Article Text

Abstract
Objective The association between passive smoking exposure in childhood or in adulthood, and the risk of rheumatoid arthritis (RA) has been incompletely investigated. We aimed to assess the relationship between exposure to passive smoking and the risk of incident RA in a French prospective cohort of healthy women.
Methods The E3N Study (Etude Epidémiologique auprès des femmes de la Mutuelle générale de l’Education Nationale) is a French prospective cohort of women included in 1990. Exposures to passive smoking were assessed using self-reported questionnaires. RA cases were self-reported and subsequently validated. Cox proportional hazards regression models adjusted for age and for potential confounders were used to estimate HRs and 95% CIs for incident RA.
Results Among 79 806 women, 698 incident cases of RA were identified; 10 810 (13.5%) women were exposed to passive smoking in childhood, and 42 807 (53.6%) in adulthood. Median age at inclusion was 47.8 years. Passive smoking in childhood and in adulthood was associated with RA risk in all models (HRs (95% CIs) 1.24 (1.01 to 1.51) and 1.19 (1.02 to 1.40), respectively). The absolute risk of RA among never smokers with exposure to passive smoking in childhood and/or adulthood (47.6/100 000 person-years) was close to the risk of ever smokers with no passive smoking exposure (47.2/100 000 person-years), while it was highest in ever smokers also exposed to passive smoking (53.7/100 000 person-years).
Conclusion Exposure to passive smoking in childhood and/or adulthood increases the risk of RA by the same order than active smoking. Such exposure should be suppressed, especially in individuals at risk of RA.
- rheumatoid arthritis
- smoking
- autoimmunity
- epidemiology
- autoantibodies
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
To date, only a few studies assessed the association between passive smoking and the risk of rheumatoid arthritis (RA), and results are conflicting.
What does this study add?
In this prospective cohort of almost 80 000 women, passive smoking exposure during childhood and/or adulthood was associated with an increased risk of RA, especially in never smokers. Passive smoking in childhood is particularly associated with the risk of RA, which may occur earlier than in women never exposed to smoking.
How might this impact on clinical practice or further developments?
Our results support the hypothesis that passive smoking is associated with the risk of RA. Exposure to passive smoking, especially during childhood, should be limited as much as possible, especially in individuals at high risk of RA.
Introduction
Rheumatoid arthritis (RA) is an inflammatory rheumatic disease of complex pathogenesis. Genetic and environmental factors are thought to interact to trigger autoimmunity leading to the disease.1 Personal active smoking has been the most reproducibly reported risk factor for RA, particularly in patients carrying the HLA-DRB1-shared epitope (SE) alleles.2–5
While secondhand smoking could increase disease activity in women with RA,6 only a few studies assessed the association between passive smoking (PS) and the risk of RA, and results are conflicting. In adulthood, PS exposure at work or at home was not associated with RA in two case–control studies and one cohort study.7–9 In a previous work in the E3N cohort of French women, we identified for the first time that, compared with never smokers not exposed to PS in childhood, ever-smoking women exposed to PS in childhood had an increased risk of RA.10 In this preliminary work, we could not identify PS as a risk factor independent of active smoking, possibly because of underpowered analysis. Indeed, at the time of the study, only part of RA cases were identified, that is, only 371 incident RA cases.10
Thus, now that more RA cases have been identified,11 the objectives of this prospective study were to investigate the relationship between PS in childhood and/or adulthood, and the risk of incident RA in a large prospective cohort of healthy French women.
Material and methods
Study population
The French E3N Study (Etude Epidémiologique auprès des femmes de la Mutuelle générale de l’Education Nationale) is a prospective cohort, initially conceived to study environmental risk factors for cancers and chronic diseases. It includes 98 995 healthy French women, primarily teachers, since 1990 covered by a national health insurance. Follow-up is still ongoing.12 They were sent every 2–3 years questionnaires (Q1–Q12) with questions on their health, lifestyle and newly diagnosed diseases. The average response rate per questionnaire is 83%, and less than 3% of the participants were lost to follow-up since 1990. Signed consent was obtained from all participants.
