Article Text

Abstract
Objective Serious infection remains a concern when prescribing immune-modulatory drugs for immune-mediated inflammatory diseases. The ‘summary of product characteristics’ (SmPCs) provide information on adverse events for example, infections, from clinical trials and postmarketing pharmacovigilance.
This review aimed to compare infection frequency, site and type across immune-modulatory drugs, reported in SmPCs.
Methods The Electronic Medicines Compendium was searched for commonly prescribed immune-modulatory drugs used for: rheumatoid arthritis, spondyloarthritis, connective tissue disease, autoimmune vasculitis, autoinflammatory syndromes, inflammatory bowel disease, psoriasis, multiple sclerosis and/or other rarer conditions.
Information was extracted on infection frequency, site and organisms. Frequency was recorded as per the SmPCs: very common (≥1/10); common (≥1/100 to<1/10); uncommon (≥1/1,000 to<1/100); rare (≥1/10,000 to<1/1,000); very rare (<1/10 000).
Results 39 drugs were included, across 20 indications: 9 conventional synthetic disease-modifying anti-rheumatic drugs (csDMARDs), 6 targeted synthetic DMARDs, 24 biologic (b)DMARDs.
Twelve infection sites were recorded. Minimal/no site information was available for most csDMARDs, certolizumab pegol and rituximab. Upper respiratory tract was the most common site, especially with bDMARDs. Lower respiratory, ear/nose/throat and urinary tract infections were moderately common, with clustering within drug groups.
Data for 27 pathogens were recorded, majority viruses, with herpes simplex and zoster and influenza most frequent. Variable/absent reporting was noted for opportunistic and certain high-prevalence infections for example, Epstein-Barr.
Conclusion Our findings show differences between drugs and can aid treatment decisions alongside real-world safety data. However, data are likely skewed by trial selection criteria and varying number of trials per drug and highlight the need for robust postmarketing pharmacovigilance.
- Infections
- Antirheumatic Agents
- Autoimmune Diseases
- Biological Therapy
Data availability statement
Data are available upon reasonable request. Data available upon request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Serious infection is a concern when prescribing immune-modulatory drugs for immune-mediated inflammatory diseases.
The European Medicines Agency ‘summary of product characteristics’ (SmPCs) data provide information on adverse events including infections; however, no comparison has been undertaken on reported infection frequencies across SmPCs for immune modulators.
WHAT THIS STUDY ADDS
We undertook a summary analysis of the SmPCs using a novel methodological approach to help clinicians visualise infection risk patterns across treatment strategies.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
Our findings can be used to visualise differences between drug infection risk profiles and aid treatment decisions and highlight the need for robust postmarketing pharmacovigilance studies with real-world safety data.
Introduction
Serious infection remains a risk in people with immune-mediated inflammatory diseases (IMIDs). One of the great challenges of contemporary disease care is balancing risk and benefit of immune-modulatory therapies. For most patients, these drugs provide a safe and effective method of disease control.1 Advances in targeted therapies for autoimmune diseases have been accompanied by a growing awareness of the potential to change infection risk.
Quantifying the risk of serious infection can be challenging, as they are relatively rare events. Primary clinical trials are not scrutinised and long-term extension data rarely focus on safety. We instead rely on real-world data such as registries. An example is the increased risk of serious infection in patients taking inhibitors of tumour necrosis factor (TNFis), demonstrated through studies of registry data in rheumatoid arthritis (RA), psoriasis and inflammatory bowel disease (IBD).2–5 Similar infection risks have also been shown with non-TNFi biologics, such as rituximab and tocilizumab, the latter being associated with serious bacterial skin and soft tissue infections.6 7
However, registry data are undermined by channelling bias and unmeasured confounding. Examining trial and long-term extension data combined would provide more power and overcome concerns around bias and confounding.
The European Medicines Agency (EMA) publishes a ‘summary of product characteristics’ (SmPC) for each drug on the European market, produced by the drug manufacturer. Stringent guidelines exist on the format and content of SmPCs.8 9 EMA requires patient-level data from both clinical trials and long-term extension data to be submitted and reviewed. Data informing risk are also gathered from spontaneous reporting, directly by regulators or indirectly via the marketing authorisation holder. Altogether these inform risk profiling, as detailed in the SmPCs, through estimated event rates.8 Information within the SmPCs is reviewed regularly (at least annually) and updated as and when new data becomes available. SmPCs are a crucial source of safety information for prescribers. However, to our knowledge, there has to date been no comparison undertaken on infection risk in immune-modulatory drug use, across SmPCs. Immune-modulatory drugs encompass conventional synthetic (cs), biologic (b) and targeted-synthetic (ts) disease-modifying antirheumatic drugs (DMARDs).
