Article Text

Abstract
Objectives The European Alliance of Associations for Rheumatology (EULAR) recommendations for the use of imaging in large vessel vasculitis establish that an imaging test supported by clinical pretest probability (PTP) is sufficient for the diagnosis of giant cell arteritis (GCA). Our objective was to determine the validity of the EULAR recommendations on the use of Colour duplex ultrasound (CDUS) in GCA after calculating the PTP.
Methods We collected data of all patients referred to our fast-track clinic between 2016 and 2020. The Southend pretest probability score (SPTPS) was calculated and classified as low (LR), intermediate and high risk (HR) according to the values obtained by its authors, <9, 9–12 and >12, respectively. All patients underwent a CDUS of the temporal arteries with their common, parietal and frontal branches, and the most also axillary (86.5%), and subclavian and carotid arteries. The gold-standard diagnosis was made according to the physician’s criteria after at least 9 months of follow-up.
Results Of the 297 referred patients, 97 (32.7%) were diagnosed with GCA. The SPTPS area under the ROC curve was 0.787. The LR category included 105 patients (35.4%), of which 10 (9.5%) had GCA and 1 had a CDUS false negative result. The HR category included 67 patients (22.5%), 47 with GCA, and in 1 case the CDUS result was a false positive.
Conclusion Combining the results of a PTP score, such as SPTPS, and the CDUS allows for an accurate diagnosis of GCA, as established by the EULAR group, with less than 2% misclassification of diagnosis.
- Giant Cell Arteritis
- Ultrasonography
- Systemic vasculitis
- Autoimmune Diseases
Data availability statement
All data relevant to the study are included in the article. No additional data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
In the 2018 European Alliance of Associations for Rheumatology (EULAR) recommendations on the use of imaging in large-vessel vasculitis (LVV) in clinical practice, an early imaging test was recommended for the diagnosis of giant cell arteritis (GCA), while ultrasounds for all patients with suspected GCA was recognised as cost-effective. Determining the pretest clinical probability was recommended in order to support the imaging result and to decide whether additional diagnostic tests are necessary.
What does this study add?
The EULAR recommendations on the use of imaging in LVV are supported by a consensus of experts informed by a systematic review of the evidence, although its results in actual clinical practice have not confirmed. In other way, there is not a definition about what is low or high clinical risk.
Our results show how the use of a clinical pretest probability score, together with an ultrasound test, correctly classifies 98% of GCA patients with a positive or negative imaging test, in accordance with the second EULAR recommendation.
How might this impact on clinical practice or further developments?
The confirmation in clinical practice of the 2018 EULAR recommendations for the use of imaging in the diagnosis of LVV should provide assurance about the usefulness of their clinical use and encourage the introduction of imaging in future classification criteria of the disease.
Introduction
Giant cell arteritis (GCA) is a chronic vasculitis of the medium and large arteries. Temporal artery biopsy (TAB) has long been regarded as the gold standard for diagnosing GCA.1 However, the evidence that has emerged from systematic literature reviews shows that Colour duplex ultrasound (CDUS) has a higher sensitivity than TAB for the diagnosis of GCA.2 Furthermore, CDUS is patient-friendly, more cost-effective and allows a much faster diagnosis than TAB. Therefore, in the European Alliance of Associations for Rheumatology (EULAR) recommendations for the use of imaging in large vessel vasculitis in clinical practice, the taskforce recommends an early imaging test in patients with suspected GCA, and CDUS of the temporal ±axillary arteries (AAs) as the first imaging modality to be performed in these patients.3 As a second recommendation, the authors state that in patients in whom there is a high clinical suspicion of GCA and a positive imaging test, a diagnosis of GCA can be made without an additional test (TAB or another imaging), while in those with low clinical probability and a negative imaging result, a diagnosis of GCA is unlikely. In all other situations, additional efforts towards establishing a diagnosis are necessary.3
The problem arises in how to establish what constitutes low or high clinical suspicion. Most clinicians will likely form a subjective opinion that can sometimes be very clear, but in other cases be only doubtful. A tool that enables one to determine what the pre-test clinical probability (PTP) is, and thus improve the precision of the imaging test is much needed. In this context, one recently published tool is the Southend pre-test probability score (SPTPS), a probability-based algorithm that aids in the diagnosis of suspected GCA in a fast-track clinic, one which includes low risk (LR), intermediate risk (IR) and high risk (HR) classifications.4 5
The main objective of our study was to determine the validity of the EULAR recommendations for the use of CDUS in GCA after calculating the PTP based on the SPTPS of our patients.