RA ascertainment
Identification of RA cases has been previously described.11 Briefly, participants who self-reported having RA in the follow-up questionnaires were sent a validation questionnaire adapted from Guillemin et al13 in 2017. Women were considered as cases if they confirmed having RA in this validation questionnaire and if any of the following criteria were fulfilled: (1) RA was confirmed by a physician, (2) they self-reported taking any disease-modifying antirheumatic drugs (DMARDs) considered specific of RA, (3) they self-reported having positive auto-antibodies (rheumatoid factors and/or anti-citrullinated protein antibodies), (4) at least four of the seven 1987-American College of Rheumatology (ACR) criteria were met. Sensitivity and specificity of this algorithm were 93.8% and 82.6%, respectively. For women who did not answer the specific validation questionnaire, we used the medication reimbursement database and women were considered as cases if they had had reimbursements of any DMARDs considered to be specific of RA. Sensitivity and specificity of this method were 70.5% and 87.3%, respectively.
For the present study, only incident cases, diagnosed after 1990, were considered and we excluded women who did not complete any of the three questionnaires (Q9, Q10 and Q11) collecting self-reported diagnosis of RA, prevalent RA cases occurring before baseline and RA cases with unavailable date of diagnosis.
Variables of interest
At inclusion, women had to answer the following question: ‘When you were a child, did you stay in a smoky room?’. Answer modalities were ‘never’, ‘do not remember’, ‘rarely’, ‘occasionally (a few hours a week)’, ‘a few hours a day’ or ‘several hours a day’. Women were considered exposed to PS in childhood if the answers were ‘a few hours a day’ or ‘several hours a day’.
PS exposure in adulthood was assessed at inclusion by asking the women to sum their time spent at home or outside the home during the day in a room while someone was smoking. This time was expressed in hours: ‘0’, ‘<1 hour’ or the number of hours. They were considered exposed if they were exposed at least 1 hour a day.
Education (<high school; up to two-level university; three/four-level university) was self-reported and collected in the first questionnaire. Weight and height were also self-reported in the first questionnaire and used to calculate body mass index (BMI; <18.5 kg/m², 18.5–25 kg/m², 25–30 kg/m², ≥30 kg/m²). Weight has been additionally measured in approximatively 10 000 women who provided a blood sample at a collection centre, and correlation between self-report and measured BMI was excellent. Personal smoking status (non-smoker, former smoker and current smoker) at inclusion was also available.
Statistical analyses
Follow-up began on the date the first questionnaire was returned in 1990 (baseline), and women contributed person-time until the date of RA diagnosis, the last completed questionnaire until the 2017 questionnaire (Q11), death or loss to follow-up, whichever occurred first.
In descriptive analyses, results were expressed as count (%) for categorical variables and median (IQR) for continuous variables.
To estimate the risk of RA associated with PS (HR and their 95% CIs), we used Cox multivariable regression models with age as the timescale (model 1), and adjusted on baseline smoking status (never, current or former smoker), the other types of PS, educational level (<high school, up to two-level university, three/four-level university) and baseline BMI (<18.5 kg/m², 18.5–25 kg/m², 25–30 kg/m², ≥30 kg/m²) (model 2). Analyses were stratified on smoking status (ever or never smokers). Potential interactions between active smoking status and PS were investigated. In addition, we built up a model that considered both exposure to PS in childhood and/or adulthood and personal smoking (ever and never smokers). This model was used to calculate absolute risks of RA associated with combinations of smoking status and PS in childhood and/or adulthood.
We also performed a sensitivity analysis on seropositive incident RA cases only, by excluding seronegative cases, or with unknown seropositivity status. Models 1 and 2 were fitted on this population.
Finally, we compared mean ages at RA onset according to PS exposure in childhood and/or in adulthood and according to personal smoking (ever or never smokers) with analyses of variance.
All statistical analyses were carried out using SAS software, V.9.3 (SAS Institute). All p values were two tailed and considered significant if p<0.05.
