Article Text

Abstract
Osteoarthritis (OA) of the knee is the most common arthritic disease, yet a convincing drug treatment is not available. The current narrative review focuses on integration of scientific evidence and professional experience to illustrate which management approaches can be taken for prototypical individual patient profiles with early knee OA. Animal models suggest that: (1) OA can progress even in the presence of fully recovered movement kinetics, kinematics and muscle activation patterns; (2) muscle weakness is an independent risk factor for the onset and possibly the rate of progression of knee OA; (3) onset and progression of OA are not related to body weight but appear to depend on the percentage of body fat. From studies in the human model, one could postulate that risk factors associated with progression of knee OA include genetic traits, preceding traumatic events, obesity, intensity of pain at baseline, static and dynamic joint malalignment and reduced muscle strength. Taken this into account, an individual can be identified as early knee OA at high risk for disease progression. A holistic patient-tailored management including education, supportive medication, weight loss, exercise therapy (aerobic, strengthening and neuromuscular) and behavioural approaches to improve self-management of early knee OA is discussed in individual prototypic patients. Secondary prevention of early knee OA provides a window of opportunity to slow down or even reverse the disease process. Yet, as the sheer number of patients early in the OA disease process is probably large, a more structured approach is needed to provide appropriate care depending on the patient’s individual risk profile.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0
Statistics from Altmetric.com
Introduction
Osteoarthritis (OA) of the knee is the most common arthritic disease, yet there is no convincing drug treatment available today that affects the progression of the disease process. There are many reasons for this, including the lack of understanding of what drives the disease process and the heterogeneity of the patient population.1 Indeed, there is considerable variability in disease trajectories, also dependent on patient profiles and the defined outcomes, leading to a need for disease stratification. A recent report has proposed a framework for the investigation of clinical and structural phenotypes; the patient characteristics and disease stage should be considered as most relevant for stratification of patients to be used in future studies.2 This approach will be of value for the field, but from a pragmatic clinical standpoint, it neither helps the individual patient nor the clinician facing the patient, today. However, we believe there is reasonable scientific evidence from studies in both animals and the human model that a personalised, patient-centred approach can result in successful clinical outcomes.
Therefore, in this narrative, we try to integrate scientific evidence and our professional experience to illustrate which approaches can be taken for prototypical individual patient profiles that are most likely going to successfully alleviate pain, control symptoms and signs, maintain or restore function and perhaps even affect the disease course. For sure, it is not our goal to be fully comprehensive, and we made some choices. This paper focuses on secondary prevention, thus on early knee OA, as we believe this being a window of opportunity for interventions that benefit the patient.3 As OA develops slowly, in most cases, pain, symptoms/signs and loss of function precede radiographic changes, although the opposite is also possible in some cases. Consequently, there is in general poor disease management in clinical practice over the course of the disease. Indeed, typical examinations in primary care do not reveal abnormalities in blood exam and imaging, certainly not in early disease, and the patient is getting the message to adapt and cope with it. Healthcare providers are not taking any coordinated action and await late stage disease associated with pronounced clinical manifestations including severe functional limitations and radiographic advanced disease. Then, more attention is geared towards surgical interventions mostly total knee replacement (with some exceptions). However, OA is a chronic disease process and begs for early disease intervention, as has been illustrated in other chronic arthritic diseases such as rheumatoid arthritis.4
Patient profiles with early knee OA, risk factors for progression, and what we have learnt from the investigations in both the animal models and the human model are introduced. The core and uniqueness for this narrative is our discussion on secondary prevention strategies for some prototypical patient profiles. We also focus our attention on the patient’s perspective in this approach, what is acceptable for the patient and how can we motivate the patient to adhere to a treatment regimen. In the conclusions and future directions, we will reflect on how to incorporate these strategies into daily clinical practice.
Patient profile of early knee OA
In view of the above-mentioned discussion, there is a clear need to more accurately define early knee OA and come to general classification criteria and outcomes, widely accepted by the clinicians and all parties involved. We have started to tackle this challenge by organising a workshop in Tokyo, Japan, in November 2014, the outcome of which resulted in a manuscript5 proposing steps towards the development of classification criteria for early OA of the knee. These classification criteria aim to identify in a standardised approach a group of patients with the highest chance to develop frank knee OA as defined by the 1986 ACR criteria.6 This is just the beginning of the process of producing consensus classification criteria, and validation and further iterations of these criteria will be required. MRI-related imaging and biochemical biomarkers may enter the classification criteria of early OA as they prove their utility and become more readily accessible.
Since there are not yet validated classification criteria for early knee OA, we attempted to bring together aspects of the disease process in its early phase that appear to be common across reported findings resulting in a profile of early knee OA patients. We made a distinction between structural and clinical findings, as the correlation between those is limited.
As for structural findings associated with symptomatic early knee OA, most of the data are obviously detected by MRI as early OA is per definition preradiographic, that is, no or very discrete changes on regular X-rays. Most MRI findings reported a significant larger amount and cumulative score for size of bone marrow lesions, the amount and cumulative score for size and percentage of full thickness cartilage loss in the tibiofemoral (TF) region, meniscal lesions and cumulative size and presence of synovitis and/or effusion in the early knee OA group compared with their healthy peers.7 8 It is precisely with these findings in mind that a group of investigators proposed classification criteria for early OA partially defined by MRI findings,7 although also these criteria are awaiting validation in independent cohorts. Nevertheless, in the primary care setting, our attention should go into clinical characteristics associated with early disease.5
In the early phases of the disease, pain is related to activity and becomes more constant over time.9 Baert et al 8 reported more knee pain and symptoms in women with early medial knee OA compared with the healthy controls and comparable with women with established medial knee OA. Reduced self-reported measure of physical function and quality of life are also reported to be already present in this stage of the disease.10 This was not the case for the performance-based functional measures.8 11
Quadriceps weakness had also been reported in patients with early knee OA,8 12 which is in line with evidence on quadriceps weakness preceding the onset of knee OA.13 14 Despite the evidence on proprioceptive deficits in moderate to severe patients with knee OA, a study on patients with early knee OA showed that proprioceptive accuracy was comparable with healthy controls.12 On the other hand, Mahmoudian et al 15 reported altered proprioceptive weighting, and a stronger ankle-steered proprioceptive postural strategy, during standing.
