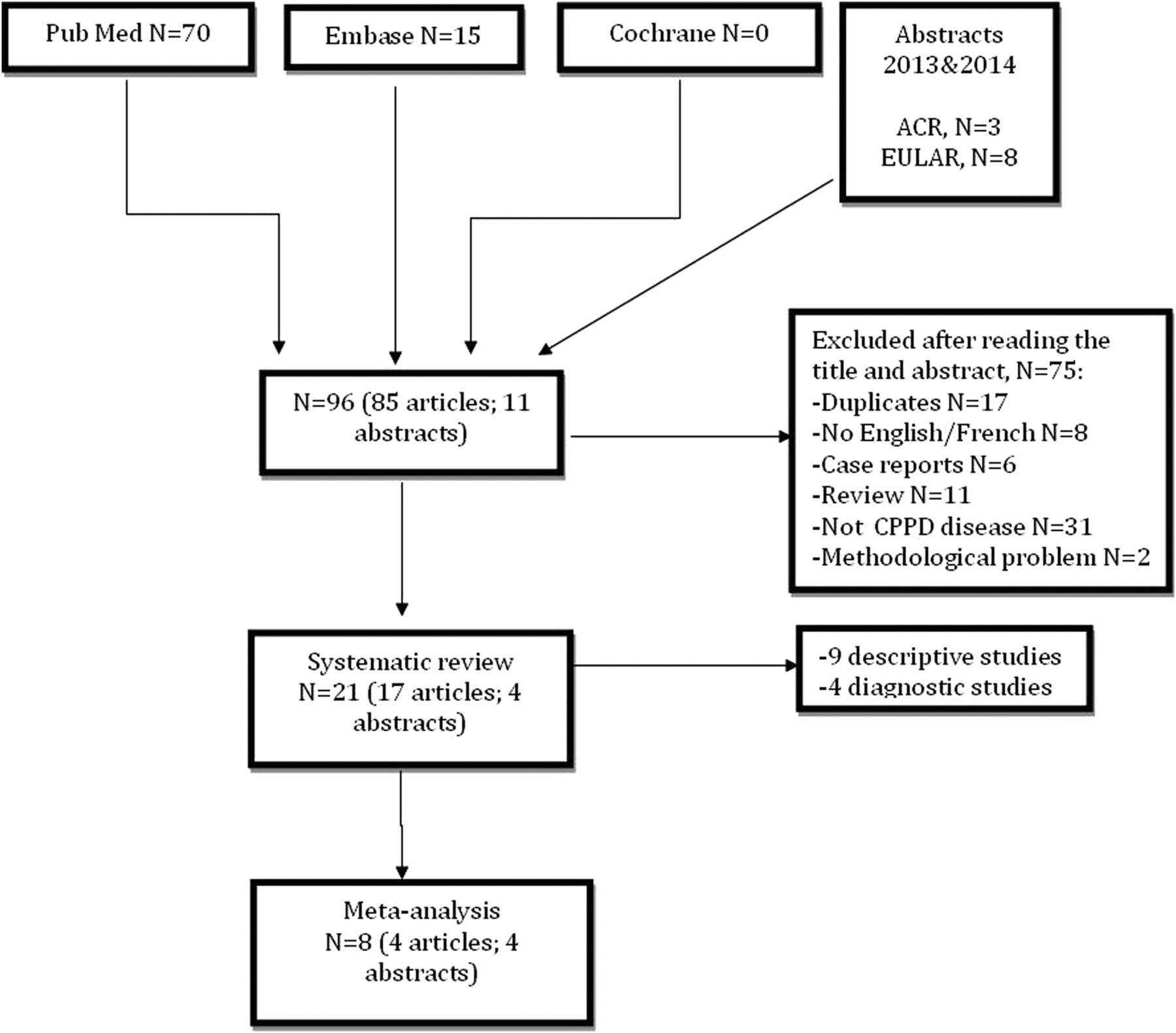
We identified 85 articles in PubMed or EMBASE and 11 abstracts from the past two rheumatology meetings (figure 1); 17 reports of original articles and 4 abstracts were included in the systematic review (9 descriptive studies,5–14 12 diagnostic studies15–26) (table 1). The meta-analysis involved four original articles15–17 ,20 and four abstracts.23–26 Table 2 provides information on the body region imaged, type of probe and Doppler specification. The pathological patterns studied by US included hyaline cartilage, fibrous cartilage or tendons, and bursa or articular recesses (table 3). Only four reports (19%) described the reproducibility of the imaging technique.