Patient and public involvement
Patients and the public were not directly involved in the design or completion of this study.
Results
Characteristics of the study population
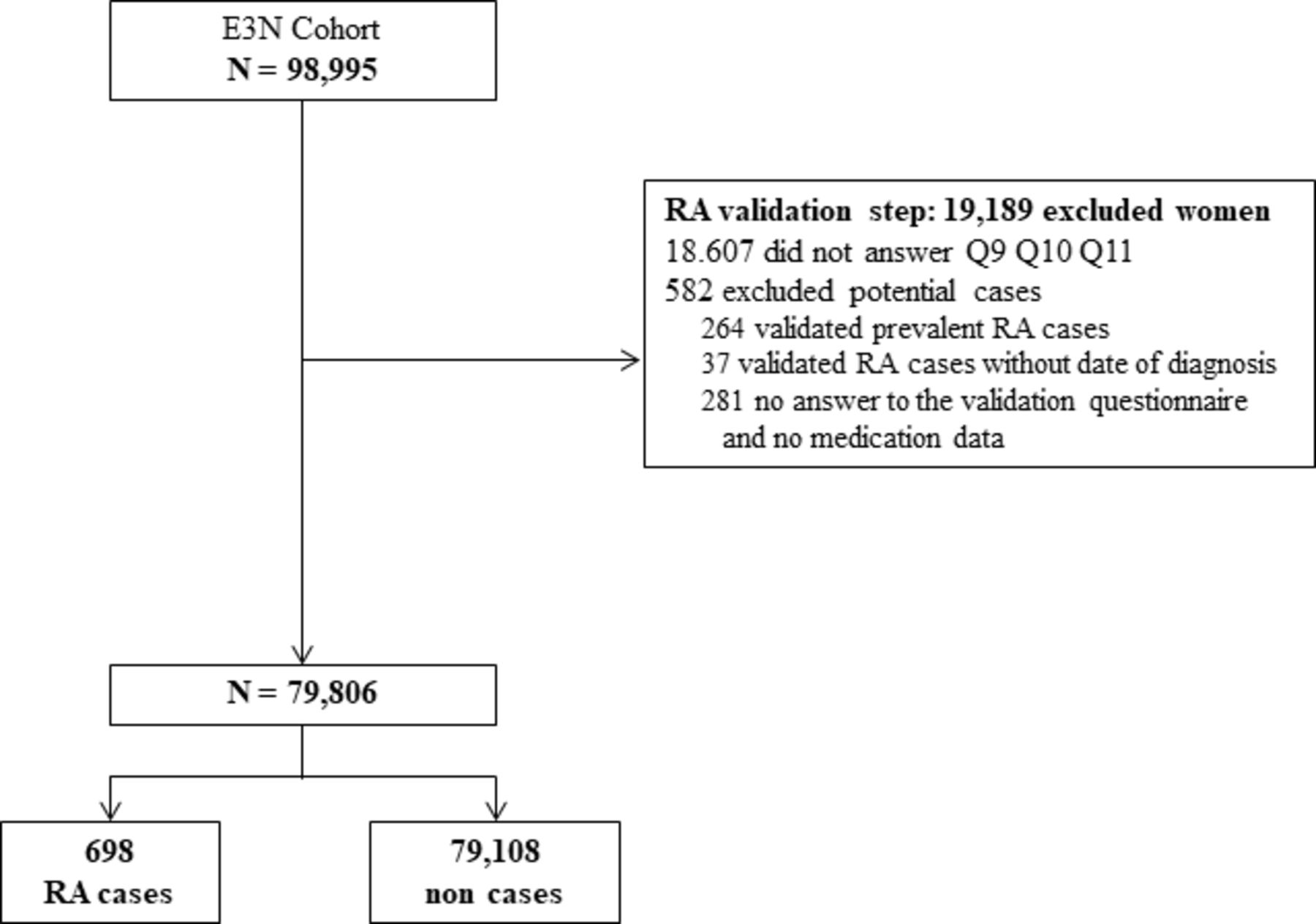
Among the 98 995 women of the cohort, the study population included 79 806 women during a total of 1 897 583 person-years of follow-up, including 698 incident RA cases (figure 1). Median (IQR) follow-up was 24.47 (24.33–24.54) years, and median age at cohort entry was 47.9 (43.5–53.5) years. Incident RA cases were diagnosed after a median of 14.9 (8.6–19.2) years after baseline and median age at RA diagnosis was 63.4 (57.7–70.3) years. Antibody status was known for 230 (33.0%) incident cases and 210 (91%) of them were seropositive.