We sought to undertake a summary analysis of the SmPCs using a novel methodological approach to help clinicians visualise infection risk patterns across treatment strategies.
The rationale for this work was to be able to compare the information, provided by regulators, as detailed in the SmPCs. SmPCs follow a common format and requirements, enabling comparability across agents.
Methods
The search question was as follows: What is the frequency and nature of infection in patients with IMIDs taking immunomodulatory medication, as reported in the SmPC literature?
Participants
An SmPC for a given drug was included if the drug is licensed in Europe for the treatment of an IMID. This comprised rheumatic diseases such as: inflammatory arthritis (including RA, axial spondyloarthropathy, psoriatic arthritis), gout, connective tissue disease (eg, systemic lupus erythematosus, scleroderma, dermatomyositis), autoimmune vasculitis, autoinflammatory syndromes, juvenile idiopathic arthritis. Non-rheumatic diseases included: IBD (Crohn’s and ulcerative colitis), psoriasis, multiple sclerosis and other rarer conditions.
Intervention
The intervention is the use of an immune-modulatory drug for the treatment of IMIDs. Information on infections as an adverse event secondary to the use of the drug, as described in the SmPC, was extracted and analysed.
Comparator
A comparator or control is not directly relevant to this review, although patients with an IMID and not taking the immune-modulatory drugs under study could be considered as such.
Outcomes
Infection risk and frequency based on each immunomodulatory drug under study were recorded, described by infection site (eg, respiratory, urinary tract, skin, etc) and by type (eg, bacterial, viral, fungal, etc).
Study selection, data extraction and synthesis
The Electronic Medicines Compendium (EMC) was searched for the most commonly used immune-modulatory drugs in the treatment of IMIDs. The search and data extraction were performed on 28 September 2020.
Drugs were selected and agreed by all authors. Full length SmPC documents were manually searched for relevant information on infection risk and frequency, which was subsequently extracted from the Special warnings and precautions for use section and Undesirable effects section The Special warnings and precautions for use section includes data on serious adverse reactions, including infections, and consideration of at-risk groups. The Undesirable effects section contains details of infections from clinical trials, postauthorisation safety studies and spontaneous reporting, in which there is at least a reasonable possibility that these are as a consequence of the medicinal product. It is important to note that decisions on what is included in the SmPC can be subjective and may be the result of a consensus decision determined by the relevant committee on evaluation of the available data. In addition to in-depth data and description of these adverse events, details on frequency of subtypes of event (eg, site and type of infection) were extracted.
Twenty-five per cent of included SmPCs were screened and extracted by a second reviewer, using a purpose-built data extraction table. Disagreements were discussed until a consensus was agreed, with a third reviewer involved as needed. No papers, or additional data or supplementary material were required from authors.
Information on frequency of infection was recorded as per the convention in the SmPC documentation: very common (≥1/10); common (≥1/100 to<1/10); uncommon (≥1/1000 to<1/100); rare (≥1/10 000 to<1/1000); very rare (<1/10 000).8 Of note, not all ‘very rare’ infections may be included in a given SmPC—the threshold for inclusion may be subjective and be based, for example, on clinical importance of the infection. Any additional information was recorded within the extraction table with adequate referencing to the relevant SmPC. Information, where available, on infection site (eg, respiratory, skin, etc), type (eg, bacterial, viral, etc) and individual pathogenic organisms was also extracted.
Results
In total, 39 drugs were identified, used across 20 indications, including 9 csDMARDs, 6 tsDMARDs (4 Janus kinase inhibitors, 2 sphingosine 1-phosphate receptor modulators) and 24 bDMARDs (17 cytokine-targeted and 7 cell-targeted). All drugs are listed by DMARD category in table 1. All included SmPCs had been updated within 18 months of the search date.
Summary of immune-modulatory drugs included in this analysis, including date of last update to the summary of product characteristic (SmPC) document at the time of the search and data extraction
All SmPCs had areas of missing or unavailable data (ie, not reported within the SmPCs), possibly due to the rarity of events or rarest events not being reported. For infection sites, this was most marked for cladribine, upadacitinib, certolizumab pegol, ravulizumab, natalizumab and dupilumab, which reported frequency of infection for a maximum of two sites. All drugs had large amounts of missing or unavailable data for frequencies of infection with pathogen groups (eg, bacteria, fungi), aside from viruses, where there were no missing data. With regards individual organisms, a large amount of missing data was noted for most pathogens, especially opportunistic infections, again due to low frequency of events. Infections were more likely to be listed by site than organism.
