Article Text

Abstract
Background Patients with immune-mediated rheumatic diseases (IMRDs) are commonly treated with immunosuppressors and prone to infections. Recently introduced mRNA SARS-CoV-2 vaccines have demonstrated extraordinary efficacy across all ages. Immunosuppressed patients were excluded from phase III trials with SARS-CoV-2 mRNA vaccines.
Aims To fully characterise B-cell and T-cell immune responses elicited by mRNA SARS-CoV-2 vaccines in patients with rheumatic diseases under immunotherapies, and to identify which drugs reduce vaccine’s immunogenicity.
Methods Humoral, CD4 and CD8 immune responses were investigated in 100 naïve patients with SARS-CoV-2 with selected rheumatic diseases under immunosuppression after a two-dose regimen of SARS-CoV-2 mRNA vaccine. Responses were compared with age, gender and disease-matched patients with IMRD not receiving immunosuppressors and with healthy controls.
Results Patients with IMRD showed decreased seroconversion rates (80% vs 100%, p=0.03) and cellular immune responses (75% vs 100%, p=0.02). Patients on methotrexate achieved seroconversion in 62% of cases and cellular responses in 80% of cases. Abatacept decreased humoral and cellular responses. Rituximab (31% responders) and belimumab (50% responders) showed impaired humoral responses, but cellular responses were often preserved. Antibody titres were reduced with mycophenolate and azathioprine but preserved with leflunomide and anticytokines.
Conclusions Patients with IMRD exhibit impaired SARS-CoV-2 vaccine immunogenicity, variably reduced with immunosuppressors. Among commonly used therapies, abatacept and B-cell depleting therapies show deleterious effects, while anticytokines preserved immunogenicity. The effects of cumulative methotrexate and glucocorticoid doses on immunogenicity should be considered. Humoral and cellular responses are weakly correlated, but CD4 and CD8 tightly correlate. Seroconversion alone might not reflect the vaccine’s immunogenicity.
- COVID-19
- vaccination
- autoimmune diseases
- immune system diseases
- T-lymphocyte subsets
Data availability statement
Data are available in a public, open access repository. Not applicable.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Immunogenicity to common vaccines is compromised in IMRD under immunosuppressors.
SARS-CoV-2 mRNA vaccines are highly effective in healthy people.
What does this study add?
In patients with IMRD vaccinated with SARS-CoV-2 mRNA vaccines:
Immunogenicity was reduced at different degrees and at different points of the immune response depending on the therapies used.
A weak correlation between elicited humoral and cellular responses, but strong correlation between CD4 and CD8 T-cell responses, were observed.
How might this impact on clinical practice or further developments?
In immunosuppressed patients with IMRD, measurement of cellular immune responses might be necessary to fully evaluate vaccinesvaccine’s efficacy.
Introduction
Patients with immune-mediated rheumatic diseases (IMRDs) are considered at-risk for serious infections as a result of the underlying dysregulation of their immune system and the common use of targeted immune-modulating therapies and immunosuppressors.1 On the scenario of the global SARS-CoV-2 pandemic, recent data indicate that patients with rheumatic diseases with low/moderate disease activity on monotherapy, but steroids, are not at a higher risk of severe manifestations of COVID-19.2 3 In fact, the use of downstream anti-inflammatory immunomodulating therapies such as anti-TNF, JAK inhibitors, anti-IL-1 and IL-6 inhibitors can have a beneficial effect on the management of pathological immune responses, including cytokine storm developed in the context of severe COVID-19.4–6 On the contrary, B-cell and T-cell depleting therapies in selected populations of patients have been associated with severe or prolonged SARS-CoV-2 infections.7 8
The COVID-19 pandemic should be overcome by the recent introduction of the new genetic SARS-CoV-2 vaccines. Because of its reported unprecedented high effectiveness and safety, these vaccines—mRNA and adenoviral vector vaccines—are a major scientific breakthrough that will probably change current vaccine practices in a near future. Because they supply to recipient’s own cells the information to produce exogenous proteins, unmodified native antigen presentation by HLA I and II molecules to the immune system follows physiological routes.9 Perhaps this feature underlays its high effectiveness across all ages. But the exact correlate of the elicited immune responses that confers protection against infection is not yet fully known.10
Immunosuppressed patients were excluded from phase III trials of the mRNA vaccines currently approved by the EMA and FDA.11 12 The management of IMRD typically requires immunosuppressive medications and biological agents to achieve and maintain disease remission. Because of its novelty, scant information is nowadays available on mRNA vaccine responses in patients with IMRD. However, it is well-known that older age, high dose steroids, high inflammatory activity index and immunosuppressive therapies are associated with decreased responses to conventional vaccines.13 Here, we report exhaustive B, T CD4 and CD8 immunogenicity data after completing mRNA SARS-CoV-2 vaccination in 110 immunocompromised patients with IMRD under active immunosuppression and compare them to 50 immunocompetent patients with the same diagnosis and with 50 healthy controls.