Static and dynamic knee alignment were measured in a group of subjects with early knee OA and were compared with a group of subjects with established OA, as well as a control group.10 The presence and magnitude of varus thrust was greater in women with early medial knee OA than in healthy controls, similar to the findings in women with established medial knee OA.10 In contrast, there was no significant difference between the early OA and healthy age-matched controls, regarding the static varus alignment.
Studies on biomechanical characteristics of subjects with early knee OA are limited, and due to the non-consistent classification of knee OA in these studies, results are barely comparable. Investigations on gait characteristics in women with early medial knee OA demonstrated no altered gait pattern or increase in knee joint loading during walking in patients with early medial knee OA, compared with the healthy controls.8 11
Lastly, based on the literature, it seems relevant to also consider patellofemoral (PF) complaints at the early stages of knee OA. According to a recent study by Hinman et al 16 70% of people (ages>40 years) with PF pain demonstrated radiographic OA. Importantly, in the same cohort, they reported that osteoarthritic changes might occur first in the PF joint, preceding structural damage in the TF joint.16
Risk factors associated with chronicity/progression of disease
In this section, we will look into the research on risk factors associated with progression of knee OA: first, in (non-human) animal models, and second, in the human model:
The (non-human) animal models
What can we learn from (non-human) animal models about OA prevention and progression?
Background
One of the difficulties with the prevention, treatment and our understanding of OA is that it creeps along slowly and without major symptoms over years and decades. Therefore, defining a time point for the onset or the rate of progression of OA is virtually impossible in human patients. Animal models, on the other hand, can be used for controlled interventions that are known to cause OA, thereby fixing the time point of OA onset. In most animal models used today, OA develops at a much greater rate than in humans, with changes in articular cartilage properties, composition and structure visible within days or a few weeks following intervention (eg, refs 17 18). This fast rate of OA progression, and the possibility for invasive measurements in animal models, allows for detailed and systematic evaluation of the development of OA that is not possible in human patients.
However, every animal model, including humans, shows different symptoms to an apparently similar intervention. For example, loss of the anterior cruciate ligament (ACL) in the knee causes permanent gait changes and changes to the subchondral bone in dogs but not in cats.19–22 Similarly, a given perturbation, like the loss of the ACL, can cause distinctly different responses and joint degeneration in the same animal species.23 24 Here, we will discuss lessons learnt from three distinct animal models of OA (post-traumatic, muscle weakness/imbalance, and obesity) that would have been hard to reach from human studies and evaluate the possible implications for human OA, its prevention and treatment.
Post-traumatic (ACL transection and partial meniscectomy) model of OA
We have used ACL transection in a variety of animal models of OA, but some of the most surprising results came from studies in the ACL-deficient cat. It has been observed in many studies that ACL loss is associated with gait and movement asymmetries in humans and animals and changes in knee joint loading (eg, refs 23–25; figure 1). The altered joint loading has been interpreted as the major factor for the onset and progression of OA. Therefore, knee OA was assumed to be stopped if knee joint loading and kinematics could be brought back to normal levels following ACL loss. In the ACL-deficient cat, in contrast to other models of ACL loss, including dogs, sheep and humans, normal movement kinematics and kinetics and normal muscle activation patterns are re-established within 4–6 months following ACL transection.21 Therefore, one would assume OA progression is stopped too. However, that is not the case, as cats develop bona fide OA in the knee following ACL transection despite normal knee joint kinematics.

(A) Vertical ground reaction force vs. time histories for the intactand ACL transected hind-limb in the cat. Note the initial unloading of the experimental limb (open symbols) and overloading of the contra lateral intact limb (filled symbols). Results are shown for 7 animals with 10 step cycles peranimal. After about 6 months, the vertical ground reaction forces are similar between the experimental and the intact contra lateral hind limb. (B) Quadriceps forces (measured using an implantable force transducer in the patellar tendon) and vastus lateralis EMG prior to ACL transection (left panel) and four weeks following ACL transection (right panel) in a representative animal. Note the decrease in muscle force to about 1/3 of the initial level following ACL transection, and the disrupted EMG during the stance phase of walking for the vastus lateralis after ACL transection, compared to the solid and continuous EMG prior to the intervention. Pre-intervention activation and forces are reached at 4–6 months post ACL transection (not shown).
Also, normal knee joint kinematics and kinetics and re-establishment of normal muscle activation patterns and forces are typically associated with normal knee joint loading. However, we found that the knee joint cartilage in ACL-transected cats changes substantially within 4 months of intervention: the cartilage becomes softer and thicker, thereby changing the load transfer from bone to bone within the knee. Specifically, PF joint contact areas were increased by 22% and peak pressures reduced by 50% 4 months post-ACL transection25 26 for identical knee joint loading conditions.
Lessons learnt: OA progresses even in the presence of fully recovered movement kinetics, kinematics, and unchanged muscle activation. Furthermore, identical knee joint kinematics and external loading does not ensure normal joint loading as the properties of articular cartilage change quickly following trauma and produce load transfer patterns different from those in the healthy joint.