Methods
Suspected GCA patients who had been consecutively referred to our fast track clinic between 1 January 2016 and 31 December 2020 were included. Medical history data records were retrospectively reviewed and collected. Those who lacked the necessary clinical data to calculate the SPTPS were excluded. The clinical and laboratory features of all patients at referral were evaluated, and the SPTPS items were applied.4 The PTP based on SPTPS was categorised as LR if the value was less than 9, IR if it was between 9 and 12 and HR if it was greater than 12, following the values established by its original authors.5 At the time of referral, all patients underwent a CDUS exploration of the superficial temporal arteries (TAs) including their common trunks, parietal and frontal branches and, in most cases, large-vessel examination of their AAs (86.5%), subclavian (52.5%) and carotid arteries (47.1%). The gold-standard for diagnosis of GCA was the physician’s final diagnosis at a follow-up of 9 months based on the patients’ clinical presentation and evolution, the results of CDUS -and other imaging techniques or TAB—as well as treatment response. The patients diagnosed with GCA were classified into the following categories according to their pattern of involvement evaluated by imaging tests (CDUS, and only those considered necessary by their attending physician, positron emission tomography-computed tomography (PET-CT)): cranial if the TAs were exclusively affected; extracranial if only the large vessel arteries were involved without associated involvement of the TAs; and mixed if both TAs and large vessels were affected.
Imaging
A CDUS diagnosis of GCA was made if the halo sign appeared in at least one vessel segment. In agreement with the Outcome Measures in Rheumatology (OMERACT) guidelines, we defined the halo sign as homogenous, hypoechoic wall thickening, well-delineated towards the luminal side, visible in both the longitudinal and transverse planes, most commonly concentric in the transverse scans.6 To increase the accuracy of the diagnosis, we measured the intima media thickness on a grey scale using a cut-off of 0.34 mm for the frontal and parietal branches of the TAs, 0.42 mm for common trunk of the TAs and 1 mm for the AAs, in agreement with previous studies.7–9 The CDUS examinations were performed by two highly experienced sonographers (EDM and IM), with 6 and more than 15 years of experience, respectively. For the CDUS examinations carried out from 2016 to 2019, a MylabTwice (Esaote, Genua, Italy) equipment was used with the following settings: for the exploration of the TAs, a 10-22MHz probe was used, with a set frequency of 22 MHz for grey scale and 12.5 MHz for colour Doppler, a colour gain adjusted to fill only the lumen and a pulse repetition frequency (PRF) of 2 kHz; and for AAs, subclavian and carotid arteries, a 4–13 MHz probe was used, with a set frequency of 13 MHz for grey scale and 7.2 MHz for colour Doppler with a PRF of 3.5 kHz and adjusted colour gain. For the CDUS examinations performed in 2020, a MyLab X8 eXP (Esaote, Genua, Italy) was used with the following settings: for TA, a 12–25 MHz probe, with a set frequency of 24 MHz in grey scale and a Doppler frequency of 12.5 MHz, an adjusted colour gain and a PRF of 1.9 kHz; and for AA, subclavian and carotid arteries, the probe used was 4-15MHz, with a grey frequency of 15 MHz and a Doppler frequency of 4.5 MHz, an adjusted colour gain and a PRF of 3.0 kHz.
Other diagnostic tests were performed when deemed necessary by the responsible physician.
Data analysis
The absolute and relative frequencies were calculated for the qualitative variables and the medians and IQR for the quantitative ones. Receiver operating characteristic (ROC) curve and the accuracy of the SPTPS were also calculated. For the comparison of quantitative variables between groups, the Mann Whitney U test was used. For the comparison of qualitative variables, the χ2 test was performed if the sample was homogeneous, and the Fisher or Kruskal-Wallis tests otherwise.
SPSS V.23 was used. A p<0.05 was considered statistically significant.
Patient and public involvement
Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research.
Results
Demographic and clinical features
A total of 297 patients referred to our fast-track clinic were included. Of these, 97 (32.7%) were diagnosed with GCA; 205 (69%) were female and 92 (31%) were male. The mean±SD age at referral was 75.4±9.6 years. Table 1 shows the SPTPS clinical and demographic characteristics of the patients included.