Methods
Design
Longitudinal observational study conducted at Complejo Asistencial Universitario of León (Spain) between April and July 2021 to characterise the immune response to mRNA SARS-CoV-2 vaccines in patients with IMRD and determine the influence of immunosuppressive and biological therapies in the elicited immune response. The study was conducted according to the principles of the Declaration of Helsinki and approved by hospital’s institutional ethics committee.
Study population
We performed a consecutive sampling on the available IMRD population >18 years from CAULE’s rheumatology outpatient clinic. One hundred and sixty patients with IMRD with low/moderate disease activity index and twice vaccinated with an mRNA SARS-CoV-2 vaccine were selected according to disease and treatment. Selected diseases included rheumatoid arthritis (RA), systemic lupus erythematosus (SLE), systemic sclerosis (SS) and Sjogren’s disease (SJ). Patients were classified into two groups: 110 actively receiving immunosuppressive therapies (cohort 1, IMRD ISP+), and 50 disease, age and gender-matched patients with IMRD without active immunosuppression for the last 2 years (cohort 2, IMRD ISP−). Both IMRD cohorts were compared with another cohort of 50 healthy vaccinated controls from healthcare personnel (cohort 3).
On the basis of composite objective factors (online supplemental material 1), cohort 1 (IMRD ISP+) was defined as patients actively receiving one or more conventional synthetic disease modifying antirheumatic drugs (ie, methotrexate (MTX), leflunomide (LFM), azathioprine (AZA), mycophenolate (MFM)) and/or biological disease modifying antirheumatic drugs (bDMARDs) such as CTLA4-Ig (abatacept), BLyS inhibitor (belimumab (BMB)) and anti-CD20 antibody (rituximab (RTX)). Cohort 2 (IMRD ISP−) was defined as patients with the same IMRD receiving non-steroidal anti-inflammatory drugs, antimalarials and/or bDMARDs blocking effector inflammatory cytokines such as anti-TNF (adalimumab, certolizumab, etanercept, golimumab, infliximab), IL-6 inhibitors (sarilumab and tocilizumab) and IL-1 inhibitors (anakinra).
Supplemental material
General exclusion criteria were previous serologically or PCR confirmed COVID-19, vaccination with any other SARS-CoV-2 vaccine, and in the control cohorts, a history or immunosuppressive treatment during the previous 2 years.
The following variables were recorded: (1) age, (2) gender, (3) type of rheumatic disease, (4) brand of vaccine administered, (5) time since diagnosis, (6) accumulated treatments during the previous 2 years, (7) cumulative dose of glucocorticoids and MTX during the previous 2 years and (8) in RTX-treated patients, time since last infusion.
Vaccination procedure
All patients received a two-dose regimen of an mRNA vaccine (either mRNA-1273 or BNT162b2, online supplemental material 2). Patients were first assessed at the rheumatology office within 2 weeks prior to vaccination and blood samples collected after at least 3 weeks (mean 37 days) of complete vaccination at the immunology laboratory.