Flow chart of the study among women in the E3N cohort. E3N, Etude Epidémiologique auprès des femmes de la Mutuelle générale de l’Education Nationale; RA, rheumatoid arthritis.
Characteristics of the overall study population according to PS in childhood and in adulthood are presented in table 1. In the whole study population, 10 810 (13.5%) women were exposed to PS in childhood, 42 807 (53.6%) to PS in adulthood, 6581 (8.25%) were exposed to both and 47 036 (58.9%) were exposed to either. Regarding active smoking, 36 636 (45.91%) had ever smoked (14.19% current and 31.71% former smokers). Compared with never smokers, current, former and ever smokers had similar increased risk of RA: HRs (95% CIs) 1.30 (1.04 to 1.63); 1.21 (1.13 to 1.42); 1.23 (1.06 to 1.43), respectively.
Baseline characteristics of the study population of the E3N cohort (N=79 806)
PS in childhood and risk of RA
In the whole population, PS in childhood was positively associated with the risk of RA in all models, including adjustment on PS in adulthood (HR 1.24; 95% CI 1.01 to 1.51 in model 2) (table 2). When stratifying on active smoking status, PS in childhood was associated with RA only in never-smoking women (HR 1.40; 95% CI 1.06 to 1.86). However, the interaction term was not statistically significant (p=0.28). In the whole population, compared with never smokers with no passive smoking in childhood, RA risk of never smokers exposed to PS in childhood was increased (HR 1.38; 95% CI 1.04 to 1.83), and of the same magnitude as the risk of ever smokers with exposure to PS in childhood (HR 1.37; 95% CI 1.03 to 1.82).
HRs (95% CIs) for incident rheumatoid arthritis according to passive smoking in childhood, overall and after stratified by ever-smoking status among women in the E3N cohort (N=79 806)
When restricting our analyses to the 210 seropositive incident cases, PS in childhood was still associated with the risk of seropositive RA (HR 1.55; 95% CI 1.10 to 2.18 in model 2), especially in never smokers (HR 1.67; 95% CI 1.03 to 2.71 in model 2), but not in ever smokers (table 3).
HRs (95% CIs) for incident seropositive rheumatoid arthritis (RA) according to passive smoking in childhood, overall and after stratified by ever-smoking status among women in the E3N cohort (N=79 318)
PS in adulthood and risk of RA
PS in adulthood was also associated with the risk of RA in all models, including adjustment on PS in childhood (HR 1.19; 95% CI 1.02 to 1.40 in model 2) (table 4).
HRs (95% CIs) for incident rheumatoid arthritis according to passive smoking in adulthood, overall and after stratified by ever-smoking status among women in the E3N cohort (N=79 806)
There was also no interaction between PS in adulthood and smoking. In analyses stratified on active smoking status, PS in adulthood was associated with an increased RA risk only in never-smoking women (HR 1.27; 95% CI 1.02 to 1.57). In the whole population, in model 2, compared with never smokers with no PS in adulthood, RA risk of never smokers exposed to PS in adulthood was increased (HR 1.24; 95% CI 1.00 to 1.53) and was of the same magnitude as the risk of ever smokers without exposure to PS in adulthood (HR 1.26; 95% CI 1.00 to 1.59). The risk of RA was the highest if women were both ever smokers and exposed to PS in adulthood (HR 1.46; 95% CI 1.20 to 1.79).
