Article Text

Statistics from Altmetric.com
Interleukin 17 (IL-17) plays an important role in many chronic inflammatory diseases such as psoriasis, psoriatic arthritis, ankylosing spondylitis and rheumatoid arthritis (RA).1 Measuring circulating IL-17 levels could be crucial to identifying patients who would benefit from IL-17-targeted therapies.2 Detection by ELISA has been difficult with high variability between studies. Furthermore, IL-17 function is critical to taking into consideration the contribution of activators (eg, tumour necrosis factor (TNF)-α acting in synergy with IL-17) and inhibitors (IL-25, autoantibodies).
In previous studies, human umbilical vein endothelial cells (HUVEC) were shown to be highly sensitive to IL-17 stimulation for the production of the chemokine IL-8.3 These cells were thus used in a functional bioassay to measure circulating bioactive IL-17. To determine the contribution of IL-17 in the IL-8-inducing activity, plasma samples at the dilution of 10% were first preincubated with or without an anti-IL-17 antibody at 10 µg/mL (R&D systems, Paris, France), before being added to HUVEC (see more details in figure 1 legend and in figure 1A, B). After 48 h of incubation, IL-8 production was measured in supernatants by ELISA. Plasma samples from 52 patients with RA and 30 healthy donors paired for sex and age were tested (table 1). Patients with RA were selected from a large database linked to a biobank and paired for key parameters, including anticyclic citrullinated protein antibodies, except for the level of destruction. There were 17 patients without destruction (Larsen score from 0 to 1) and 35 patients with destruction (Larsen score over 2).
Clinical characteristics of patients with rheumatoid arthritis (RA) compared with healthy donors

{kind=link}
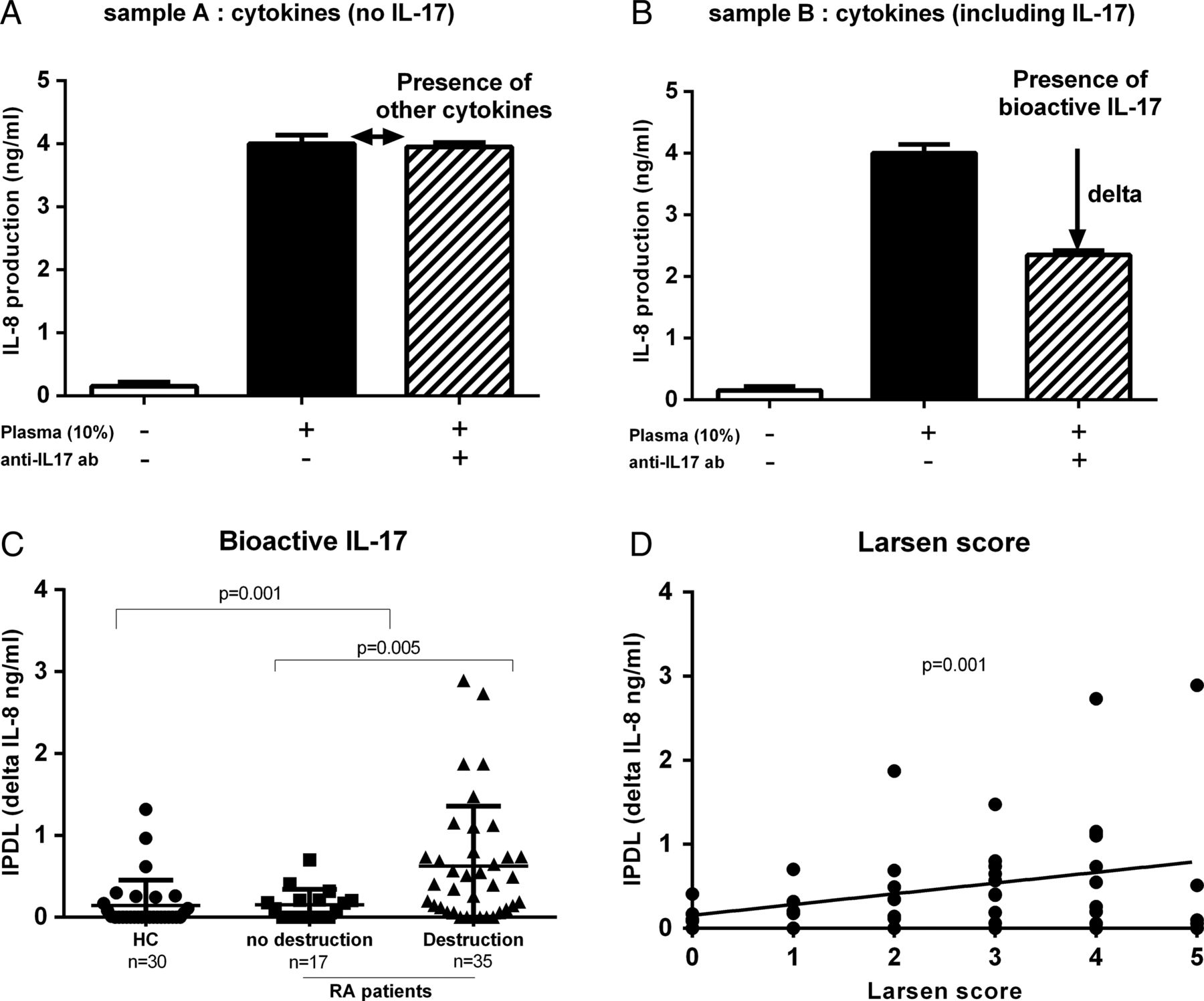
Detection of IL-17 pro-inflammatory dependent level (IPDL) in patients with rheumatoid arthritis (RA) compared with healthy donors. This bioassay is based on the ability of human umbilical vein endothelial cells (HUVEC) to produce IL-8 in the presence of IL-17. The specific contribution of IL-17 in plasma was determined by the addition of an anti-IL-17 blocking antibody. HUVEC at the density of 10 000 cells/well were cultured in 96-well plates in 200 µL of EGM2 medium. Plasma samples at 10% were first preincubated with or without anti-IL-17 antibody at 10 µg/mL for 1 h before addition to the cells. After 48 h of culture, supernatants were collected and production of IL-8 was measured by ELISA. IPDL or delta IL-8 production (ng/mL) represents the production of IL-8 with and without addition of anti-IL-17. (A) In sample A, no reduction of IL-8 production was observed with the addition of anti-IL-17 antibody, indicating the presence of IL-8-inducing factors other than IL-17. (B) In sample B, a reduction was observed, indicating the contribution of IL-17 in the IL-8-inducing activity. (C) Detection of bioactive IL-17 in RA plasma with (n=35) or without bone destuction (n=17) and health controls (HC) plasma (n=30). (D) Correlation analysis between IPDL and Larsen score in patients with RA.