Supplemental material
Assessment of humoral responses
Humoral vaccine response was evaluated by means of SARS-CoV-2 Trimeric S IgG assay (Dia-Sorin). A value above 33.8 binding antibody units (BAU/mL) was considered positive, according to the manufacturer’s instructions.
Assessment of cellular CD4 and CD8 responses
Cellular CD4 and CD8 responses were analysed in vitro in freshly isolated peripheral blood lymphocytes (PBL) after stimulation with a peptide pool spanning the entire SARS-CoV-2 spike glycoprotein (S) (Miltenyi Biotec) plus anti-CD28. After 18 hours stimulation with S-peptide or control, IL-2, IFN-γ, Granzyme A and Granzyme B were quantified in culture supernatans (CBA, Becton-Dickinson). For each cytokine, a 2× increased level above individual’s basal were considered positive.
A CD4 T-cell positive response was stringently defined by a combined IL-2 and interferon-γ response to S peptides (Th1 response). A CD8 T-cell positive response was defined by a combined granzyme A/B and interferon-γ response to S peptides.
To rule out unrecognised previous SARS-CoV-2 infection, simultaneous isolated stimulation with a peptide pool spanning the entire SARS-CoV-2 nucleocapsid glycoprotein (N) (Miltenyi Biotec) was performed. Any participant with a cellular response to N was excluded from the analysis.
Statistical analysis
Categorical variables were reported as percentages, whereas continuous variables were expressed as median and IQR values. Where appropriate, Mann-Whitney U and Kruskal-Wallis tests were used to assess the difference between groups. Categorical variables were compared by using contingency tables, and p values calculated with χ2 or Fisher’s exact tests, when appropriate. Sequential multivariate analysis of factors influencing vaccine responses (B-cell, CD4 and CD8) were performed by linear regression analysis. Those covariates showing a p value <0.2 in univariate analysis were included in the models. P values of less than 0.05 were considered to indicate statistical significance. All p values presented are two sided. The following variables were included: age >65 years, sex, disease duration (>5 years and >10 years), diagnosis, treatment with antimalarials, anti-TNF monotherapy, MTX monotherapy, IL-6i monotherapy, cumulative glucocorticoids, anti-TNF monotherapy, IL-6i+MTX, RTX, RTX+MTX, abatacept, BMB, BMB+MTX, MFM, AZA. Analysis was performed using SPSS V.12.
Results
Demographic characteristics
A total of 160 patients with IMRD (110 ISP+, 50 ISP−) and 50 healthy controls with the two-dose regimen were enrolled (figure 1). After analysis, 10 patients from cohort 1 (IMRD ISP+) and 3 patients from cohort 2 (IMRD ISP−) were excluded on the basis of previous unrecognised COVID-19 infection. The final analysis included 100 patients from cohort 1, (42 RA, 32 SLE, 12 SJ and 14 SS), 47 patients from cohort 2 (13 RA, 12 SJ, 10 SS and 12 SLE) and 50 healthy healthcare workers.

Study overview. AZA, azathioprine; BMB, belimumab; BMB+MTX, belimumab+methotrexate; CQ, chloroquine; HCQ, hydroxychloroquine; IL-6i, IL-6 inhibitors; LFM, leflunomide; MFM, mycophenolate; MTX, methotrexate; RA, rheumatoid arthritis; RTX, rituximab; SJ, Sjogren; SLE, systemic lupus erythematosus; SS, systemic sclerosis.
