Article Text

Abstract
Giant cell arteritis (GCA) is a chronic systemic vasculitis affecting large-sized and medium-sized vessels. Glucocorticoids are currently the mainstay of treatment for GCA and associated large vessel vasculitis (LVV) but are associated with frequent adverse events. Methotrexate has only demonstrated a modest benefit while anti-TNF biological agents (infliximab and etanercept) have been inefficacious. Elevated levels of interleukin-6 (IL-6), a proinflammatory cytokine, has been associated with GCA. Tocilizumab (TCZ), a humanised antihuman IL-6 receptor antibody, has been used successfully in several reports as a treatment for GCA and LVV. We report the potentially long-term successful use of TCZ in 8 cases of refractory LVV. All of our patients achieved a good clinical response to TCZ and C reactive protein reduced from an average of 70.3 to 2.5. In all cases, the glucocorticoid dose was reduced, from an average of 24.6 mg prednisolone prior to TCZ treatment to 4.7 mg, indicating that TCZ may enable a reduction in glucocorticoid-associated adverse events. However, regular TCZ administration was needed for disease control in most cases. TCZ was discontinued in one case due to the development of an empyema indicating the need for careful monitoring of infection when using this treatment.
- DMARDs (biologic)
- Giant Cell Arteritis
- Systemic vasculitis
- Treatment
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known on the subject?
Giant cell arteritis (GCA) usually responds to glucocorticoids. However, refractory patients may require treatment with disease modifying and biologic agents such as Tocilizumab.
What might this study add?
This study demonstrates the long term safety and efficacy of Tocilizumab in selected patients with GCA and large vessel vasculitis (LVV).
How might this impact on clinical practice?
Patients with refractory GCA or LVV should be considered for Tocilizumab therapy.
Introduction
Giant cell arteritis (GCA) is a systemic vasculitis affecting large and medium sized vessels.1 While it is often limited to the temporal arteries and cranial branches, widespread involvement of vessels including the aorta and major vessels is a significant cause of morbidity and mortality. Glucocorticoids (GC) are the mainstay of treatment, but adverse events are frequent (86% at 10 years) due to the protracted treatment course, and flares are common (up to 50%), especially within the first year requiring high dose continuing GC.2 Methotrexate affords only modest benefit and biological agents such as infliximab and etanercept have been shown to be inefficacious.3–5 There is clearly a need for effective and safer steroid-sparing therapies in GCA.
Interleukin-6 (IL-6), a proinflammatory cytokine, is used as a target of disease therapy in several inflammatory conditions. Originally reported by Dasgupta and Panayi6 in 1990, IL-6 levels are elevated in GCA and reports have shown that levels correlate with disease activity.7 Dysregulated production of IL-6 results in exaggerated acute-phase protein production and recruitment of chemokines and leukocytes, driving the pathological process and associated constitutional symptoms.8 Tocilizumab (TCZ) is a humanised antihuman IL-6 receptor antibody that competitively inhibits binding of IL-6 to both the membrane-bound and soluble IL-6 receptors.9 In view of the high relapse rates, GC-related adverse events and inadequate disease control, TCZ has been used in several reports with good clinical and biochemical response.10–16 Furthermore, several of these reports achieved a significant reduction or complete withdrawal of GC.10 ,11 ,14 ,15 ,16 However, significant adverse events occurred in two reports including neutropaenia, pneumonia, cytomegalovirus infection and transaminitis.11 ,14
The cases we describe provide further evidence of the potential benefit and safety of long-term TCZ therapy for refractory GCA. Clinical response was evaluated using the ITAS 2010 (a validated disease assessment tool for large vessel vasculitis (LVV)) and by imaging in one case.
Methods
This is an open case series in which eight patients with GCA were treated with TCZ 8 mg/kg/month. The average patient follow-up was 2 years and 10 months (range 1–4 years 4 months). The total TCZ dose, disease duration at initiation of treatment, pre-TCZ and post-TCZ C reactive protein (CRP) levels, pre-TCZ and post-TCZ prednisolone dose, follow-up duration, ITAS scores and adverse reactions are listed in table 1. All ITAS scores reduced to zero following TCZ treatment.
Number of TCZ doses, disease duration at initiation of treatment, pre-TCZ and post-TCZ CRP levels, pre and post-TCZ prednisolone dose, duration of follow-up, pre and post-TCZ ITAS scores and adverse events for each case study
Case 1
A 68-year-old woman presented in 2010 with shoulder and pelvic girdle pain, night sweats, fatigue, weight loss and arm claudication. Examination revealed absent radial pulses bilaterally and a left femoral artery bruit. Blood pressure was 147/84 in the right and 132/82 in the left arm.