Demographic, clinical and laboratory characteristics included in the SPTPS of the patients in our cohort
Values of SPTPS and clinical risk classification
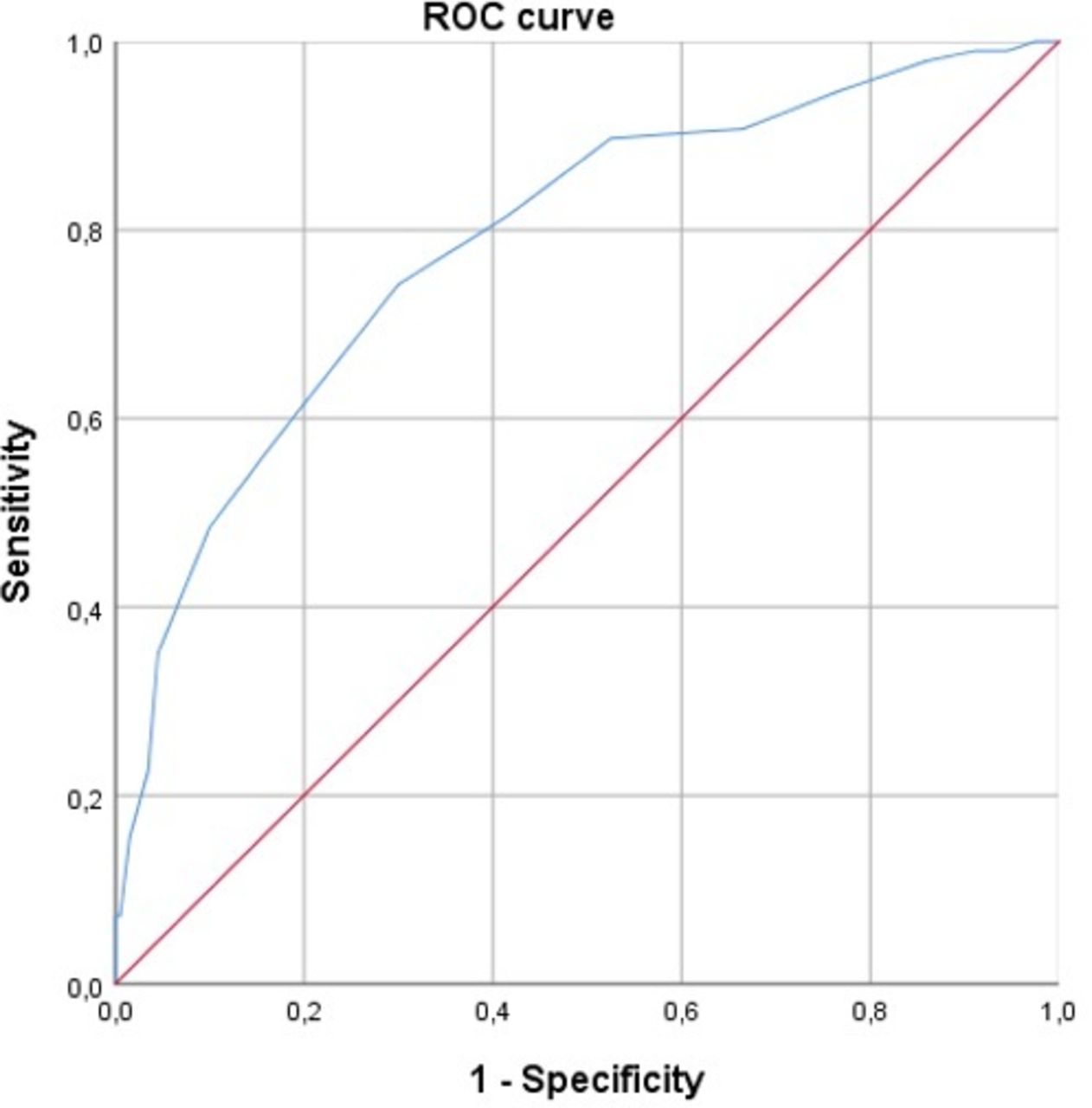
The mean value of the SPTPS was 9.9±3.7, and the area under the ROC curve was 0.787 (95% CI 0.731–0.843) (figure 1). The mean SPTPS of the group with GCA was 12.4±3.6, compared with 8.7±3.1 in the group without GCA (p<0.01).

Receiver operating characteristic (ROC) curve of the SPTPS in our cohort. SPTPS, Southend Pre-Test Probability Score.
The LR category included 105 patients (35.4%), of which 10 had GCA (9.5%) while 95 did not have GCA (90.5%). The IR category included a total of 125 patients (42.1%), 40 with GCA (32%) and 85 without (68%). Finally, the HR category included 67 patients (22.5%), 47 with GCA (70.2%) and 20 without (29.8%).