In the sensitivity analyses, the association between PS in adulthood and incident seropositive RA was no longer found (online supplemental table 1).
Supplemental material
PS in childhood and/or adulthood and risk of RA
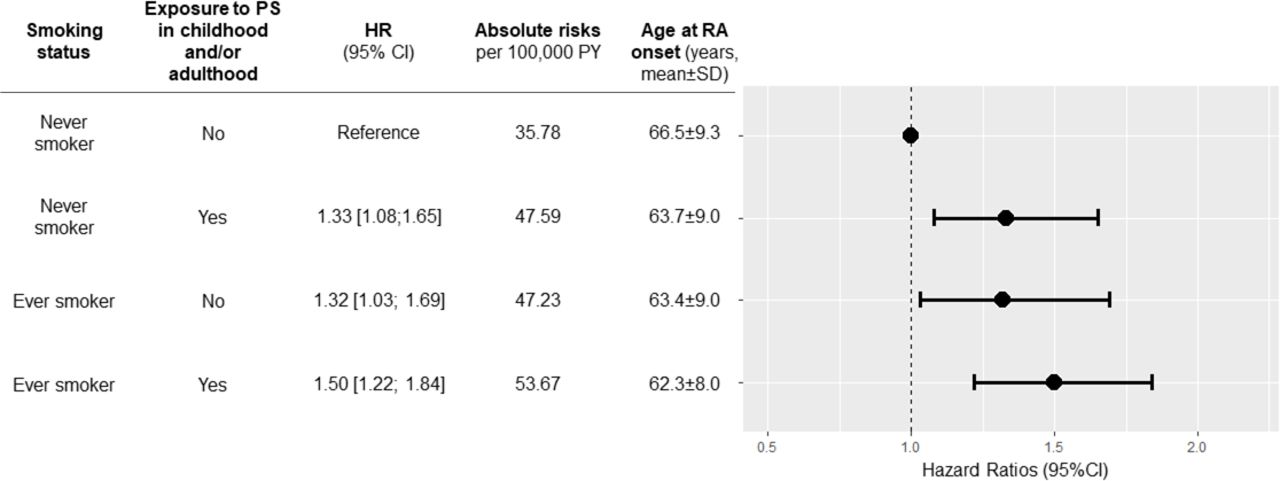
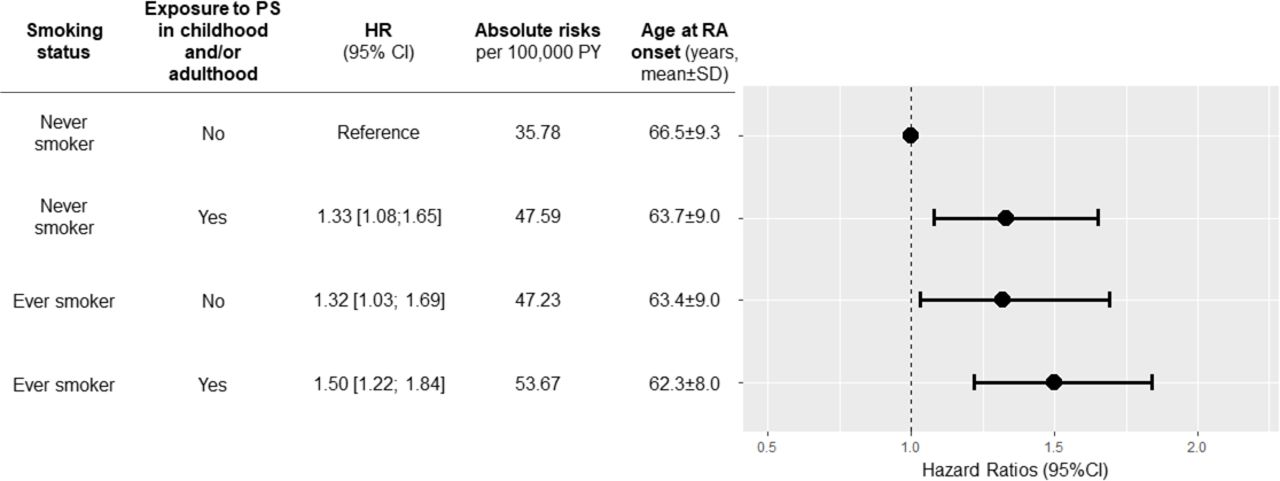
In the whole population, compared with women never exposed to smoking—actively or passively (childhood and/or adulthood)—, women exposed to PS (in childhood and/or adulthood), whatever the active smoking status, were at increased risk of RA (figure 2). The absolute risk of RA was lowest in those never exposed to smoking—actively or passively—(35.8/100 000 person-years), while it was highest in ever smokers also exposed to PS (53.7/100 000 person-years). The absolute risk of RA in never-smoking women exposed to PS (47.6/100 000 person-years) was very close to the risk of ever smokers not exposed to PS (47.2/100 000 person-years).