Muscle weakness model of OA
Muscle weakness, particularly knee extensor weakness, has been associated with knee joint OA.27–32 However, it remains controversial if muscle weakness is caused by knee OA or if knee extensor weakness is an independent risk factor for the development and rapid progression of knee OA. In contrast to the human model, muscle weakness in animal models can be produced consistently, repeatedly and with a precisely defined start in a variety of ways, including nerve transection,33 hind limb suspension,34 disuse atrophy,35 36 and chemical denervation.37–39 We used botulinum toxin type A to induce controlled and reversible weakness in the quadriceps muscles of rabbits. Rabbits showed increased Mankin scores, associated with significantly increased knee OA in experimental joints at 1, 2 and 3 months postweakness induction30 40 41 (figure 2). Quadriceps muscle imbalance, introduced by denervation of the vastus medialis or vastus lateralis muscles, did not change the pressure distributions in the PF joints of rabbits42 but still resulted in PF OA at 3 months post intervention.43
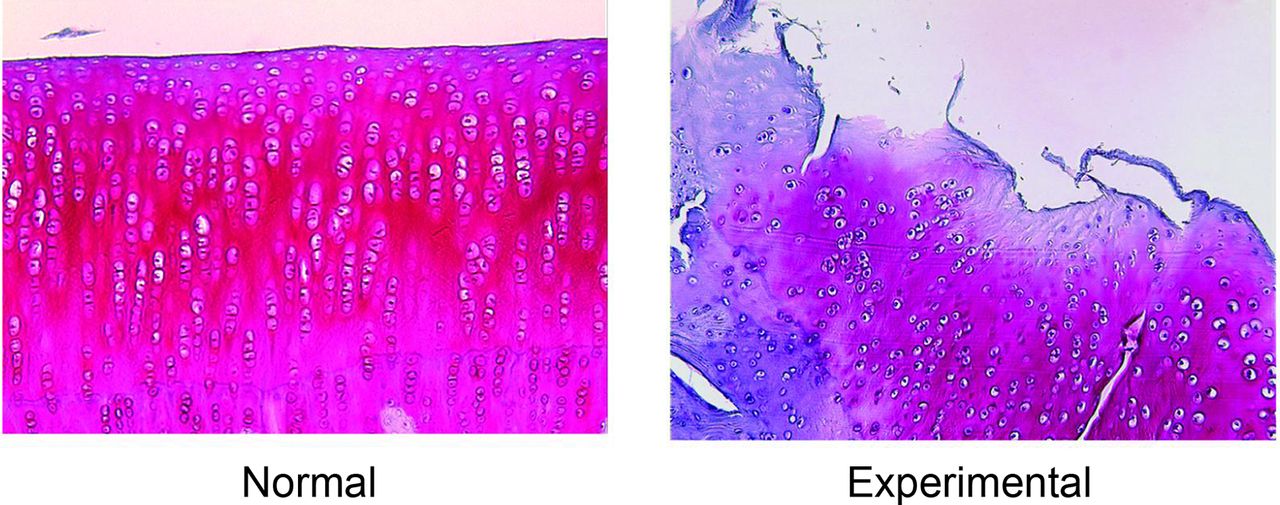
Histological evidence of the onset of knee OA in a rabbit model of botulinum toxin type-A induced muscle weakness (knee extensor muscles were weakened systematically to 20% of their original strength). Note the disruption of surface integrity, the loss of homogeneous staining and the disruption of cellular structure in the cartilage 4 weeks after the onset of muscle weakness (right panel) compared with a normal strength control animal (left panel). Similar results were also observed at 8 and 12 weeks post muscle weakness induction. OA, osteoarthritis.
Lessons learnt: muscle (quadriceps femoris) weakness is an independent risk factor for the onset and possibly the rate of progression of knee OA (in the rabbit). Furthermore, knee extensor muscle imbalance results in knee OA despite no apparent changes in PF tracking and/or contact pressure distributions. Healthy and balanced muscle function seems essential for good joint health.
Diet-induced obesity and OA
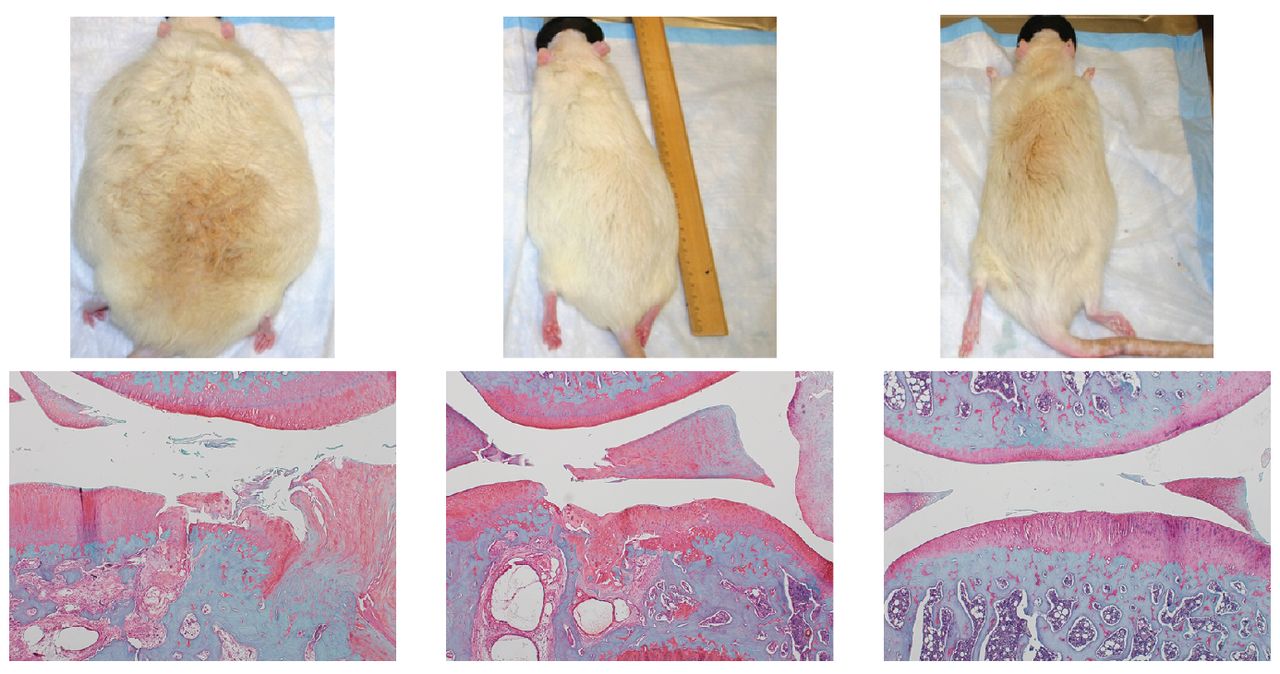
A high-fat, high-sucrose (HFS) diet leads to differential obesity in Sprague-Dawley rats44 (figure 3). This outcome is insofar beneficial, as it has been argued that obesity causes knee OA in humans because of increased body weight alone. An obesity model of ‘normal’ body weight might help determine if knee OA is indeed associated with the gain in body weight. Therefore, we asked the question: is body weight or obesity responsible for knee OA?