A value of SPTPS ≥9 (that is, IR or HR), showed a sensitivity of 89.7%, a specificity of 47.5% and a negative predictive value (NPV) of 90.5% in the diagnosis of GCA, while the cut-off point ≥14 (corresponding to the 90th percentile) had a specificity of 95.5% and a positive predictive value (PPV) of 79%.
Ultrasound results
Ninety-seven of the 297 cases registered in our fast-track clinic had a final diagnosis of GCA established by the physician. CDUS examination showed a sensitivity for its diagnosis of 95.9%, with a specificity of 97%, a PPV of 93.9% and an NPV of 97.9%. In 4 of the 97 patients with GCA, the CDUS was negative and the diagnosis was confirmed with PET-CT (3 of them had exclusively aortic involvement and one exclusive involvement of the vertebral arteries). On the other hand, 6 of the 200 included patients without GCA (3%) had a false positive result of CDUS. Table 2 shows the final clinical diagnosis of the false positive and false negative CDUS ‘halo sign’ results. With all but one false positive, the SPTPS classified the patient as LR or IR. In contrast, two patients with GCA and negative CDUS were classified as HR, one as IR and the other as LR.
Final diagnoses of false positives and negatives of CDUS and SPTPS values
The AAs were explored in 257 patients (86.5%), while they were not evaluated, and neither did other large-vessel arteries, in 40 of them (13.5%). Subclavian arteries were explored in 156 patients (52.5%) and carotid arteries in 143 (47.1%). The distribution of the GCA subtypes was: 51 cases of cranial GCA with a mean SPTPS value of 12.7±3.6 points, 28 mixed forms (cranial and extracranial involvement) with a mean of 12±3.1 points and 18 extracranial isolated patterns with a mean of 11.9±4.1 points (all with p>0.05). Of note, in 10 GCA patients presenting with a SPTPS <9, 3 revealed exclusive extracranial involvement (which is equivalent to 20% of all cases with this subtype of the disease), and all had a very low SPTPS of less than 7. Of the 46 patients who had large-vessel involvement (alone or in combination with TAs), 31 had involvement of the AAs (67.4%), 24 of the subclavian arteries (52.2%) and 14 of the carotid arteries (30.4%).