Twelve sites of infection were recorded. Minimal or no site information was available for most csDMARDs and siponimod, certolizumab pegol and rituximab. Figure 1 shows the most common sites of infection listed by drug group. Upper respiratory tract was the most common site of infection, especially with bDMARDs. Lower respiratory, ear/nose/throat (including sinusitis) and urinary tract infections (UTIs) were moderately common, with clustering within drug groups, especially TNFis. No drugs reported the risk of cardiac infections. The eye, musculoskeletal, neurological oral and reproductive tract sites were the least commonly reported sites of infection.
Summary of common sites of infection for immune-modulatory drugs. Key: red = very common; orange = common; yellow = uncommon; green = rare; blank = no information available. Drugs with no frequencies reported for specific infection sites not included (azathioprine, ciclosporin, interferon beta, leflunomide, methotrexate, sulfasalazine, siponimod, certolizumab pegol, dupilumab).
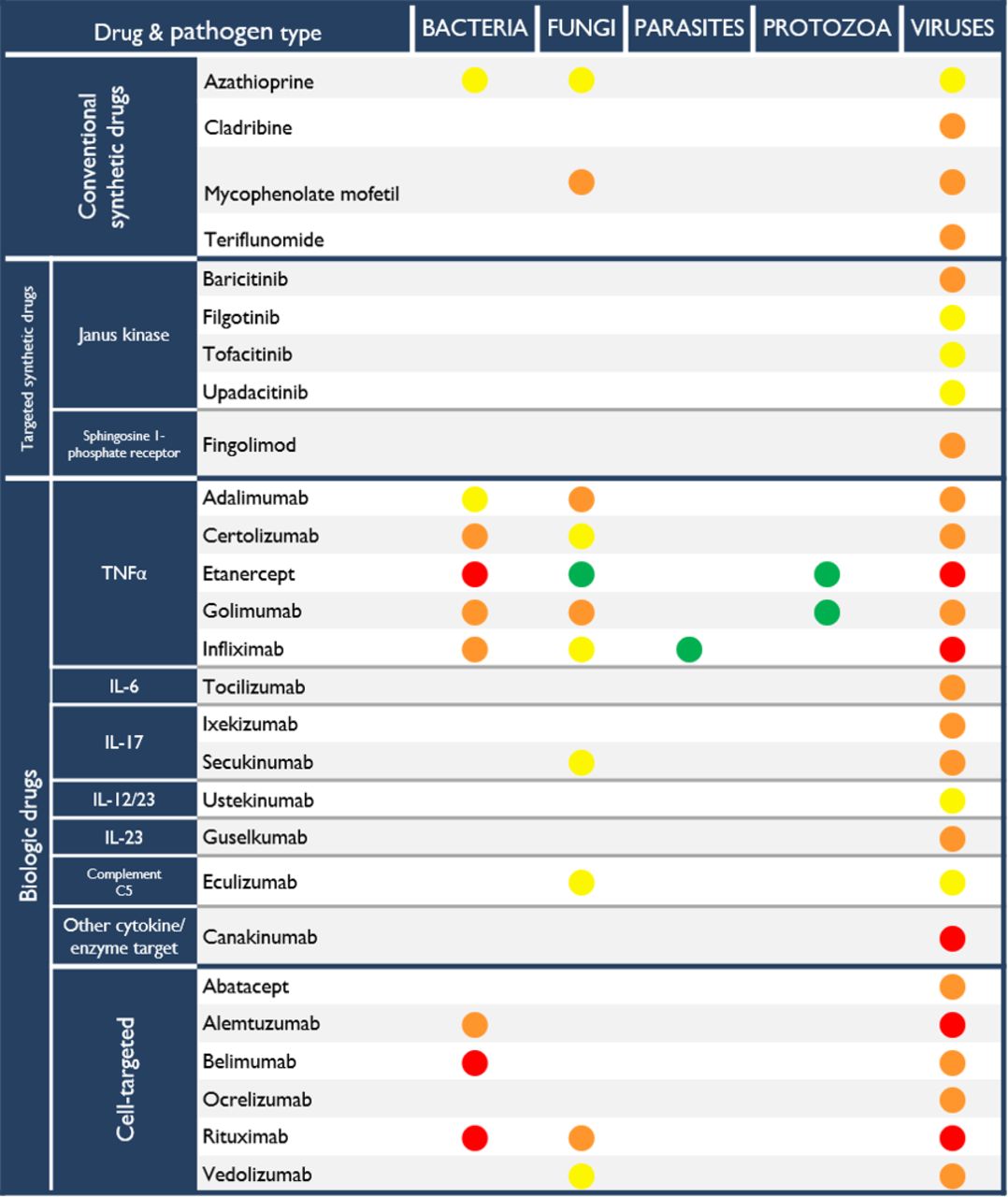
Infection data for 27 distinct pathogens were recorded, the majority viruses, especially with bDMARD use. Online supplemental figure 1 shows the most common pathogen subtypes by drug (where information was available). Specifically, herpes simplex and zoster were the most frequently listed pathogens (mainly with bDMARDs and tsDMARDs, most classed as ‘common’ in frequency), followed by influenza virus (common to very common with the use of several drugs across all categories; very common with the use of fingolimod, canakinumab, infliximab and ocrelizumab). Common non-viral causes of infection were candida and tinea species.