Systematic review of 21 studies of ultrasonography for diagnosis of CPPD
Description of imaged region and US techniques for investigating CPPD by study
Summary of diagnosis studies detailing US imaging in CPPD separated by type of pattern

Flow chart of the selection of the articles (CPPD, calcium pyrophosphate deposition).
Diagnostic values and meta-analysis
Among the 12 diagnostic studies15–26 (8 original articles and 4 abstracts), all but one19 used microscopy observation as the gold standard; 9 of 11 used microscopy crystal identification and 2 of 11 used the McCarthy criteria that included microscopy identification.2 Among the 11 studies, 9 used arthrocentesis15–18 ,20–21 ,23–24 ,26 and 2 meniscal operating pieces.22 ,25 The articular sites studied were mostly knees (10 articles) as well as elbows (1 article), shoulders (1 article), wrists (2 articles) and feet (2 articles). The age of patients ranged from 49 to 74 years, and the proportion of males ranged from 29% to 71%. The mean disease duration was described in four studies and ranged from 3.9 to 7.2 years. As previously described,7 the US patterns evaluated were thin hyperechoic bands in the hyaline cartilage (9 articles); hyperechoic spots in fibrous cartilage or in tendons (11 articles) and homogeneous hyperechoic nodules localised in bursa or articular recesses (4 articles). The sensitivity ranged from 15.8%18 to 100%24 and specificity from 38.9%23 to 100%.17 One study compared US with synovial fluid analysis (with meniscal biopsy as a gold standard).25 Six studies compared X-ray and US.17–18 ,20–21 ,24 ,26 One study compared in the same patients the diagnostic values of different patterns.20
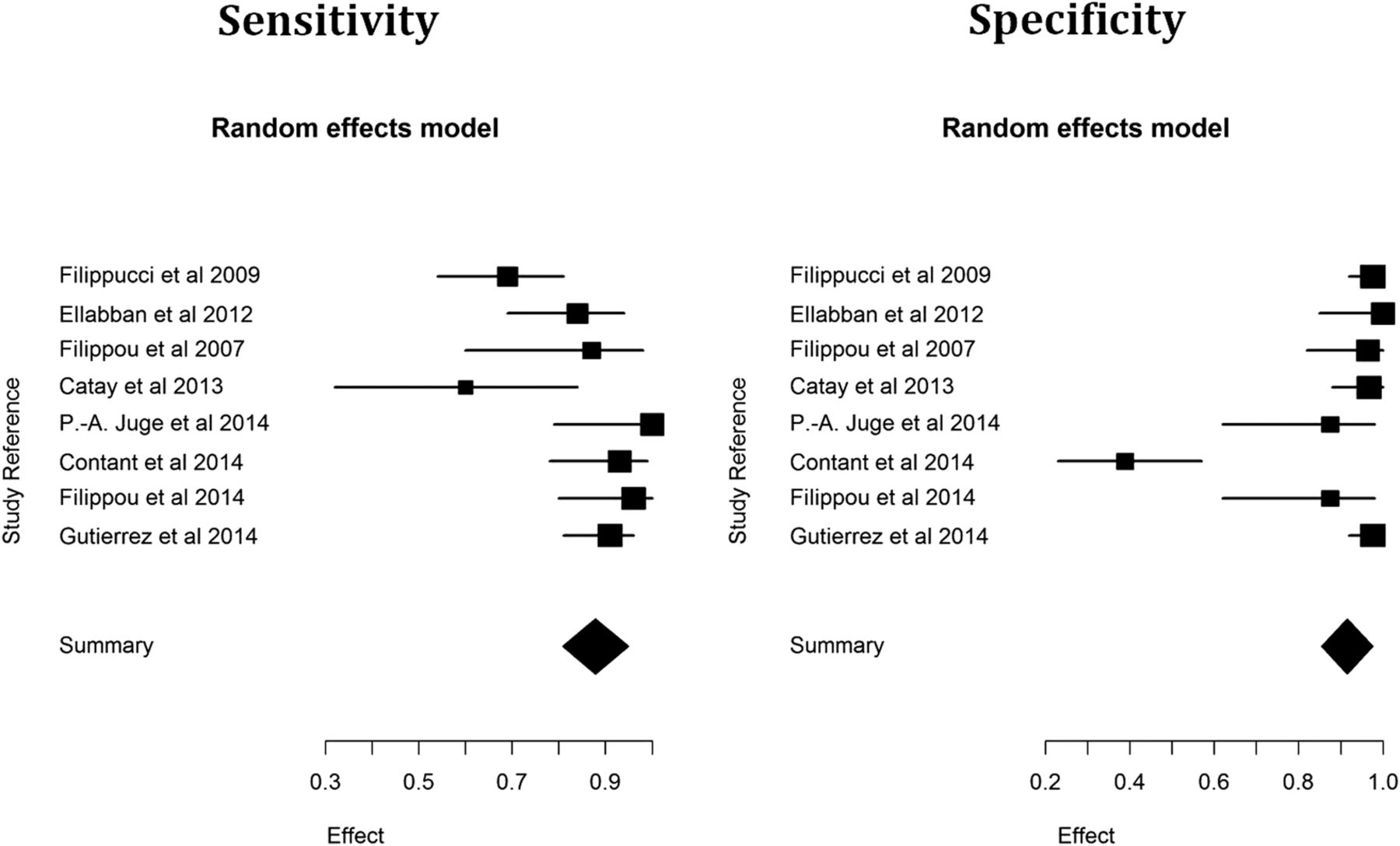
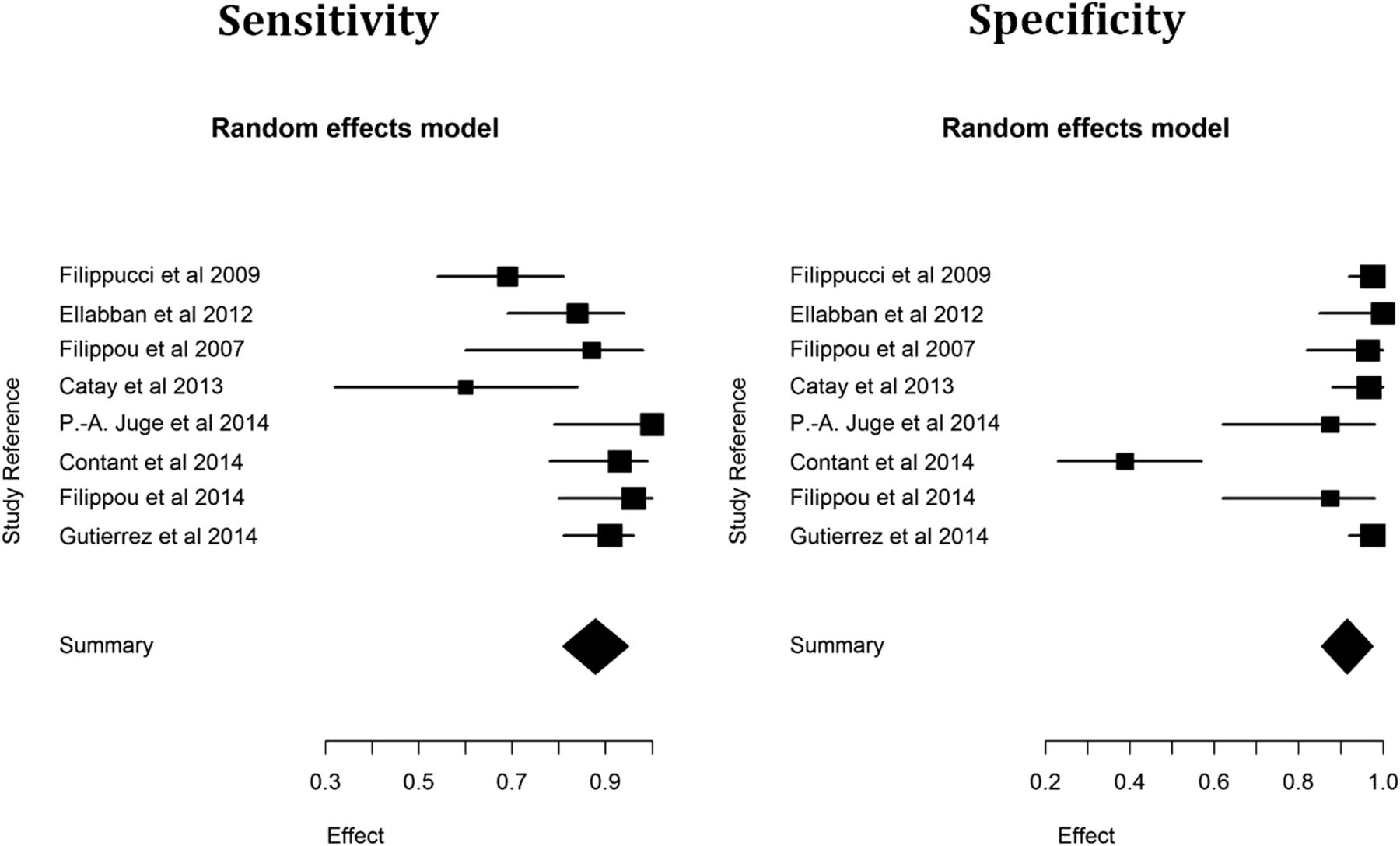
For the 12 diagnostic studies, 4 were excluded from the meta-analysis: 1 used X-ray as the gold standard,19 2 focused on the periarticular structure (plantar fascia and Achilles tendon)18 ,21 but used another joint (the knee) as the gold standard for the diagnosis, and 1 was not designed at the patient level.22 The meta-analysis, based on 262 patients and 335 controls, with a fixed effects model revealed a sensitivity of 91% (95% CI 87.6 to 94.4%, I2=72.4%) and specificity of 96.6% (95% CI 94.7 to 98.4%, I2=87.24%) (figure 2) and, with a random effects model, 87.9% (95% CI 80.9 to 94.9%) and 91.5% (95% CI 85.5 to 97.5%), respectively.