IL-17 pro-inflammatory dependent level (IPDL) corresponding to bioactive IL-17 represents the difference between the production of IL-8 with and without addition of anti-IL-17 antibody. Levels were significantly higher in patients with RA versus healthy donors (0.16±0.33 ng/mL vs 0.47±0.65 ng/mL, p=0.001, figure 1C) and in destructive versus non-destructive RA (0.62±0.73 ng/mL vs 0.15±0.18 ng/mL, p=0.005), with a positive correlation between IPDL and Larsen score (p=0.001) (figure 1D). However, no significant correlation was observed between disease duration (p=0.1) and activity (Disease Activity Score in 28 Joints) (p=0.6) (data not shown).
IL-17 now represents an important target for treatment of chronic inflammation with promising results.4 Our results demonstrated that bioactive IL-17 can be measured in plasma using a simple assay. Levels are higher in patients with RA compared with controls and associated with RA severity, in line with results at the local site.2 However, 25% of patients with RA were negative for circulating IL-17. In previous clinical trials, 30% to 40% of the patients did not respond to IL-17 inhibition.5–7 It remains to be demonstrated if this correlates with an absence of circulating IL-17. Conflicting results were obtained on IL-17 detection by ELISA; most studies reported very low/undetectable serum/plasma levels.8 More importantly, ELISA measures protein content but does not evaluate function. This is critical since IL-17 is well known for its synergistic interactions with other cytokines, such as TNF-α, a key argument for treatment with dual inhibition of TNF and IL-17. As IL-17 contributes to the chronicity of inflammation, targeting it at an early stage may prevent irreversible features of chronic inflammation from occurring.7 Better detection of potential responders would be critical at that stage.
This bioassay can detect circulating bioactive IL-17 and could be used as a selection biomarker for patients more susceptible to respond to an anti-IL-17 treatment, in conditions such as RA with a high degree of variability of the response.5 ,6 These encouraging results need to be extended to larger populations of RA and other IL-17-driven diseases, specifically using samples for which the response to an IL-17 inhibitor is known. The next step could be selecting patients on pretreatment levels to confirm the predictive value of the test.
Footnotes
Contributors NN-T: experiments and writing; PM: concept and writing.
Funding NN-T is supported by the IHU prometteur OPERA. PM is a senior member of and supported by the Institut Universitaire de France.
Competing interests NN-T and PM hold a patent on the determination of bioactive IL-17.
Patient consent Obtained.
Ethics approval Ethics committee of the hospitals of Lyon.
Provenance and peer review Not commissioned; externally peer reviewed.