Supplemental material
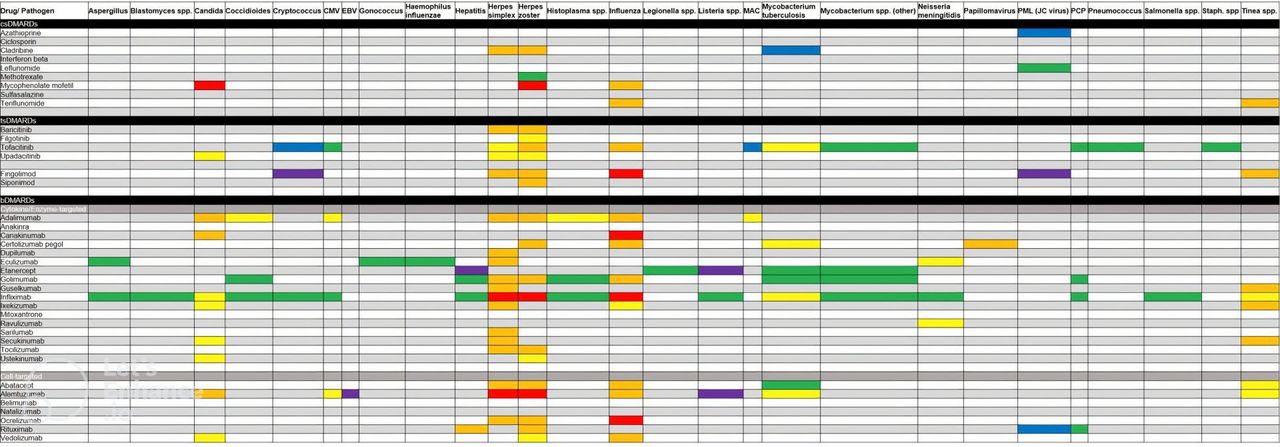
Variable or absent reporting was noted for opportunistic infections and certain viruses with high prevalence in the general population, for example, Epstein-Barr. Infection frequencies for several opportunistic infections were reported, with variable amounts of missing data. Frequencies of infection with fungi—especially candida and tinea species—had the least missing data. Infection frequency for mycobacterium tuberculosis (TB) was reported for 8 of the 39 drugs. Frequencies for other mycobacterial infections, including mycobacterium avium complex, were available for five drugs. Other opportunistic infections, including histoplasma, blastomyces and aspergillus had frequencies reported for three or fewer drugs. The full list of frequencies of infections with the individual pathogens, by drug, is found in figure 2. Cells are left blank where there is no mention of the infection within the SmPC. Colours denote the frequency reported within the SmPC, including where it is reported as ‘unknown’.
{kind=link}
{kind=link}
Summary of infection frequency with specific organisms for immune-modulatory drugs. Key: red = very common; orange = common; yellow = uncommon; green = rare; blue = very rare; purple = unknown; blank = no information available. bDMARDs, biologic disease-modifying anti-rheumatic drugs; csDMARDs, conventional synthetic DMARDs; tsDMARDs, targeted-synthetic DMARDs.
Discussion
The SmPC literature reports differences in infection risk, by site and pathogen, between immune-modulatory drugs, although accounting for the lack of standardisation of reporting. The findings can be used to visualise risk estimates, in a format that is easily and quickly legible. However, some of the patterns we have shown lack face validity to clinicians familiar with real-world safety data. Reasons for this include that the data are likely skewed in some cases by trial selection criteria, varying number of trials per drug, and quirks of individual study-reporting methodologies. In addition, data used to build SmPCs may fail to capture risk of rare infections, which may be detected in observational studies and real-world data.