Immunogenicity of mRNA vaccines in patients with IMRD
Humoral responses were evaluated by quantifying serum IgG antibodies to SARS-CoV-2 spike protein. All healthy controls (50/50, 100%) demonstrated seroconversion, whereas patients with IMRD ISP− and patients with IMRD ISP+ achieved seroconversion rates of 80% (p=0.03) and 55% (p=0.02), respectively. Median IgG titres for healthy controls were 526.3—IQR 2078, 458.6—IQR 2960 (p=0.18) for cohort 2, and 254—IQR 280 for cohort 1, which averaged an almost twofold reduction in antibody titres in patiets with IMRD ISP+ compared with patients with IMRD ISP− (p=0.0072). Therefore, we concluded that having an IMRD slightly reduced elicited humoral response, that was more compromised with immunosuppressors (table 1)
Sociodemographic characteristics, humoral and cellular responses from cohort 1 (immunosuppressed IMRD ISP+), cohort 2 (immunocompetent IMRD ISP−) and cohort 3 (healthy controls)
CD4 and CD8 cellular immune responses were assessed in vitro after stimulation of PBL with S-peptides. A complete functional Th1 response consisting of IL-2 and interferon-γ production (a surrogate of Th1 response) was present in all 50 healthy controls (100%), in 35 patients with IMRD ISP− (75%) (p=0.002) and in 52 patients with IMRD ISP+ (52%) (cohort 1 vs cohort 2, p=0.01). Functional T CD8 responses consisting of S-induced Granzyme A/B detection in supernatants were observed in 46/50 healthy controls (92%), whereas 77% and 53% from IMRD ISP− and IMRD ISP+ showed positive responses (p=0.04 and p=0.01, respectively) (table 1). Therefore, we concluded that patients with IMRD exhibit decreased cellular immune responses to the vaccine, that decreased even more under immunosuppression.
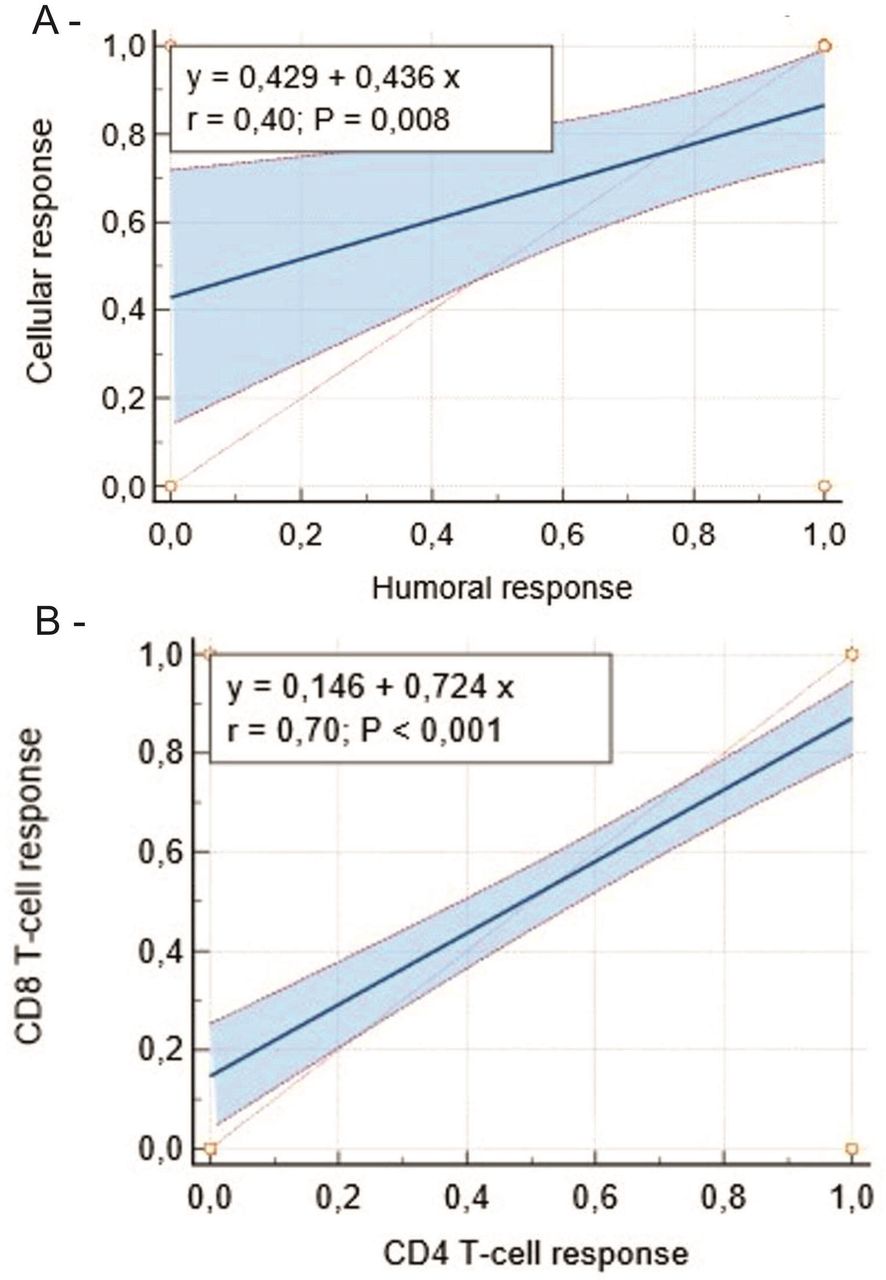
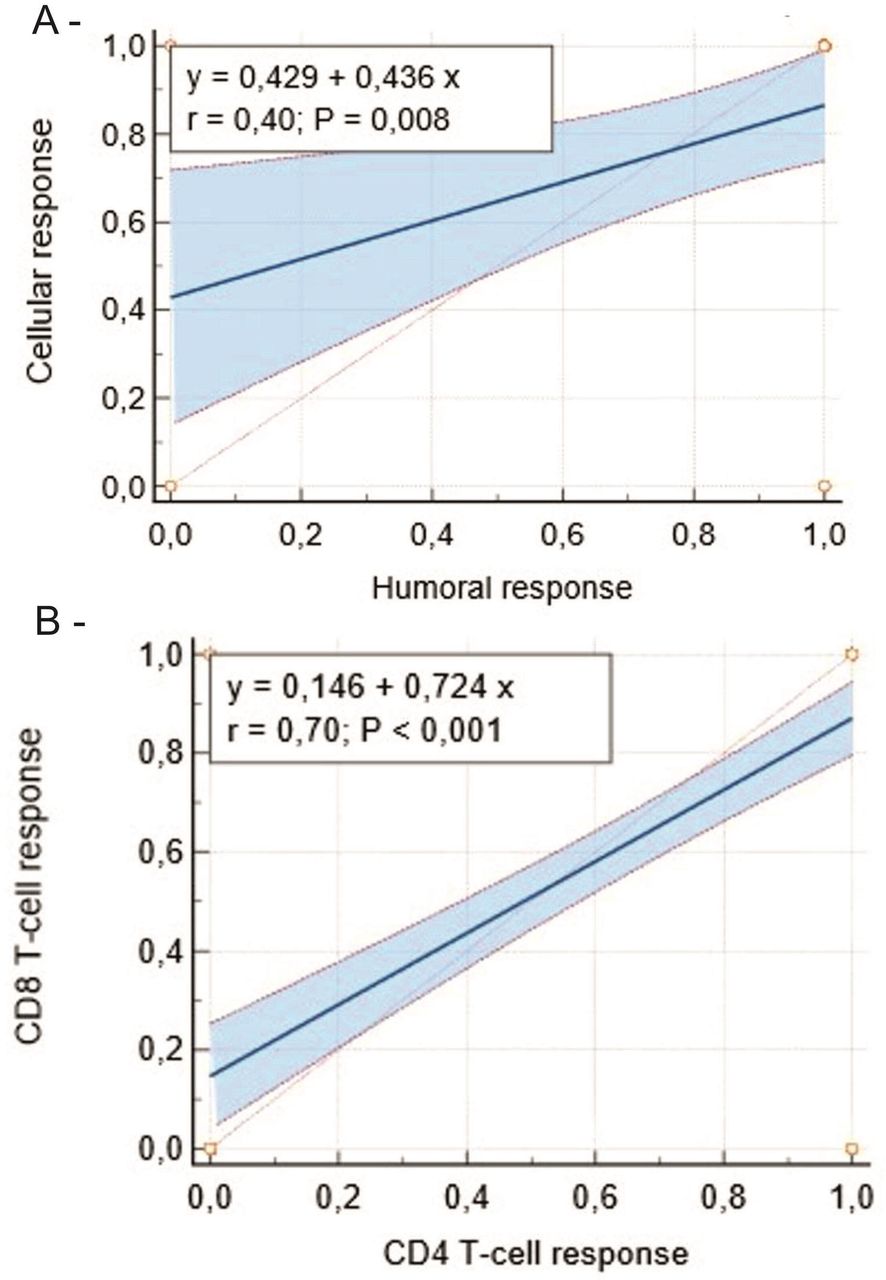
A correlation between humoral and cellular immune responses has been described in healthy individuals infected with SARS-CoV-2.14 We assessed the correlation between humoral and cellular responses in patients with IMRD with/without active immunosuppression, and found weak correlation (r=0.40, p=0.008) (figure 2A). On the contrary, a strong correlation between CD4 T-cell and CD8 T-cell responses was observed in either IMRD group (r=0.70, p<0.001) (figure 2B).