Exemplar rats with high body fat and high weight (left), high body fat and normal weight (middle) and normal body fat and normal weight (right) and associated exemplar histological samples of the knee following 28 weeks on a HFS diet (left and middle rats) and a normal control diet (right rat). Note that the severity of knee joint degeneration is similar in the rats with the high percentage of body fat (left and middle), despite unequal body weight, while joint degeneration is substantially greater in the middle compared with the right rat despite similar body weight but unequal body fat percentage. HFS, high-fat, high-sucrose.
Following 28 weeks of exposure to the HFS diet, all animals showed increased OA development in the knee compared with control animals fed a regular diet44 (figure 3). This finding was independent of the amount of body weight but only depended on the per cent of body fat, illustrating that it is obesity that causes OA onset and progression and not body weight. Inflammatory profiles reflected a metabolic subtype of OA with multiple significant relationships between inflammatory markers and Mankin scores, an indicator for knee OA.44 45 Furthermore, we found that the rat vastus lateralis showed increased intramuscular fat content and fibrosis within days following the onset of an HFS diet, suggesting that diet can affect muscle integrity and function quickly46 (figure 4).
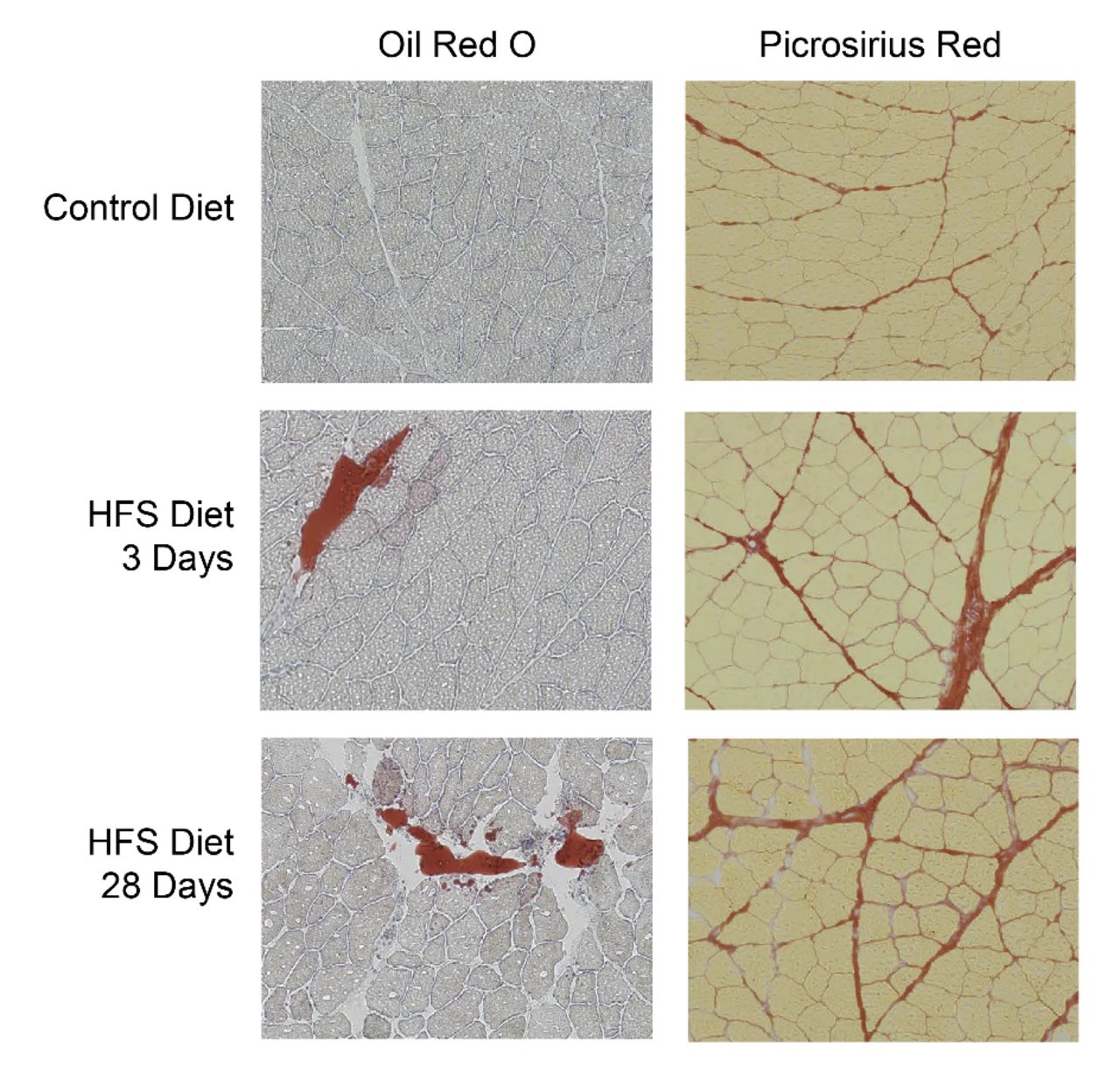
Exemplar histological samples of intramuscular fat (assessed using Oil Red O staining; left panel) and fibrosis (assessed using Picrosirius red staining) in control animals on a regular diet (top panel), and for animals on an HFS diet at 3 days and 28 days following onset of the diet intervention. Note the (statistically significant)1 increase in intramuscular fat and fibrosis within 3 days of the HFS diet intervention. HFS, high-fat, high-sucrose
Lessons learnt: obesity is an independent risk factor for the onset and increased rate of knee OA progression in Sprague-Dawley rats. OA onset and progression depend crucially on the percentage of body fat. An HFS diet affects the knee and has immediate effects on muscle structure and integrity that, in turn, might affect joint health.
