

To the Editor:
It is increasingly understood that the association between obesity and osteoarthritis (OA) is partially mediated by a systemic, inflammatory effect of adipokines such as leptin (LEP), adiponectin (ADIPO), and resistin. The association of obesity and OA of non-weight-bearing joints, such as the hand, lends further support to this hypothesis1,2. LEP and resistin have been suggested to have a strong proinflammatory influence3,4, while the role of ADIPO in a knee joint is unclear, as some have shown an antiinflammatory effect5 and others suggest a proinflammatory effect6. Similarly, the ADIPO receptors have been identified in the knee joint only6.
No study has examined the epidemiologic relationship between obesity and shoulder OA or identified these obesity hormones in the shoulder joint. The objective of our study was to determine if the adipokines LEP, ADIPO, and resistin are present in the shoulder synovial fluid (SF) of patients with OA and to examine the relationships of these hormones to measures of body habitus.
We recruited patients awaiting elective arthroscopic rotator cuff repair or shoulder replacement surgery to participate, between 2009 and 2011. We excluded patients with a history of previous shoulder surgery, previous steroid injection, posttraumatic arthritis, or a history of inflammatory arthropathy. Patients undergoing shoulder replacement surgery for a diagnosis of OA were used as the source for articular chondrocytes. The study protocol was approved by the Human Subject Review Committee.
Demographic data, including body mass index (BMI) and waist circumference (WC), were collected. Our study cohort had at least 1 chondral surface with Grade 3 or Grade 4 damage as determined by the Outerbridge classification7.
SF and venous blood samples were collected and stored at −80°C; protease inhibitors were added, at the time of shoulder surgery, under sterile conditions. Milliplex™ MAP kits (Millipore, Natick, MA, USA) were used to detect levels in triplicate of relevant adipokines and inflammatory cytokines. All samples were read on the BioPlex 200 reader.
Performance characteristics for the immunoassays were determined with the intraassay coefficient of variation for each analyte.
Chondrocyte isolation
Cartilage was immediately placed into transport media and kept at 4°C until processed. Briefly, cartilage was washed in phosphate buffered saline and transferred to a culture dish containing DMEM supplemented with 10% fetal bovine serum (FBS) and hyaluronidase. Samples were incubated at 37°C overnight and the next day were filtered, centrifuged, resuspended, counted, and plated.
Cell culture
Human liver HepG2 cells, human embryonic kidney HEK293 cells, mouse fibroblast C3H10T1/2, and mouse prechondrocytic ATDC5 cells were grown in DMEM supplemented with 10% FBS. ATDC5 and C3H10T1/2 cells were induced to differentiate into chondrocytic cells by the addition of insulin and BMP2, respectively. Samples were passaged through a needle and then centrifuged. Supernatants were collected and protein concentration determined.
Western blot analysis
Samples were run on SDS-polyacrylamide gels and blots were probed with antibodies directed against AdipoR1, AdipoR2, and ObRb.
Immunofluorescence microscopy
Chondrocytes were grown in 12-well Falcon dishes on 18-mm glass coverslips coated with 25 μg/ml poly-L-lysine. Cells were fixed and permeabilized and then incubated in 1% bovine serum albumin, then left overnight at 4°C with AdipoR1, AdipoR2, ObRb, collagen 11, sarcomeric actin, or collagen 1 primary antibodies. All fluorescence images were acquired using a Leica DMI 6000B fluorescence microscope.
Continuous data were compared between groups with the Kruskal-Wallis test, while correlations were determined using nonparametric Spearman coefficients.
Separate linear regression models were built to evaluate the relationship between body habitus (BMI and WC) and the 3 dependent variables: levels of SF LEP, SF ADIPO, and SF resistin. The models were then adjusted for age and sex.
A sample size of 35 patients was chosen for this study, anticipating 4 independent variables in the regression model, thus allowing for > 8 outcomes per covariate. All statistical analysis was performed with SPSS Version 13.0 (SPSS, Chicago, IL, USA).
In our sample of 35 patients, there were 15 men (43%), with mean age of 63.0 years (SD 10.1) and mean BMI of 28.3 kg/m2 (SD 5.4).
Statistically significant correlations were found between SF and serum adipokine levels, that is, LEP 0.39 (p = 0.02); ADIPO 0.47 (p = 0.01); and resistin 0.69 (p < 0.001). Regression modeling showed that female sex and a greater BMI were predictors of higher level of SF LEP, while only a greater BMI predicted a lower level of SF ADIPO, independent of age and WC (p < 0.05). For the model predicting SF resistin levels, no variables reached statistical significance.