{kind=link}
{kind=link}
Risk of incident RA and age at RA onset according to smoking status and exposure to passive smoking (PS) during childhood and/or during adulthood among women in the E3N cohort. Results are expressed as HRs with bars representing 95% CIs. This model was adjusted on age (as the timescale), body mass index and educational level, and used to calculate absolute risks of RA associated with smoking status and exposure to PS in childhood and/or in adulthood. This model was used to calculate absolute risks of RA associated with combinations of active smoking status and PS in childhood and/or adulthood. E3N, Etude Epidémiologique auprès des femmes de la Mutuelle générale de l’Education Nationale; PY: person-years; RA, rheumatoid arthritis.
PS and age at RA onset
Age at RA onset was highest among women never exposed to smoking—actively or passively (childhood and/or adulthood) (66.55±9.30 years), while it was lowest among ever-smoking women exposed to PS in childhood whatever PS exposure in adulthood exposure (60.7±9.19 years if also exposed during adulthood, and 60.3±8.83 if not) (table 5). Age at RA onset was in between, and similar among never smokers exposed to PS and ever smokers not exposed to PS.
Age at RA onset according to smoking status among women in the E3N cohort (N=79 806)
Discussion
In this large, population-based prospective cohort study of French women, we reported that PS exposure during childhood and/or adulthood was associated with an increased risk of RA, especially in never-active smokers. This risk was similar to the one of ever-active smokers without exposure to PS especially during adulthood. Interestingly, the size effects related to PS exposure in childhood and in adulthood (HRs 1.26 and 1.24, respectively) were similar to the one of patients who smoked between 1 and 10 pack-years according to a meta-analysis (HR 1.26; 95% CI 1.14 to 1.39 compared with never smokers).14
In addition, we found an even stronger association between PS in childhood and seropositive RA, especially among never smokers, and that RA exposed to PS in childhood was diagnosed earlier than RA never exposed to smoking. Among ever smokers, we failed to find any association between PS exposure in childhood or in adulthood with the risk of RA. Untangling the proper effect of secondhand smoke from primary smoke exposure would require larger populations with different levels of primary smoke exposure.
Our findings reinforce existing hypotheses and understanding of RA pathogenesis, and add to the mucosal paradigm of RA pathogenesis. It is well established that smoking favours citrullination and, in genetically predisposed people, immunisation to citrulline can occur years before the first symptoms of the disease.3 5 The fact that exposure to smoking at the very beginning of life could be associated with RA suggests that autoimmunity could be triggered even earlier and many years before the onset of the symptoms.