{kind=link}
{kind=link}
Correlation between humoral and cellular responses. (A) CD4 T-cell response prediction as a function of humoral response. (B) CD8 T-cell response as a function of CD4 T-cell response.
Effect of different immunotherapies on the immunogenicity of the vaccine in patients with IMRD
Since decreased vaccine’s immunogenicity was observed in both IMRD cohorts, we next sought to investigate differences that might be due to treatment. Thus, we compared immune responses in patients with IMRD receiving different therapies (table 2).
Humoral and cellular responses to vaccine according to treatment received: comparison between cohort 1 (immunocompromised, IMRD ISP+) and cohort 2 (immunocompetent, IMRD ISP−)
Humoral response
The lowest seroconversion rate was observed in patients receiving abatacept (10% of 10 patients) compared with patients with IMRD ISP− (β=−0.8, 95% IC −1.8 to −0.2, p=0.001) and the rest of patients with IMRD ISP+ (β=−0.33, 95% IC −0.75 to −0.08, p=0.008). Monotherapy with RTX and BMB was associated with lower seroconversion rates than patients with IMRD ISP− (β=−0.18, 95% IC −0.63 to −0.25, p=0.007 and β=−0.4, 95% IC −0.08 to −0.91, p=0.04, respectively) and the rest of patients with IMRD ISP+ (β=−0.31, 95% IC −0.72 to −0.09, p=0.03). In the case of RTX, serum IgG levels in patients vaccinated within 9 months after treatment were below 33.8 BAU/mL in about 75% of patients, but titres increased in correlation with mean time after RTX treatment (r=0.49, p=0.015).
Regarding MTX, we found a reduction in anti-spike antibodies (313±291 vs 458.6±2960, p=0.02), and seroconversion rates (p=0.04) compared with IMRD ISP−, suggesting that MTX modestly impairs humoral response to mRNA-based vaccines. Interestingly, monotherapy with MFM, LFM and AZA did not significantly affect seroconversion rates. However, antibody titres were diminished with AZA (178.5±142, p=0.01), MFM (323±250, p=0.03), but not with IL-6 inhibitors (611.5±272.7, p=0.79) or anti-TNF (543.6±298, p=0.61). Compared with monotherapy with anti-TNFs, significant lower antibody titres were observed when combined MTX plus anti-TNF therapy was used (543.6±298 vs 356±246, p=0.03). Meanwhile, combination of MTX with either BMB or RTX did not worsen the effects of the isolated drugs. Interestingly, higher seroconversion rates in patients under hydroxychloroquine were found when compared with IMRD ISP+ (β=0.22, p=0.01).