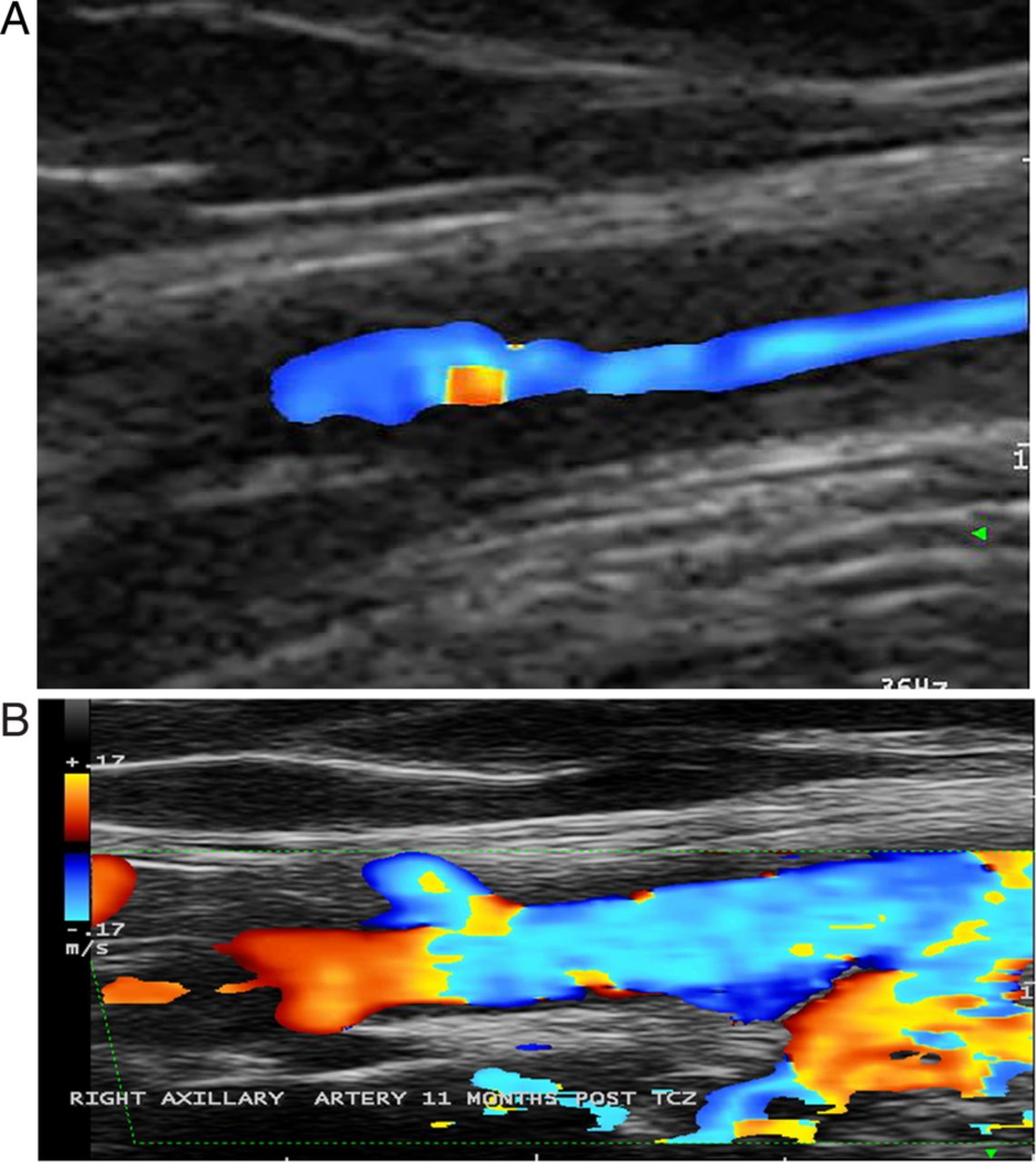
Positron emission tomography-computerised tomography (PET-CT) scan showed evidence of LVV in the abdominal aorta, subclavian, iliac and axillary arteries (figure 1A). Right axillary artery ultrasound revealed evidence of stenosis and minimal flow (figure 2A).

Positron emission tomography-computerised tomography pretocilizumab (TCZ) (A) and post six cycles TCZ (B).

{kind=link}
{kind=link}
Ultrasound right axillary artery pretocilizumab (TCZ) (A) and post 11 cycles TCZ (B).
She received intravenous and oral GC (40 mg prednisolone) with good response and CRP reduced from 78 to 27. However, she was unable to taper the GC dose and was started on TCZ with clinical improvement, return of radial pulses and increase in blood pressure, necessitating antihypertensive therapy to be restarted. CRP improved to 3. She remains clinically stable on 3 mg prednisolone after 30 TCZ infusions. A repeat PET-CT scan showed no evidence of active LVV (figure 1B). Repeat right axillary artery ultrasound demonstrated excellent flow (figure 2B).
Case 2
A 63-year-old woman presented in 2011 with weight loss, postprandial abdominal pain, bitemporal headache and blurring of vision. Temporal artery biopsy confirmed GCA. PET-CT scan revealed LVV in the right axillary artery and thoracic aorta. GC treatment was started (prednisolone 60 mg) with improvement of CRP from 155 to 13 but proximal muscle weakness and an acneiform rash led to lowering the GC dose to 15 mg, with subsequent return of headaches. TCZ was started in 2012 with symptom resolution and reduced CRP (1), allowing GC reduction to 3 mg. She has had intermittent courses of TCZ over 30 months with good disease control.