The human model
Much of the discussion on progression of knee OA depends on how we define progression. Studies to date tried to identify patients with disease progression mostly based on the assessment of structural progression detected on radiography (joint space narrowing) or the amount of cartilage loss detected on MRI.47–51 As an alternative to structural changes for monitoring progression of knee OA, clinical and functional markers may provide a useful substitute, as it is dealing with patients who have sought medical care for their symptoms.
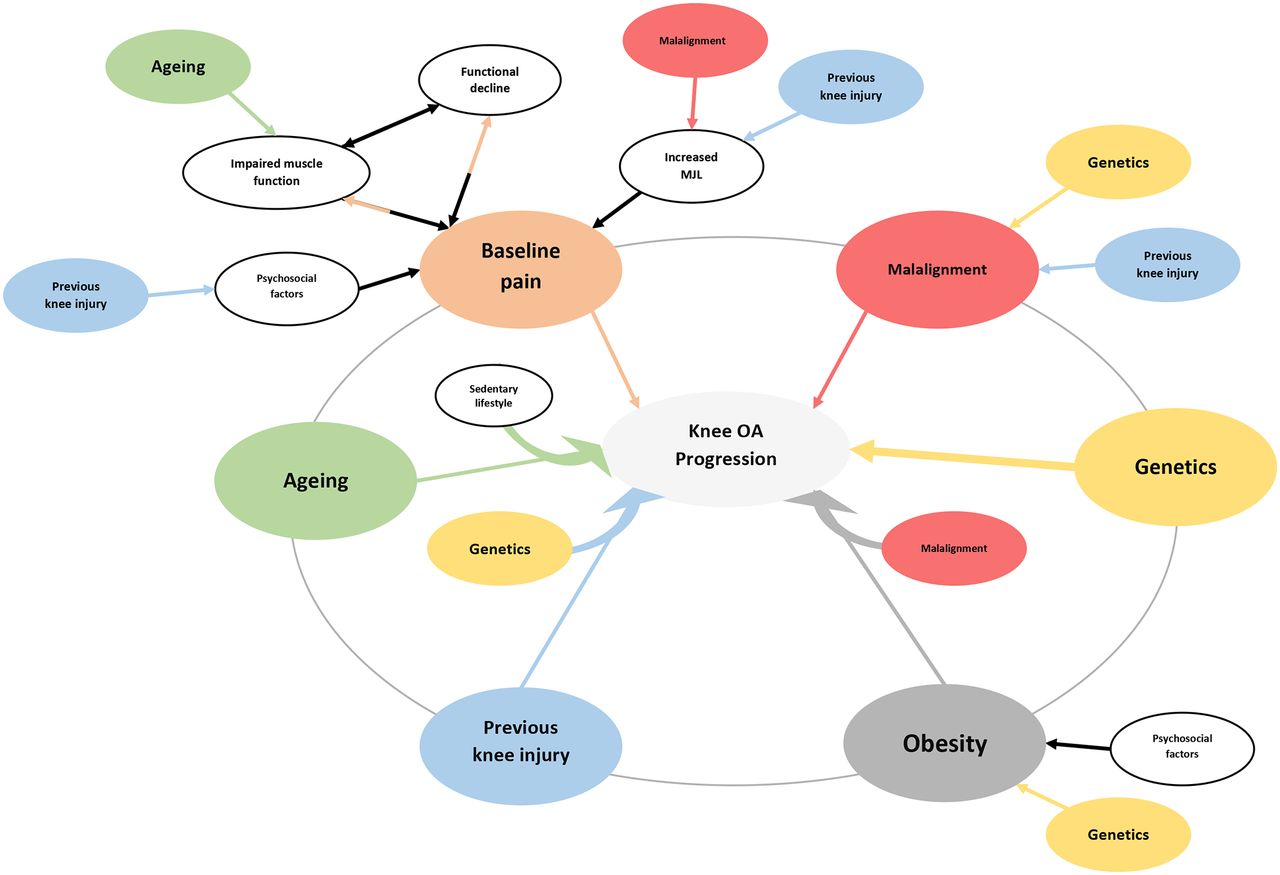
The most predictive set of factors associated with progression of knee OA are briefly summarised in figure 5. We are aware of the fact that this is not necessarily the same in an early knee OA population versus established knee OA, but since we consider the disease process as a continuous one, with intermittent periods of no or little clinical signs/symptoms, key risk factors are probably not that different depending on the stage of the disease process.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Schematic diagram illustrating factors associated with progression of knee OA and their interactions. Stronger associations are shown schematically with thicker arrows. Age: conflicting evidence is found in the relationship between age and progression of knee OA.102 Possible role of sarcopaenia, an age-associated loss of skeletal muscle mass and a major factor in the strength decline with ageing should also be considered.103 104 Obesity: the possible effect of obesity on progression of knee OA, in human models, has been supported by some studies.105–108 Static (in the context of genetic traits) and dynamic knee joint alignment s: have also been associated with progression of knee OA.106 109 Moreover, as reported by Felson et al, the effect of body weight on progression of knee OA is affected by alignment.110 Genetic predisposition: is well established, and several genes have been identified as risk factors for the incidence and progression of knee OA.111–113 Genetic predisposition might be a key difference between a patient who sustained a traumatic knee injury and fully recovers and a patient who develops early OA as a result of similar injury.114 A patient with predisposed malaligned knee will have a higher risk of progression compared with his ot her counterpart with neutrally aligned knee. P ain at baseline: the effect of pain on progression of knee OA is of major importance as it itself could modify or be modified by several other factors like: muscle inhibition, psychosocial factors, increased medial knee joint loading. Previous history of knee joint injury: has also been associated with increased risk of progression of knee OA.47 115 Previous injury could also be related to the progression of knee OA via its mediating effects on psychosocial factors (kinesiophobia116) and knee joint alignment. MJL, medial joint loading; OA, osteoarthritis.