Cellular responses
When analysing T-cell responses, we again observed the lowest responses in abatacept-treated patients (10% CD4-responders of 10 patients, p=0.03 and p=0.003 compared with the rest of IMRD ISP+ or IMRD ISP−, respectively). Eighty per cent of 21 patients on monotherapy with MTX, 70% of 10 patients with MFM and 42% of 7 patients with AZA showed a complete cellular response. Quantitative values of CD4 and CD8 immune responses of patients on different treatments are shown in online supplemental material 4. Compared with monotherapy, combined therapies of MTX with either RTX or BMB did not significantly worsen cellular responses to vaccination. Abatacept was associated with lower cellular immunogenicity compared with patients with IMRD ISP− (β=−0.25, IC 95% –0.79 to −0.29, p=0.003) and the rest of patients with IMRD ISP+ (β=−0.33, IC 95% –0.59 to −0.25, p=0.03). However, RTX (β=−0.08, 95% IC −0.47 to 0.3, p=0.08), MTX (β=−0.4, 95% IC –0.9 to 0.13, p=0.56) and BMB (β=−0.33, 95% IC −0.29 to 0.96, p=0.47) were not associated with lower cellular immunogenicity compared with patients with IMRD ISP− but associated when compared with healthy controls. Regarding anti-TNF and IL-6 inhibitor therapies, either in monotherapy or combined with MTX, we found similar T-cell responses than in the rest of patients with IMRD ISP−. Treatment with hydroxychloroquine was associated with higher cellular immunogenicity in comparison with IMRD ISP+ (β=0.21, 95% IC 0.12 to 0.86, p=0.03).
Supplemental material
It must be stressed that CD4 T-cell and CD8 T-cell responses were often present in serological non-responders under any treatment: RTX (50%), BMB (63%), RTX+MTX (50%), BMB+RTX (60%). Across all patients and treatments, CD4 T-cell and CD8 T-cell responses were positively correlated (β=0.73, p<0.001).
Multivariate analysis
To control for possible confounding variables, we performed stepwise multivariate regression analysis adjusting for age, gender, disease duration, treatments and glucocorticoid and MTX cumulative dose (table 3). A negative correlation between IgG anti-spike levels and age >65, disease duration >10 years, abatacept, MTX cumulative dose and glucocorticoid cumulative dose was found. Moreover, a positive correlation with antimalarial treatment was also found. Regarding cellular responses (CD4 and CD8), only a negative correlation with abatacept was maintained.
Multivariant analysis
Discussion
We report the results on the effectiveness of SARS-CoV-2 vaccine focusing on humoral and cellular responses after two doses of BNT162b2 or mRNA-1273 in patients with IMRD, and determine the influence of immunosuppressive and biological therapies in the vaccine’s immunogenicity. It is, to our knowledge, one of the very first studies to analyse immunogenicity to mRNA vaccines in immunosuppressed patients with rheumatic diseases simultaneously assessing serological, CD4 T-cell and CD8 T-cell responses.
We considered two pre-determined hypotheses: that potential decreased vaccine’s immunogenicity might be due to an underlying IMRD-intrinsic dysregulation of the immune response and/or to immunosuppressive/immunomodulatory therapies. Results show that although the entire IMRD population elicited reduced vaccine’s immunogenicity as compared with healthy population, immunosuppressive treatment rather than diagnosis further reduced immunogenicity (online supplemental material 3). Drugs directed to cell surface proteins or that modify T or B-lymphocytes metabolism, but not blockade of effector distal cytokines, exerted deleterious effects, as described with another vaccines.15
Supplemental material
When comparing humoral response, we observed substantial reductions in seroconversion and antibody titres in patients with ISP+ compared with to patients with ISP−. The lowest seroconversion rate was observed in patients receiving abatacept compared with patients with IMRD ISP− and the rest of patients with IMRD ISP+, that was also associated with the lowest T-cell responses. BMB and RTX-treated patients showed reduction in seroconversion and antibody titres after vaccination. Nevertheless, in these patients, T-cell responses were successfully induced in most, suggesting that humoral response is more affected than cellular response, as previously reported in patients treated with B-cell depleting therapies vaccinated with influenza and pneumococcal vaccines.16 17 We observed a positive correlation between mean interval from last RTX dose and immunogenicity and found that most patients vaccinated within 9 months after RTX treatment showed lower seroconversion and antibody levels. These findings are consistent with previous studies regarding the influence of anti-CD20 therapy on humoral response and as predictor of failure to seroconvert.18–21
As already reported with other types of vaccines,15 22 LFM, anti-TNF and IL-6i agents and antimalarials did not significantly affect mRNA vaccine’s humoral and cellular immune responses.