To our knowledge, this is the first review comparing infection risk profile of immune-modulatory drugs, as detailed in the SmPCs. Previous studies have sought to compare other aspects of drug information reporting, such as drug interactions and contraindications in conditions other than the IMIDs.10–12 Similar to our findings, these also identified inconsistencies in reporting, especially when compared with real-world data, and potentially misleading information due to absent or contradictory information. All studies highlight the need to consult other sources prior to prescribing, and not relying solely on SmPC literature, for example, outcomes from observational studies from large-scale datasets.
The lack of reporting on rarer events, missing or unavailable data may in part be due to a lack of use of spontaneous adverse event reporting systems, such as the MHRA yellow card system, especially after a drug has been on the market for a period of time, leading to the Weber effect.13 This is the phenomenon of increased reporting of adverse events for new drugs in their first years of approval. The EMA guidance on the production of SmPCs requires information on adverse events to comprise both trial and real-world data.8 9 SmPCs for newer drugs are, therefore, likely to have their adverse event profile based on trial data, whereas older drugs are more likely to have a greater real-world evidence base. Nonetheless, rarer infections may also be more likely to be reported with newer drugs such as tsDMARDs and IL-17 inhibitors, in comparison to drugs which have been on the market for longer and there is, therefore, awareness and management of risk, for example, TNF inhibitors and tuberculosis.
With regards to sites of infection, upper respiratory tract infections (URTIs) were noted to be common with all drugs, except cladribine, indicating this is a poor discriminator for drug choice. In contrast, UTIs varied much more in frequency, with less frequent reporting for classes such as IL-17 inhibitors. There is also within-drug variation in the frequency of infections at different sites, for example, for abatacept, gastrointestinal infections are classed as rare, compared with ENT and URTI, which are very common. This is insightful as no studies to date have examined infection risk by site for a single drug. Abatacept overall appears to be associated with infections at all sites. The SmPC data would, therefore, suggest that it is not a good drug for patients at risk of infection. However, this is in contrast to registry data, which has generally reported a good infection safety profile compared with other biologics such as the commonly used TNF-inhibitors, although the EMA SmPC guidance stipulates that these data should be used in the production of SmPCs.7 14 15 The SmPC may report a greater number of infection sites for abatacept compared with other bDMARDs due to variations in trial data and reporting between drugs. This is a good example of the discordance between SmPCs and real-world registry data, which will be familiar to clinicians prescribing biologic drugs in clinical practice. It is also important to note that target populations for patients taking abatacept may be different to those taking TNFi (eg, RA vs psoriasis and IBD), and this will affect infection rates—in this example, infection rates are overall higher in RA compared with psoriasis and IBD. This reflects a limitation of the SmPCs, in that adverse events are not segregated by disease.
Variable or absent reporting was noted for most of the biologic DMARDs. This may be due to missing or unavailable data or due to number of patients being too low for very rare events to have occurred. It may also be the case that even if an event did occur, it simply was not reported in the SmPC document. Rituximab is a commonly used medication for the management of IMIDs such as RA and ANCA vasculitis. However, SmPC literature, based on pharmacovigilance data, was only able to provide information on respiratory tract infections and few organisms. In contrast, real-world registry data have been able to assess incidence ratios of infections, serious infections and hospitalisations with the use of this drug, as well as of individual infections.7 16 The same is true of other drugs with sparse infection frequency reporting in the SmPCs, such as abatacept, tocilizumab and anakinra.7 17 Interpretation of the SmPC data requires the user to appreciate that these could represent with no data or few data. For newer drugs, this is most likely explained by no or few events. For older drugs, it is likely to be due to true missing data, due to historical reporting methods in clinical trials and postmarketing pharmacovigilance. Of note, only two drugs, tofacitinib and abatacept, report ‘rare’ sites of infections, for skin and gastrointestinal infections, respectively.
Reporting of infection frequencies within the table of adverse events in the SmPCs is not within the context of individual IMIDs. Information within them, therefore, requires cautious interpretation or the details of trial data that can be found for some indications, but not all, within the document. For example, infections at all sites are reported as ‘very common’ for canakinumab, a drug used in the treatment of periodic fever syndromes. The reported infection profile may reflect the underlying disease state, rather than the side-effect of the drug.