Lessons learnt: taken together and understanding the limitations of the existing scientific evidence, one could postulate that clinical risk factors in early knee OA include ageing, genetic traits, preceding traumatic events, obesity, intensity of pain at baseline, static and dynamic joint malalignment, and reduced muscle strength. Importantly, additional factors that will further determine the management plan includes an assessment of the psychosocial context of the patient, the professional and recreational activities and expectations. A standard assessment of the above parameters will help to identify the patient at high risk with a need for more active patient management, as discussed below.
Secondary prevention of early knee OA
As discussed above, there is quite some information on indicators/predisposing factors available to identify the patient and patient profiles with early knee OA and at risk of progression. We believe we need to focus on these patients with high-risk early knee OA and design an individualised management plan based on more in-depth patient profiling. We envision the patient being detected in primary care as at risk based on a specific algorithm that needs to be developed but comparable with some assessment as used to detect patients with high-risk profile for cardiovascular incidents or osteoporotic fractures.52 The degree and thoroughness with which this should be done needs to be explored, but a user friendly screen in primary care is imperative, and a more thorough advanced assessment in second line seems relevant.53 Advanced profiling should include a full anamnesis probing for pain/symptoms and signs based on validated scales and within the biopsychosocial context of the patient; further functional performance (both subjective and objective), quality of life assessment, genetic traits by family history, sedentary behaviour, professional and recreational activities and expectations. Management will focus on self-management programme including: education regarding disease perception and drug use, non-pharmacological pain relief approaches, role of exercise and adapting lifestyle, physical activities, and last but not least, weight control. Besides coaching, the management will need to include clear delivery strategies such as stepped care, shared decision processes, systematic use of wearables and applications. Finally, to achieve a feasible individually tailored intervention, we need to include personal coaching, adaptation in exercise and/or activity participations (aerobic conditioning, muscle strength training, and neuromuscular exercise) and safe weight reduction/weight control strategies.
Although poor level of evidence is currently available on OA self-management measurement properties, we suggest to simply assess patient’s self-management prior to the intervention. All prototypical patients could be assessed on attitudes and capabilities regarding self-management. The Perceived Efficacy in Patient-Physician Interactions54 55 (PEPPI-5) for instance, assesses a discrete aspect of self-management and points out self-efficacy of patients with OA to interact with their physicians.55
If the latter results in a poor perceived efficacy to interact, one should provide early coaching possibly to extend supportive social context to manage expectations and motivational interviewing before any interventional programme is initiated. When the patient’s self-efficacy to interact is ‘good to satisfying’, one can directly start to actively involve the patient in shared decision-making process and to act along with the mutual interventional short-term goals set.
As an illustration, we will discuss below what we believe are prototypical patients and what we propose at this point could require additional investigations and a valuable treatment and management plan.
Profile 1: post-traumatic 20-year-old patient returning to competitive sport with high reinjury risk
Previous knee injury could be considered, in this case, as a risk factor for development of early knee OA. For such profile, the key would be to increase insight of the patient’s high-risk profile and create an urge to change the patient’s provocative persistence behaviour. An immediate coaching towards alternative lower risk and quickly enjoyable sport participation is recommended.35 43 56 Once a progressive criteria-based rehabilitation is initiated, patient’s knee reactivity is the main parameter to take into account. If the patient still prefers to participate in a high impact sport (non-anticipated changes in directions at high speed), a neuromuscular training regimen should be added to the exercise routine. Health benefits of being physically engaged in daily recreational and social activities will certainly help slow down the subclinical progression in early knee OA.57 For example, if daily running is moderate (>4 km at slow speed, assertive cadence), and gradually progresses without signs of knee swelling at the end of the day, we assume beneficial functional and even chondro-protective adaptations.58 59
Profile 2: post-traumatic early knee OA in 30-year-old male
Regarding a 30–40-year-old male patient with posttraumatic early knee OA, one should analyse more thoroughly the risk profile. Post-traumatic can range from major intra-articular trauma to arthroscopic partial meniscectomy. Following traumatic events, the joint structure is affected, and biomechanical loading will be changed. Small uncompensated changes in arthrokinematics,60 for example, due to a medial shift in loading, will cause the more vulnerable cartilage-bone unit to suffer and may lead to progressive degeneration by increase in local contact pressures.61 If family traits are a concern, one should target for establishment of a healthier lifestyle with therapy sessions at low frequency. If the occupation involves intense lower limb loading of the lower limb, direct help to change the job or adapting the workload is a necessity, before absenteeism overrules job commitments.