In our study, the effect of MFM on humoral and cellular vaccine’s immunogenicity was milder than the observed with AZA. These data contrast with a study reporting lower serological responses to mRNA SARS-CoV-2 vaccines in recipients of solid organ transplants under immunosuppression (MFM or AZA), and also with another study in patients with rheumatic diseases under MFM. But in both studies, responses were measured after a single dose of vaccine, and cellular responses were not mentioned.23 24
Seroconversion and anti-spike titres were moderately decreased, but T-cell responses mostly preserved, in patients treated with MTX. Consistent with our data, two other studies showed lower levels of spike-specific IgG in patients receiving MTX versus immunocompetent controls and patients receiving biologic agents, but cellular immunity was not hampered.25 26 We did not observe decreased vaccine’s immunogenicity in patients on combined therapy with anti-TNF/IL-6i and MTX.
In multivariate analysis, a negative correlation between humoral response and age >65 years was found, despite no association in univariate analysis. It is well-known that immunosenescence brought on by natural ageing leads to T-cell exhaustion and intrinsic B-cell defects, which alter immunogenicity.27 Furthermore, since functional immunosuppression is related with length of disease and therapies, we also considered the influence of cumulative glucocorticoid and MTX dose. Interestingly, we found that disease duration >10 years, accumulated dose of glucocorticoids and MTX and treatment with abatacept were also independent predictors of dimmed immunogenicity. But it has to bear in mind that collinearity among variables cannot be fully excluded. On the contrary, surprisingly, hydroxychloroquine had a positive effect on immune response to the vaccines.
Our study has several strengths: we have included homogeneous study groups matched by age and gender, patients with different diseases and treatments, and have determined the effects on both humoral and functional cellular (CD4 and CD8) immune responses to this new vaccine strategy. While we still don’t understand the importance of cellular immune responses in COVID-19, it is recognised that in immunosuppressed patients, vaccine-induced cellular immunity is a better surrogate for protection.28–30 Cellular immunity has a crucial role in SARS-CoV-2, as specific CD4 and CD8 responses have been identified in healthy COVID-19-recovered individuals, but also in recovered agammaglobulinemic patients.31 32 Moreover, since our study is prospective, all patients will be followed for 1 year to assess vaccine’s clinical efficacy and duration related to their humoral and cellular immune responses. In addition, the effect of a booster dose will be evaluated.
On the other hand, important limitations of the study also exist. Distinction between immunosuppressive and immunomodulatory drugs is at present far from clear,33 rendering the choice of cohorts difficult. We reasoned that this weakness could be appropriately overcome by using a composite of objective features (online supplemental material 2). The small number of patients treated with some drugs does not allow generalisation of conclusions. It has also to be recognised that even with a multifactorial analysis, the net effect of any single characteristic analysed is difficult to envision.
In light of our findings, it would be advisable to consider cell-mediated responses after vaccination in patients with immune-mediated inflammatory diseases. However, its clinical utility warrants further research with a greater number of vaccinated immunosuppressed patients.
Data availability statement
Data are available in a public, open access repository. Not applicable.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by CAULE's Ethical Committee. Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors CSS, SC, JGRdM contributed to study design and developed the study protocol. CSS, SC, JGH and JGRdM contributed to sample preparation and performed the assays. CSS, CMM and EDA selected and recruited patients. CSS, SC, CMM, EDA, JGH, FR and JGRdM contributed to analysis and clinical interpretation of the data. CSS, FR and JGRdM performed the statistical analysis. CSS, SC, CMM, JGH, EDA, FR and JGRdM contributed to drafting and editing the final manuscript. All authors had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Funding CAULE'S Research funding 2021.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.