There is some face validity to the results described, for example, the risk of lower respiratory tract infections and skin and soft tissue infections appear to be more frequent with TNF inhibitors, mirroring real-world data,2 3 18 whereas these infections are less common with the use of IL-23 inhibitors. However, some of the results from the SmPCs lack face validity. When considering individual pathogenic organisms (figure 2), certain infections are overrepresented compared with the time spent managing them in clinical practice, for example, candida. This may be due to certain infections being especially targeted or investigated, in comparison to infections with lower incidence. There is also no differentiation in this case as to whether this pertains to oral thrush or invasive candidiasis, two conditions with vastly different clinical features, management and prognosis. There are few missing data for organisms that are relatively prevalent, such as influenza, herpes zoster and herpes simplex. There is a relative underrepresentation of opportunistic infections, such as TB, given the importance of these for a patient’s clinical course and choice of immunosuppressant. There are also certain associations that appear to be absent from the SmPC data, for example, natalizumab has association in clinical practice with progressive multifocal leukoencephalopathy secondary to JC virus. However, despite being discussed within the SmPC, its frequency is not reported as an adverse event. This is likely because the event is too rare. Similarly, trials on baricitinib included cryptococcus, but the frequency of this infection is not reported in the SmPC, although it is for tofacitinib. It may therefore be prudent in future for drugs of a similar type or target to have a standardised template by which to report events within the SmPCs. It is important to note that the SmPC guidelines specifically state that the section on undesirable events should ‘also inform on adverse reactions with very low frequency or with delayed onset of symptoms which may not have been observed in relation to the product, but which are considered to be related to the same therapeutic, chemical or pharmacological class. The fact that this is a class attribution should be mentioned’.8 9
Finally, there is a discrepancy between reporting on sites of infection (figure 1) and individual organisms (figure 2). This is demonstrated by the C5 inhibitors, eculizumab and ravulizumab. While ravulizumab is reported as being strongly associated with ENT and URT infections, there is a lack of reporting on individual organisms. In contrast, eculizumab lists all sites of infection as uncommon or common but only reports frequency data for six specific organisms.
There are several limitations to this work. This is a secondary analysis of the data. Therefore, if there is an error in the reporting of data within the SmPC by the EMA, it will be carried forward as we were unable to review the original data. Safety signals that have emerged postlicensing will not necessarily be listed on the SmPC documents as there may be a lag in updating them. The data within the SmPCs depend on the drug company and how the trials are designed to capture and report adverse events. While there are EMA guidelines on the format and content of the SmPCs, these are open to interpretation by drug companies producing them. SmPCs also report only generic drug information (ie, not specific to certain patient demographics or subgroups), influenced by sampling bias of clinical trial recruitment. Patient numbers are not reported, so it is not possible to known the sample size on which information on adverse events has been based. In addition, infection risk is affected by a number of factors including demographics such as age, the primary autoimmune diagnosis, as well as co-treatment with corticosteroids, which will be applicable to many patients taking these immune-modulatory drugs.
While it is useful to compare data across SmPCs, it is not possible to perform a ‘ead-to-head’ trial between them, due to the vast variation in trial designs and reporting methods. This will subsequently influence any between-drug differences. Nonetheless, our comparisons have potential use in clinical practice. For patients with recurrent infections at a given site, clinicians can use the charts for cross-drug comparison, as a point of reference to choose drugs with less frequent infections, although being mindful that absent or rare events may indicate less reporting of infection, not necessarily low frequency. Similarly, for patients with a history of infection with a specific organism or opportunism, visualisation of organism data can help select drugs with a weaker signal for these infections. However, to have sufficient face validity for comparisons between SmPCs to alter care, the EMA would need to ensure more detailed information on source data within the tables in the SmPCs, especially with regard adverse events with drug use in different diseases. Ultimately, drug choice is individualised, dependent on both patient and clinician.
In conclusion, the SmPC literature is an important source of information on infection frequency, including on individual types and infectious organism. Our comparison of SmPCs across immune-modulatory drugs shows striking patterns, including the similarities and differences in infection, which can be used to guide prescribing decisions in this high-risk population. However, we have also highlighted the need for robust postmarketing pharmacovigilance studies, and the importance of using SmPC data alongside other sources when assessing infection risk.
Data availability statement
Data are available upon reasonable request. Data available upon request.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @ElenaNikiUK
Contributors MD, AC, EN and JG developed the idea and search strategy for this work. MD and KB extracted data from relevant sources. All authors were involved in the synthesis of the paper and editing the final manuscript. JG is the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.