Regarding the other diagnostic tests, TAB was performed in 34 patients (11.4%), PET-CT in 48 (16.2%) and other imaging tests such as AngioMRI or AngioCT in 8 (2.7%). TAB influenced the final diagnosis of 4 CDUS false positives, being especially important in the case of multiple myeloma since histology confirmed the presence of amyloid material in the vascular wall. PET-CT influenced the diagnosis of the 4 CDUS false negatives by allowing the detection of aortic or vertebral vasculitic involvement, as well as in the false positive with final diagnosis of hydrocephalus, since the CDUS showed involvement of large vessels that in the PET-CT was ruled out. The rest of the additional tests did not modify the final diagnosis.
CDUS + SPTPS results
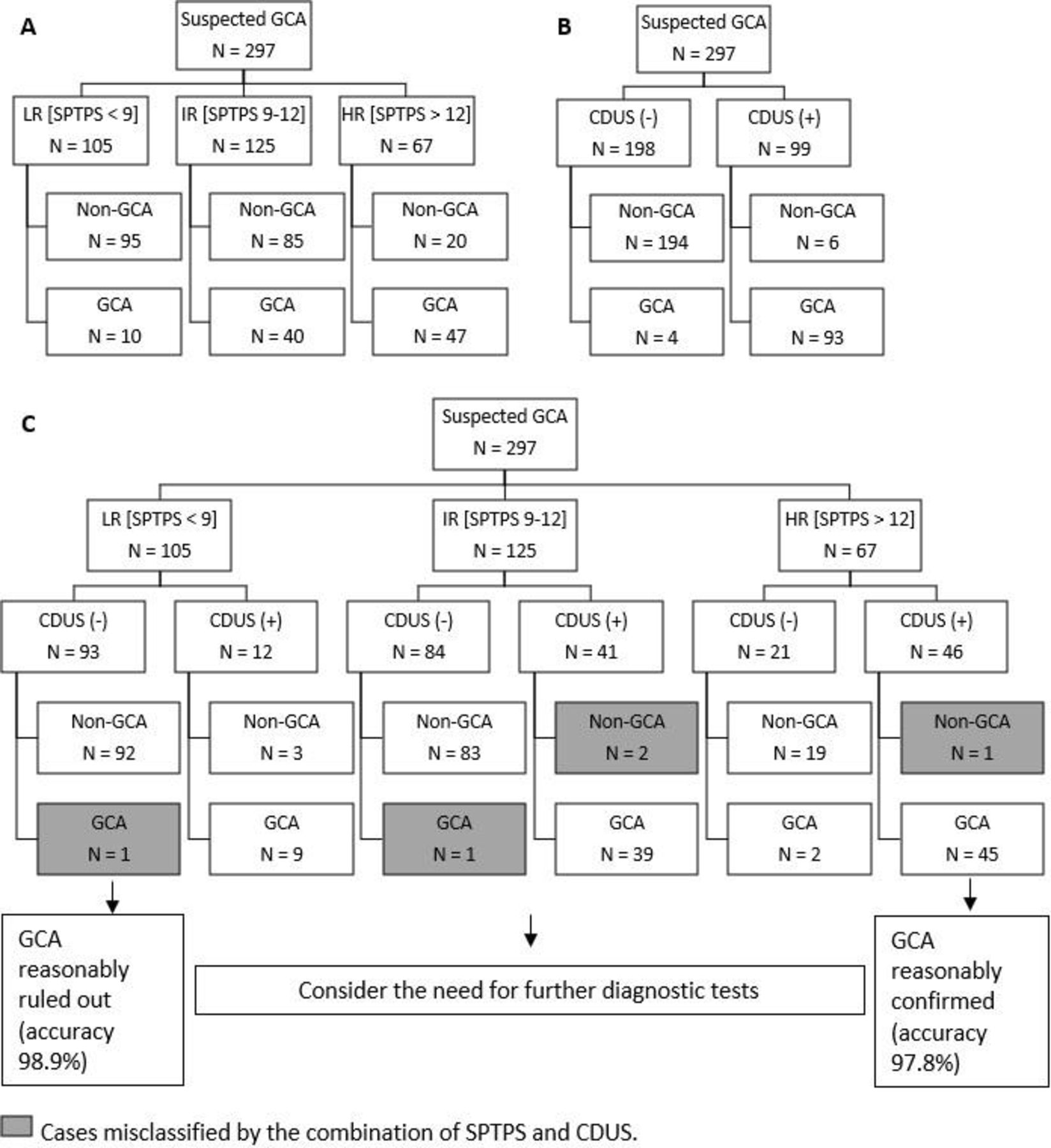
The LR with negative CDUS category had 93 patients, of which one had a final clinical diagnosis of GCA, which represented an error of 1/93 (1.1%). On the other hand, the category of HR with positive CDUS included 46 patients, and one of them had a true positive halo sign but a false positive diagnosis of GCA, because he had amyloidosis with amyloid material in the TAB without any signs of inflammation in the vessel wall, which means an error of 1/46 (2.2%). Within the IR group, we observed that negative CDUS has a high validity to rule out the diagnosis of GCA, since in this category 84 patients had negative CDUS with only one final GCA diagnosis (1.2%). Of the cases with IR and positive CDUS, 2 were not GCA.
A positive CDUS result with LR on SPTPS should lead the clinician to consider that it might not be a GCA, and likewise, a negative CDUS result with HR on SPTPS suggests that it may be a false negative for CDUS. Therefore, the combined use of SPTPS +CDUS only misclassified 5/297 cases (<2%).
Table 3 summarises the diagnostic validity of SPTPS, CDUS and SPTPS+CDUS and figure 2 shows the results of their diagnostic performance.
Diagnostic validity of SPTPS, CDUS and SPTPS+CDUS

{kind=link}
{kind=link}
Flow chart of the results of the diagnostic performance of SPTPS (A), CDUS (B) and SPTPS +CDUS (C). CDUS, colour duplex ultrasound; GCA, giant cell arteritis; HR, high risk; IR, intermediate risk; LR, low risk; SPTPS, Southend Pre-Test Probability Score.