Previous attempts have been made to assess the association between PS exposure and RA. In the Nurses’ Health Study I prospective cohort, there was no association between PS exposure although PS exposure was assessed by the number of years lived with a smoker.7 However, long exposure to PS (≥30 years of exposure) was marginally associated with incident RA both in ever and never smokers, suggesting a potential link. More recently, the association of life course PS and the risk of incident RA has been reported in the Nurses’ Health Study II cohort.15 Childhood exposure measured by childhood parental smoking was associated with a 41% increased risk of seropositive RA after adjustment for potential confounders, and a 75% increased risk after further adjustment for adulthood active and passive smoking. The association was even stronger among ever smokers, while there was no association in never smokers. These results are consistent with ours, even though, we mainly observed an increased RA risk associated with PS exposure in childhood in never smokers. In a Swedish population-based case–control study including 589 cases and 1769 controls, there was no association between exposure to PS (at home or at work) and the risk of RA.8 However, the authors did not separately consider PS exposure in childhood and in adulthood, and the retrospective design of the study might be prone to differential recall bias.
We acknowledge some limitations to our study. First, our cohort only studied women. However, incidence of RA being higher in women, our study population was appropriate to test our hypothesis. In addition, identification of RA cases was based on self-reported data. However, the accuracy of our case identification was improved by our algorithms. Antibody status was known in only 230 (33%) RA cases, and 210 of them (91%) were seropositive, which further validates our algorithm for the diagnosis of RA. The low rate of antibody status is due to the self-reported design of the questionnaire, and the difficulties for patients to report their serological status. However, even with a reduced power, we still found an even stronger association between PS in childhood and seropositive RA, reinforcing our hypothesis. We acknowledge that exposure to PS was assessed only at a single time at baseline and we did not have quantitative data on cumulative personal active smoking and pack-years. In addition, exposure to PS in childhood was retrospectively collected, which might be prone to recall bias. However, because this question was asked years before the onset of RA, this bias should not be differential. Although we adjusted our analyses on several potential confounders, we did not adjust for other factors such as diet, lifestyle or air pollution, as data were either not available or available only in a fraction of the cohort. However, our study was mostly focused on investigating associations with childhood PS, which was unlikely to be strongly confounded by adult dietary or lifestyle behaviours. However, this could have potentially had an impact on our assessment of associations with adult PS. We were not able to investigate a potential gene–environment interaction, lacking data on the HLA-DRB1-SE and on family history. Finally, we could not perform analyses on RA severity, including radiological changes and clinical severity, and because we excluded prevalent cases occurring before baseline, our results might not apply to early life RA occurring before the inclusion, leading to a higher median age of RA onset.
Nevertheless, the strengths of our study include the large cohort size and the high number of RA, during a long follow-up period. In addition, we stratified our analyses on personal smoking exposure and were able to study the effect of PS on never-smoking women.
To conclude, PS during childhood and/or adulthood was associated with an increased risk of RA, especially among never-smoking women. Such exposure should be limited as much as possible to prevent the onset of the disease. Even if our study was not designed to investigate this point, this message could especially apply to individuals at risk of RA, for example, relatives 0f patients with RA.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and approval was obtained from the French National Commission for Data Protection and Individual Freedom (327346-V14) and the French Advisory Committee on Information Processing in Material Research in the Field of Health (13.794). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors acknowledge all participants of the E3N Study for their continued participation. The authors would like to thank Pascale Gerbouin-Rerolle and Roselyn Rima Gomes for their help on data management.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
M-CB-R and RS contributed equally.
Contributors All authors contributed to the manuscript. YN, CS, XM, M-CB-R and RS were responsible for conception and design. YN, M-CB-R and RS were responsible for data collection and analysis. All authors were responsible for the interpretation of data. YN wrote the first version of the manuscript. All authors critically revised and approved the final version of the manuscript. All authors agreed to be accountable for all aspects of the work and attest to the accuracy and integrity of the work.
Funding The present work was performed using data from the Inserm E3N cohort and support from the MGEN, Gustave Roussy and the Ligue contre le Cancer for setting up and maintaining the cohort. The cohort was supported by a state grant ANR-10-COHO-0006 from the Agence Nationale de la Recherche within the Investissement d’Avenir programme. This study was conducted thanks to a research grant from FOREUM Foundation for Research in Rheumatology. In addition, the validation study was conducted with the financial support from the Société Française de Rhumatologie.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.