Since the influence of body mass index (see above), in contrast to obesity, in early OA is not clearly established, we pragmatically question weight change in the history of patients with post-traumatic early knee OA in this age group. If the current weight exceeds patient’s weight in early adulthood with more than 10 kg, we interpret body weight as a possible risk factor.62 Since the knee in this situation already or in the near future encounters physiological overload, it is recommended to coach patient towards healthier eating habits in order to control and if necessary reduce weight.
Although this age group is supposed to potentially represent an active lifestyle, sedentary behaviour and low participation rates in moderate to intense activities may be observed. Changing physical activity behaviour and improving (1) the lower limbs and core muscle strength, (2) aerobic fitness, and (3) neuromuscular agility could be of interest. It is unclear if all these training goals should be addressed; however, supervised group sessions are favourable, safe and recommended.63 Whereas physical activity is good for general health and therefore a necessity, exercise therapy involves systematic training with specific therapeutic goals. In patients with early knee OA, the purpose can be formulated as ‘to restore normal musculoskeletal function or to reduce nociceptive pain caused by disease or injuries of the knee’. The abovementioned three major training goals are shown to be effective to improve function and provide pain relief in established knee OA. We assume this to be no different in early knee OA if patient’s complaints are defined as dominantly nociceptive pain.64
Profile 3: early knee OA in a 50-year-old female or male with varus malalignment and family history of knee prosthesis
In this prototypical patient, the two risk factors, malalignment and genetic predisposition, are combined and interpreted as prognostic for the development and progression of knee OA. Both dynamic and static varus malalignments may significantly contribute to cartilage degeneration medially in knee OA.65 66 We assume that even for patients with normal static alignment but accompanied varus thrust, gait modification therapies might be beneficial. Several gait modifications, aiming to reduce medial knee compartment loading, have been studied experimentally to prevent progression of knee OA. Two major methods are studied to reduce the knee adduction moment. The first method tries to reduce the overall ground reaction force by lowering gait speed or partially shifting the weight on the arms by use of poles.67 68
The second gait-modifying method aims to reduce the Knee Adduction Moment (KAM) by shortening the lever arm of the Ground Reaction Force (GRF) in the frontal plane. The most common techniques are: (1) toe-out and toe-in gait,69–71 (2) increasing the ipsilateral trunk lean,72–74 and (3) increasing medial knee thrust during landing.74 The latter two showed clearly the highest potential to improve gait kinetics and decrease medial compartment loading.74 Importantly, the authors highlighted that selection of individual-specific gait modification and the timing of the modification seems vital to optimise knee kinematics.75 (4) Modified footwear strategies are also found to reduce medial compartment loading in patients with medial knee OA.76 Shakoor and Block76 demonstrated that the peak joint loads significantly decreased during barefoot walking, in both hip and knee joints of patients with knee OA. Paterson and colleagues77 found significant reductions in peak KAM and KAM impulse using flat flexible shoes compared with any other types of stable supportive shoes. Moreover, the use of stable supportive shoes even increased both peak KAM and KAM impulse.77 Additionally, the use of lateral-wedge insoles has also been proven to be effective in reducing the (knee) medial compartment loading in persons with medial knee osteoarthritis.78 The abovementioned gait modifications list is not complete but79 80 overall gait modifications seem promising, underused and low-cost interventions that might help preventing the progression of knee OA. Whether these modifications in gait studies show long-term effectiveness needs further evaluation. Side effects of gait modification strategies, such as discomfort and decreased balance, are occasionally reported and need to be taken into account.
Although quadriceps strengthening is the cornerstone of exercise therapy in most knee OA management regimens, in this specific profile of knee OA patients, it has to be prescribed with caution. In this type of patients with malaligned knees, the distribution of forces are not even, and an increase in muscle contraction might result in higher joint reaction forces, which could be harmful for the joint.81 Evidence up to now is lacking to identify the window of opportunity for corrective surgical osteotomies in the treatment trajectory in early knee OA.
Profile 4: early knee OA in postmenopausal 55-year-old overweight female with sedentary behaviour
Although at first glance obesity and ageing could be considered as the primary risk factors here, this prototypical patient presents multidimensional risk factors and probably will even have an additional risk to develop chronicity of pain. All risk factors need to be addressed by therapeutically reassuring approaches. This implies proper drug treatment to support pain relief, such as paracetamol and intermittent non-steroidal anti-inflammatory drugs (NSAIDs),82 referral to specific programmes and involvement of other health professionals.
Unfortunately, many clinicians perform history taking and screening for musculoskeletal pain mainly based on biomedical and somatic features. Moreover, many feel unprepared to treat patients with chronic pain by exploring the psychosocial factors that influence recovery.83 History taking using the Somatic–Cognitive–Emotional–Behavioral–Social (SCEBS) method could be of great help. Since it is easy and fast, it helps to change management and directs to well-known barriers to recovery.84 85 The SCEBS method identifies: (1) the somatic or biological, (2) the psychological, and (3) the social dimension of pain. A set of questions traces impairments of movement-related function, catastrophic or helplessness cognition, fear of pain, lack of self-efficacy or unrealistic treatment expectations, depression or anxiety, avoidance behaviour or pain resistance behaviour and maladaptive social responses to pain behaviour (the detailed SCEBS can be seen in online supplementary appendix 1 86).