Case 3
A 72-year-old man was admitted in 2012 with fatigue, abdominal pain, poor mobility and weight loss. CRP was 200, haemoglobin 7.5 g and CT abdomen and pelvis revealed evidence of aortitis. PET-CT scan confirmed LVV involving the aorta and extracranial vessels.
He was treated with prednisolone 40 mg and started TCZ at diagnosis with a marked clinical improvement. Prednisolone was reduced to 20 mg, with improved haemoglobin (12 g), CRP (5) and mobility.
Case 4
This previously reported 67-year-old woman with refractory PMR since 2003, presented in 2010 with worsening proximal pain and stiffness, temporal headache, weight loss and fatigue.17 PET-CT scan revealed LVV in the aorta, axillary and subclavian arteries. Initial prednisolone dose was 60 mg with improvement of CRP from 78 to 28. Prednisolone was reduced to 15 mg with persistent symptoms and TCZ was started with reduction of CRP (1). The TCZ dose was reduced to 4 mg/kg/month and she was successfully weaned off of GC and inflammatory markers have remained normal. She has experienced three episodes of transient neutropaenia.
Case 5
This 75-year-old man presented in 2011 with typical features of PMR and was started on monthly intramuscular depomederone injections. He subsequently developed night sweats, weight loss and muscle weakness. PET-CT scan revealed LVV in the aorta, extracranial and axillary arteries, and he was started on prednisolone 40 mg with leflunomide. CRP improved from 83 to 13 but he subsequently developed arm claudication in 2012 and was started on TCZ with good disease control and reduced CRP (1). Unfortunately he developed an empyema, necessitating the cessation of leflunomide and TCZ. Leflunomide was restarted in 2014 and he remains clinically stable on prednisolone 4 mg.
Case 6
This 80-year-old woman presented in 2011 with temporal artery biopsy-positive GCA and was started on prednisolone 40 mg. CRP improved from 329 to 226. In 2012, she developed abdominal pain and loose stools and PET-CT scan, revealed LVV in the aorta, axillary and carotid arteries. Leflunomide and TCZ were introduced resulting in good disease control, and reduced CRP (7). The GC dose was tapered from 15 to 5 mg, and TCZ was reduced in 2013 to 6 mg/kg/month. The course was complicated by splenic infarction. A repeat PET-CT scan demonstrated improvement in the aorta but ongoing LVV. Leflunomide was discontinued in 2013 secondary to hypertension and diarrhoea, and methotrexate was started. TCZ was temporarily stopped due to abdominal pain but was recommenced due to a recurrence of GCA symptoms, with good symptom control.
Case 7
This 66-year-old man was diagnosed with temporal artery biopsy and ultrasound-positive GCA in 2010. The patient was started on prednisolone 40 mg and CRP reduced from 52 to 50. He was unable to reduce the dose below 20 mg and leflunomide was added. He subsequently developed GC-related diabetes and myopathy with headaches and abdominal pain. A PET-CT scan in 2012 confirmed LVV in the thoracic aorta, axillary, subclavian and carotid arteries.
He was started on TCZ in 2012 with good response and reduced CRP (1). GC were successfully weaned with improved diabetic control. A recurrence of symptoms led to reintroduction of TCZ and methotrexate was added in 2013. His symptoms remain stable on TCZ, leflunomide and methotrexate.
Case 8
This 69-year-old man presented with a 5-year history of GCA manifested by headaches, stiffness and constitutional symptoms. Over the 5 years, he was treated with prednisolone doses varying between 10 and 30 mg. CRP improved from 45 to 5.4, but there was only a partial clinical response. PET-CT scan in 2013 revealed LVV in the aorta, carotid and subclavian arteries. The patient was started on TCZ in 2014, followed by subcutaneous TCZ every 2 weeks and GC dose was reduced from 12 to 2.5 mg with good clinical response and improved CRP (1). TCZ was stopped after 6 months and the patient remains clinically stable with normal inflammatory markers.
Discussion
We report the successful long-term use of TCZ in eight cases of refractory LVV. All patients had a good clinical and biochemical response to therapy. TCZ was well tolerated over a long follow-up and GC dose reduction was possible in all cases. In case 1, there was evidence of recanalisation with TCZ therapy. However, as noted in previous reports, we reported one significant adverse event (empyema) indicating the need for careful monitoring of infection in patients on this treatment.
LVV is now increasingly recognised in a subgroup of patients with GCA and/or PMR refractory to conventional GC therapy. These are also patients who suffer adverse effects from long-term high-dose GC as our cases demonstrate. Cardiovascular complications and increased early mortality rates are now recognised in GCA, perhaps related to uncontrolled disease and to the proatherogenic effects of prolonged GC therapy. TCZ in these patients, as in our case series, may enable a reduction and in some cases a cessation of GC.
In conclusion, our case series provides further evidence of the potential efficacy and safety of long-term TCZ in a particular subgroup of patients with GCA and PMR with LVV. This requires further evaluation in a multicentre setting.
References
Footnotes
Contributors The article was written by JE with significant contributions from the other authors (LS, FB and BD). Patient recruitment was coordinated by BD and FB.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.