{kind=link}
{kind=link}
Sensitivity and specificity of cohort studies of ultrasonography used for investigating calcium pyrophosphate deposition disease included in the meta-analysis.
Patterns observed
Hyaline cartilage
Table 3 provides details of diagnostic studies focusing on hyaline cartilage. The number of descriptive and diagnostic studies found were equal (n=9 each). CPDD was described as thin intrahyaline hyperechoic bands parallel to the surface of the cartilage, with monosodium urate deposition observed on the cartilage surface. Calcifications within the cartilage usually do not have a posterior shadow because linear CPPD crystal deposits do not have sufficient compactness to stop the US beam progression. The range of possible expression ranged from isolated hyperchoic spots to extended deposits, which might involve a wide portion of the hyaline cartilage. This pattern was described mainly in the femoral hyaline cartilage of the knee. The prevalence of intrahyaline calcifications in two studies ranged from 0%17 for the wrist to 30.7%16 for the knee; the sensitivity of this pattern for diagnosis ranged from 59.5%20 to 68.7%15 and specificity from 96.4%20 to 97.6%15 (table 3). Nevertheless, a recent study8 described the correlation of in vivo presence of CPPD on the cartilage surface and a hyperechogenic line by US that could be mistaken for urate deposit and lead to false-negative results.
Fibrous cartilage or tendons
Table 3 provides details of diagnostic studies focusing on fibrous cartilages or tendons in CPPD. Most of the studies found involved diagnosis (n=11) and fewer were descriptive studies (n=9). CPDD in these sites was the most frequently reported sonographic feature and was described as a ‘punctuate’ pattern composed of several thin hyperechoic spots more common in fibrous cartilage and in tendons. These aggregates appeared as hyperechoic rounded or amorphous-shaped areas. Calcification of tendons in CPPD disease is typically linear and extensive and might generate an acoustic shadow. This pattern was described mainly in the knee meniscus. Two articles studied this pattern only in the Achilles tendon and plantar fascia.18 ,21 The prevalence of fibrous cartilage calcifications in three studies ranged from 56.3%17 for the wrist to 100%16 for the knee; the sensitivity ranged from 57.9%21 to 90.5%20 and specificity from 96%18 to 100%.21 Sensitivity was lower when considering the plantar fascia and Achilles tendon (15.8% and 57.9%, respectively).
Bursa or articular recesses
Table 3 provides details of diagnostic studies of bursa or articular recess calcification in CPPD. The homogeneous hyperechoic nodular or oval deposits localised in bursa and articular recesses (frequently mobile) were typically uniformly rounded in shape with sharply defined margins and could be easily distinguished from joint debris. This pattern was described in only 4 of 12 diagnostic articles or abstracts. In two studies, the prevalence of this pattern ranged from 23.7%16 to 29.4%19 in both knees.
Comparison with other imaging techniques
Seven studies5 ,17–18 ,20–21 ,24 ,26 compared X-ray and US (table 4). The sensitivity was at least as equal as with X-ray and the δ difference ranged from 0%18 to 71%17 in favour of US in those seven studies. Regarding specificity, the values were mainly equal,17–18 ,21 slightly inferior in one study,20 and superior in three others.5 ,24 ,26 One study5 compared US, X-ray and CT in a cohort of patients with CPPD, without controls, and found that US was the most powerful imaging technique to diagnose CPPD, with a strong sensitivity of 100%.