Supplemental material
Following the biopsychosocial clinical assessment, one should summarise the multifactorial knee OA risk profile including those related to pain. If the patient was able to express himself or herself properly, you start the therapy by summarising the patient’s needs and expectations expressed in each domain. Next, in the shared-decision process, the patient prioritises together with the team of healthcare professionals will decide the preferred actions and help the patient by formulating realistic time bonded goals, again in each domain. As such, we hope to strengthen patients to change their movement behaviour.87 Practically, the patient could be referred to well-trained professionals acting in line with a knee OA care pathway, including support for self-management, education, exercise and weight control. For the latter, this prototypical patient is a good example. Evidence shows that weight loss is achievable, but maintenance of the reduced weight is the real challenge.88
Profile 5: early knee OA in a 52-year-old female or male with no obvious clinical risk factors and no radiographic abnormalities
Particularly, in this prototypical patient, we assume other underlying causes for the pain described in the knee. Therefore, many clinicians will suggest further technical investigations and overuse them. In other words, a stepped care strategy is uttermost important. Outcome superiority of a specific implementation is not proven, but most recommended nonsurgical modalities seem to be well used if care is implemented by protocol. These interventions also point out that patients with a passive coping style should be encouraged more to use non-surgical treatments such as supportive medication combined with exercise therapy (aerobic, strengthening and neuromuscular) and behavioural approaches to improve self-management.89 90 A reassuring ‘demedicalisation’ approach of primary healthcare professionals in first line is warranted. Relative short-term follow-up (within 3 months) to reassess needs and steps is recommended.
Discussion and future directions
There is little doubt that there are plenty of opportunities when looking into secondary prevention and early knee OA. Very little is done in a structured way for these patients, and it is time to invest resources into an individual patient-centred approach as OA is a serious disease, and the impact of knee OA on the patient is very sizeable in many aspects of his or her daily, recreational, and professional life. Therefore, we believe secondary prevention is the key. Yet, as the sheer number of patients with this early disease process is large, we have to set up a structured approach allowing to detect early knee OA in primary practice and provide appropriate coaching depending on the (risk) profile of the patient. This is much in line with other chronic musculoskeletal diseases such as rheumatoid arthritis and osteoporosis. Besides the fact that defining and classifying early knee OA allows much needed interventional studies in early phases of the diseases process,5 it should also trigger a cascade of events in clinical practice leading to a proper patient-centred management.
Indeed, most patients with nociceptive, activity-dependent knee pain are getting the message that with normal blood exam and normal X-rays, nothing can be done, but symptomatic pain relieve by paracetamol and NSAIDS as no disease-modifying drugs are available. This attitude needs to be replaced by a more personalised patient approach like characterisation of the patient by many angles including the biopsychosocial factors. This is feasible by screening methods and algorithms implemented via most modern technologies such as computerised decision support systems allowing to guide both the physician and patient to take proper action. Importantly, this approach should also allow to classify a patient in a risk category, and when the risk is high for progression suggesting to refer the patient to more advanced multidisciplinary centres where in-depth assessment of his or her individual profile will result in a personalised approach and coaching with examples as discussed above.
Indeed, in this expert centre, typically a multidisciplinary team with orthopaedic surgeon/rheumatologist/rehabilitation doctor next to a physiotherapist, dietitian, psychologist and other relevant non-medical partners, will review the diagnosis, assess the patient profile as comprehensive as possible, elicit patient’s expectations and propose using a shared decision process to achieve relevant management goals.
In doing so, it is still a challenge today to understand the risk profile of the patient and its relation to prognosis. Much research still needs to be done in this regard to come up with an algorithm to evaluate the risk profile of the patients at higher risk of disease progression. Indeed, the relationship and interplay between many identified risk factors and how these factors quantitatively interact and affect diseases outcomes remains a major research task (figure 5).
Specific pitfalls in management of the patient with early knee OA need to be addressed. We should avoid introducing MRI as a necessary investigation to define and classify the patients as early knee OA. Although MRI is more accessible, it cannot be recommended in the first line of early knee OA diagnosis. Moreover, MRI findings and their interpretation may contribute in some patients to a distorted disease perception that leads to chronicity. Second, early imaging as observed in patients with low back pain may increase and extend disability91 92 and be associated with decreased sense of well-being.93 Overall, a review on diagnostic testing suggests that the reassuring potential of investigations is only of value for a serious disease.94 So, one should rely on clinical findings, inform and refer patients at consultations in a more reassuring way, for instance physical therapy, based on clinical findings, that has demonstrated to be of benefit, without any known risk for the patient.63 95 96
Another pitfall would be ‘overtreatment’ in a patient who is not responding to the first-line management. It is quite often that the patients experience specific insurmountable barriers at the very start of the treatment. Therefore, a re-evaluation of barriers and facilitators is necessary in order to personalise the initial treatment plan. Additionally, adherence to exercise is often reported to be low and decline over time that becomes problematic as it is identified as a predictor of the long-term effectiveness of exercise therapy.97–99 There is also the discussion on relevant outcomes in this regard but that is somewhat outside of the scope of this paper. Last but not least, as reported by Choi et al, 100 in studying risk factors associated with development of rheumatic conditions and their complications, one should consider that the discrepancies in predictors for development and progression could be explained by index event bias.
As mentioned before, we are fully aware of the limitations of our discussion. This narrative was limited, to some extent, in addressing all the recent developments on prevention of pain chronicity, educational approaches, programme implementation and continuation and non-pharmacological modalities, which are already available in several guidelines.82 101 To conclude, the ultimate goal of secondary prevention for patients with early knee OA should be to restore joint homeostasis and recover full function in all activities. It may require appropriate adjustments, targeting to increase quality of life, and prevention or slowdown of structural deterioration over time. To achieve this, the approach should be personalised and the attention focused on modifiable factors in the broad context. We also believe it is affordable, more clinically relevant and of real value for the patient and the society. As in many countries, there is not sufficient appreciation for the merit of a management trajectory for an individual patient with early knee OA; this approach may require adaptations for the reimbursement policies. In doing so, this will decrease substantially the OA disease burden.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- 108.↵
- 109.↵
- 110.↵
- 111.↵
- 112.↵
- 113.↵
- 114.↵
- 115.↵
- 116.↵
Footnotes
AM and DVA are joint first authors.
Contributors All authors contributed equally to this paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Commissioned; externally peer reviewed.