Discussion
The diagnosis of GCA has evolved rapidly in recent years. Imaging has becoming increasingly recognised as a reliable and accurate tool for its diagnosis.2 The EULAR recommendations establish that in patients with a high clinical suspicion of GCA and a positive imaging test, the diagnosis of GCA can be made without any additional tests, while in patients with a low clinical probability and a negative imaging test, a diagnosis of GCA is considered unlikely.3 These recommendations have led to significant changes in the diagnosis of GCA and its introduction into clinical practice has been confirmed in recent articles that show a steady increase in the use of imaging as a diagnostic tool for this disease.10 In agreement with EULAR, the value of a positive imaging test is related to the degree of clinical suspicion, but as far as we know, this PTP has not previously been defined and is a subjective concept, with the attendant variability that can be introduced into the accuracy of the final diagnosis. In 2019–2020, the SPTPS reported its clinical PTP in order to gain adoption in a fast-track clinic.4 5 With an overall prevalence of 25%, in the HR group CDUS showed a sensitivity of 94%, a specificity of 85%, an accuracy of 92% and a GCA prevalence of 80%. In the LR group, CDUS showed undefined sensitivity (0/0), a specificity of 98%, an accuracy of 98% and a GCA prevalence of 0%, although in 70 LR patients CDUS was not performed because the suspicion of GCA was too low in the opinion of the authors.5 In our study, which showed a similar prevalence of GCA (32.7%), the objective was not to test the PTP against CDUS that all patients had, but rather against the gold standard diagnosis, which also included other imaging tests or TAB when the clinicians considered it appropriate, such as when monitoring the clinical evolution of a patient during follow-up. As can be seen from the results, the precision of the SPTPS is not sufficient for making a proper diagnosis, since in the LR group 10/135 (9.5%) patients had GCA. This could result in a significant number of patients going undiagnosed and untreated, thus leaving them vulnerable to serious complications from GCA. However, combining SPTPS results with CDUS findings, as recommended by EULAR, yields better results with less than 2% of misclassified patients. Thus, in the group with LR SPTPS and negative CDUS, there was only one false negative, an aortitis visualised by PET-CT. Moreover, it is well known that the validity of CDUS in evaluations of the aorta is low and in these cases the use of other imaging techniques for an accurate diagnosis is necessary. Similarly, when we reviewed patients with HR SPTPS and positive CDUS, only one case proved to be a false positive, an amyloidosis secondary to multiple myeloma, which is a disease that produces a true halo positive sign due to amyloid infiltration of the vessel wall.11 An additional clinical risk stratification result to consider is one that may aid the correct determination of false positives and false negatives, since two cases of atherosclerosis had an LR score and three of the false negatives of GCA with large vessel vasculitis involved HR or IR. In fact, according to the EULAR recommendations, this should have prompted the clinician to request an additional diagnostic test.
In terms of the limitations of this study, it was retrospective in nature, although the data obtained from the clinical histories was of good quality in terms of capture and a second investigator survey monitored the included data after the initial collection. It should also be noted that, in most cases, the CDUS result was taken into account when a final diagnosis was made by the physician in charge. However, the results also show that there were false positives that the clinician detected in the final diagnosis. In fact, four false negatives involved GCA with isolated large-vessel involvement diagnosed by PET-CT. Another limitation was that the value of each component of the SPTPS in the original article was assigned based on the experience of the authors, lacking any statistical calculations or other objective reasons to verify its accuracy in measuring the risk of GCA, problems that could be improved in the future.
In conclusion, our results show that the use of a clinical risk score such as SPTPS with TAs±large-vessel CDUS examinations confirms the validity of the EULAR recommendation on the usefulness of CDUS in diagnosing GCA in actual clinical practice. Furthermore, combining GCA clinical risk scores with CDUS could improve the detection of both false negatives and false positives.
Data availability statement
All data relevant to the study are included in the article. No additional data are available.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the local ethics committee (HULP PI 3040). Given the retrospective nature of the study, written informed consent of the individual patients was waived.
Acknowledgments
FERBT2021 - The authors thank the Spanish Foundation of Rheumatology for providing medical writing/editorial assistance during the preparation of the manuscript.
Footnotes
Twitter @EliFdezFdez
Contributors All the authors have participated in the preparation of this article. EFF wrote the first version of the manuscript. All authors reviewed it and made extensive comments and appropriate changes to it. All authors approved the final version of the manuscript. EdM acted as guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests EFF: None declared. IM: Speakers bureau: Roche, Novartis, UCB, Gedeon Richter; Consultant of: Roche. DP: None declared. AB: Consultancies or speakers bureau: Abbvie, Pfizer, BMS, Nordic, Sanofi, Sandoz, Lilly, UCB, Roche, Galapagos, Gilead. EdM: Speakers bureau: Abbvie, Novartis, Pfizer, MSD, BMS, UCB, Roche, Grunental, Janssen, Sanofi; Paid instructor for: Janssen, Novartis, Roche; Consultant of: Abbvie, Novartis, Pfizer, Galapagos; Grant/research support from: Abbvie, Novartis, Pfizer.
Provenance and peer review Not commissioned; externally peer reviewed.