Studies comparing US with other imaging techniques
Site distribution and extent of CPPD deposits
Only one study deals with the extent and site distributions.12 Filippou et al12 proposed a semiquantitative score (0–3) for the extent of CPPD deposits in each examined site and investigated the number of joints affected in CPPD. The mean involvement was 4.7 sites per patient and the knee was the most affected site, followed by the wrist, the Achilles tendon and metacarpophalangeal joints (at least one site affected in 41, 37, 23 and 4 of 42 patients, respectively). The highest mean values of the score were for the menisci, followed by the hyaline cartilage of femoral condyles and the calcaneal entheses.
Reliability
Four studies12 ,15 ,20 ,24 evaluated interobserver reliability, assessed by rereading stored global images. In two studies, the experience of the two ultrasonographers differed.15 ,20 Interobserver reliability was moderate to good: κ values for hyaline cartilage ranged from 0.5515 to 0.8124 and for fibrous cartilage from 0.6820 to 1.0.12 Reproducibility was evaluated in three studies15 ,20 ,24 and ranged from 87%24 to 91.4%.20
Responsiveness
None of the analysed papers dealt with responsiveness.
Discussion
Our report is the first systematic review with meta-analysis to examine diagnostic performances of US in CPPD. Although its incidence and prevalence remain unclear, CPPD is a frequent disease with currently no real pharmacological option to address the crystal formation and dissolution.27 Since the clinical presentation of CPPD can vary and can mimic other rheumatic diseases, its detection relies on the accuracy of the imaging technique used. US has growing importance in the field of rheumatology and specifically in crystal-related arthropathies. After an exhaustive search of the scientific literature, we found several studies of the diagnostic value of US in CPPD, but they included a small number of patients and controls. The meta-analysis allowed us to pool these studies and improve the power.
CPPD patterns are often detected by US, which appears to be valid in detecting hyperechoic bands in hyaline cartilage and hyperechoic spots in fibrous cartilage or in tendons and bursa with histology used as the gold standard. Not surprisingly, the most frequently reported pattern was hyperechoic spots in fibrous cartilage or tendons but with a large range of sensitivity and specificity depending on the examined site. Except for two studies focusing on plantar fascia and Achilles tendon,18 ,21 this research alone was very efficient. We have few data on US of bursa. As expected, the sensitivity and specificity obtained with the meta-analysis are very high and confirm that US may be a valid tool to diagnose CPPD. This good performance may result from evaluation of a combination of several patterns and several sites during the same examination. Yet a proper number of joint sites to examine when CPPD is suspected remains to be determined, despite there being no correlation between clinical presentation of CPPD (acute/chronic/asymptomatic) and the number of sites involved.12
Unfortunately, few studies compared US with different imaging techniques such as CT scan, MRI or even X-ray for the diagnostics of CPPD disease, but US appears at least as equal as X-ray in specificity and sensitivity. In one study,5 US even seemed to be the best imaging tool to diagnose CPPD as compared with X-rays or CT.
When reported, the reliability appeared to be moderate to good despite a difference in the experience of sonographers. The responsiveness of US has not been reported, but it is difficult to evaluate because of the lack of specific and efficient treatment. Moreover, it has not been evaluated with other imaging techniques. The power doppler may be useful in detecting the inflammatory activity of CPPD and was frequently used but was never precisely described.
Some limitations should be acknowledged: first, the number of studies of US for CPPD is limited, particularly as compared with US in RA or even gout. The number of patients in the selected studies was often few and the comparators used differed (inflammatory disease, OA, asymptomatic). To evaluate this limitation, we used the QUADAS tool. Overall, the quality of the studies was satisfactory with a QUADAS score varying from 8.5 to 13.5, the base value being 14. None of the studies reported the feasibility of US imaging in CPPD; however, US practicality is considered acceptable relative to other imaging techniques. Since these US lesions are of potential diagnostic utility, defining, standardising and validating US lesions thought to be specific to CPPD are likely to be of clinical benefit, similar to the Outcomes Measures in Rheumatology (OMERACT) US definitions for RA. The biggest issues are still related to the reliability of the technique and the number of joints to scan, since the time required for evaluating multiple joints or lesions can be long. The standardisation of the description of what is considered a US-detected CPPD lesion may better facilitate the development of US as an outcome tool for the diagnosis and monitoring of the disease. Nevertheless, ultrasound is only an indirect approach of the synovial fluid and arthrocentesis should remain the gold standard to rule out septic arthritis and bring out the exact nature of the crystal.28
In conclusion, US is a promising tool for the diagnosis and management of CPPD to improve outcomes for patients; however, further work is required, particularly in defining the pathology and establishing the validity and reliability of the US-detected signs.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online figures
Footnotes
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.