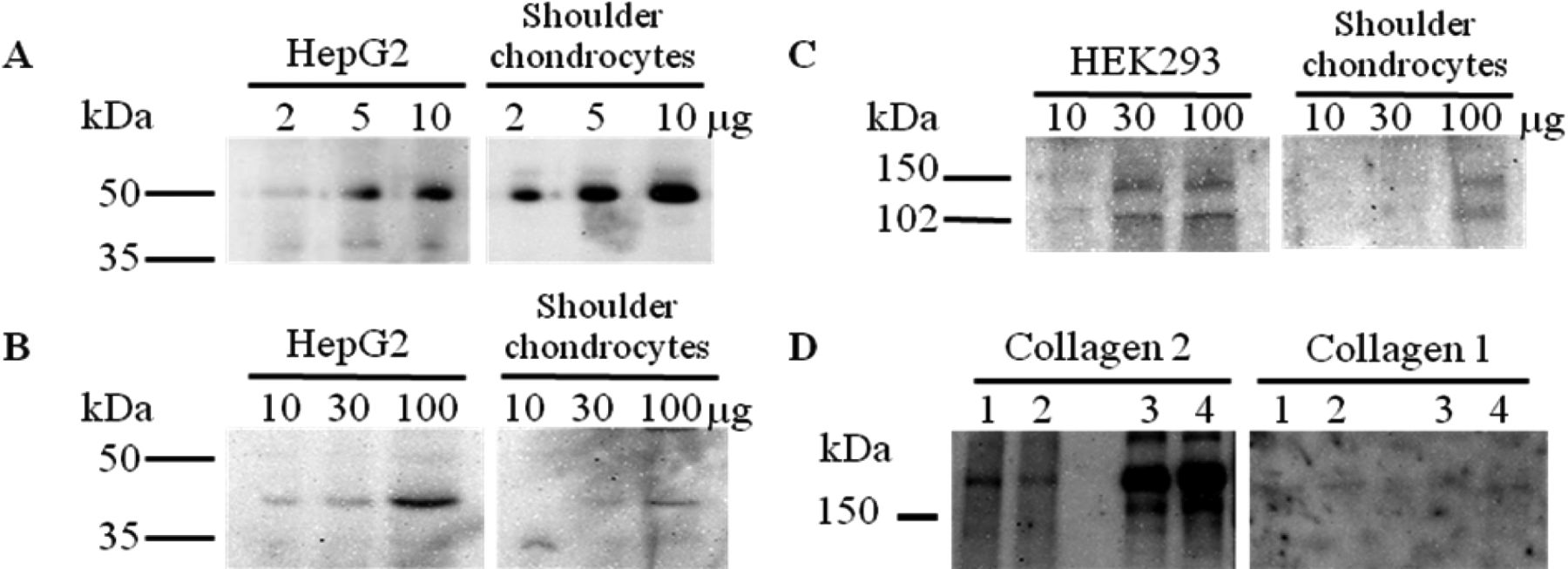
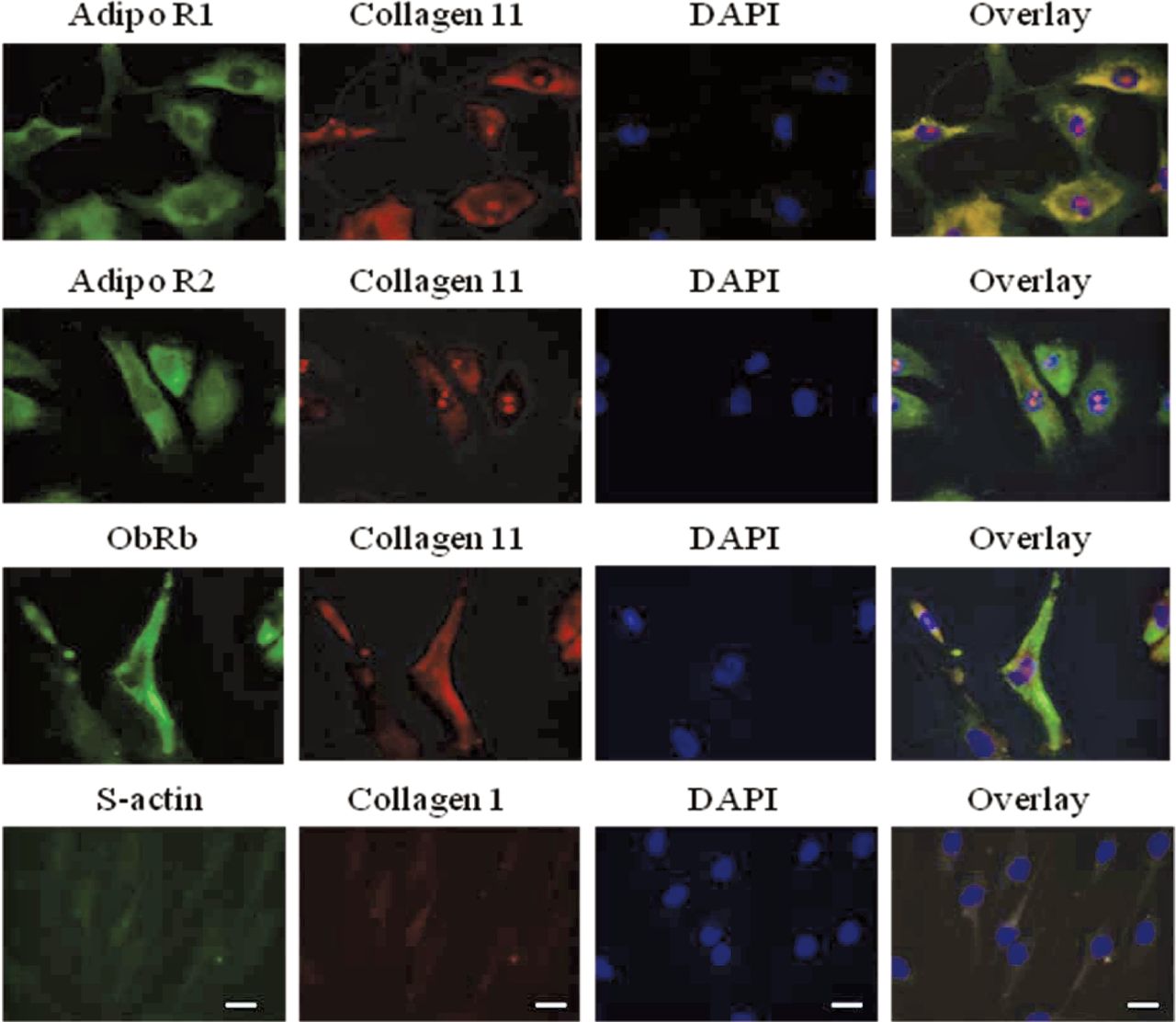
The most prevalent receptor detected was the AdipoR1 receptor, which demonstrated a detectable band when as little as 2 μg of lysate was run on the gel (Figure 1). Both the AdipoR2 and leptin receptor (ObRb) demonstrated lower levels of expression and were detectable only when 100 μg of cell extract was loaded. Immunofluorescence imaging on a confocal microscope revealed a similar pattern of diffuse expression throughout the chondrocytes (Figure 2). Intensity of staining was also found to be comparable across all 3 forms of receptors.

Expression of adiponectin and leptin receptors in shoulder cartilage. Total cell lysates extracted from shoulder cartilage chondrocytes, human hepatic (HepG2) and embryonic kidney (HEK293) cell lines were run on denaturing gels and quantified by Western blotting. Different quantities of cell lysates were loaded: (A) 2 μg, (B) 5 μg, and (C) 10 μg for the adiponectin type 1 receptor; and (D1) 10 μg, (D2) 30 μg, and (D3) 100 μg for the adiponectin type 2 and leptin receptors.

Expression of adiponectin and leptin receptors in shoulder chondrocytes. Cells were counterstained with collagen 11 and the nuclear stain DAPI. Scale bars represent 20 μm.
We found that the shoulder joint contained adipokines at levels that correlated with BMI. Further, we identified the LEP ObRb and ADIPO1 and ADIPO2 receptors on the surface of chondrocytes of late-stage OA shoulders. These findings strengthen the hypothesis of the metabolic pathways of obesity and OA.
Our work is the first to identify that fat-derived hormones are present in OA shoulder joints, whereas other research examining adipokines and OA of non-weight-bearing joints is limited. One group has shown that greater serum ADIPO may be associated with a decreased risk of progression of radiographic hand OA8, while another showed that greater serum ADIPO is associated with more advanced hand OA9. One final cross-sectional study found that elevated serum resistin was associated with an increased severity of prevalent hand OA, whereas serum ADIPO had no relationship10.
A limitation of our study is the cross-sectional design, and thus we cannot assume that adipokines observed within the shoulder joint contributed to the OA in our patients.
We successfully identified fat-derived hormones and the corresponding receptors within OA shoulder joints.








{kind=link}
{kind=link}