Article Text

Abstract
Introduction MRI sensitively depicts erosions, bone marrow edema (BME) and synovitis in rheumatoid arthritis (RA). Recently developed European League Against Rheumatism (EULAR) recommendations stated that MRI is valuable to improve the certainty of a considered diagnosis and to detect structural damage at an early time point. However, these recommendations were mainly based on the data of patients with RA; prevalences of MRI features in the general population were not extensively explored. We reviewed the literature on MRI studies including symptom-free persons to assess the occurrence of MRI features.
Methods Medical literature databases up to September 2013 were systematically reviewed for symptom-free persons with MRI data on metacarpophalangeal, wrist and metatarsophalangeal joints. Data were extracted and summarised. When allowed because of comparable scanning and scoring protocols, a mean frequency of features was calculated.
Results Of the 338 articles screened, 31 studies evaluated MRI findings in symptom-free persons (n=516 in total). Both the imaging techniques (<1/≥1 T, with/without contrast enhancement) and the scoring methods (non-validated or RA MRI score (RAMRIS)) varied widely, prohibiting direct comparisons of the results of many studies. 15 studies scored data according to RAMRIS; combining data of similar joint regions showed that erosions (RAMRIS ≥1) were present in 33–52% of symptom-free persons. Similarly, synovitis was present in 27% and BME in 0–16% of symptom-free persons. The prevalence of MRI-detected erosions increased with age.
Conclusions MRI features, erosions in particular, occur frequently in symptom-free persons. Before MRI can be implemented in the diagnostic process, larger studies should be conducted determining the degree and combination of MRI features that are disease specific.
- Rheumatoid Arthritis
- Magnetic Resonance Imaging
- Early Rheumatoid Arthritis
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
MRI detected erosions, synovitis and bone marrow edema occur frequently in symptom-free persons.
Owing to the of heterogeneity in the studies, RA-specific MRI criteria cannot yet be defined.
Before implementing MRI in the diagnostic process of joint symptoms, further research is needed.
Introduction
Early treatment initiation in rheumatoid arthritis (RA) is associated with less radiographic progression and a higher chance to achieve disease-modifying antirheumatic drug-free sustained remission, illustrating the relevance of early diagnosis.1–6 To what extent MRI is valuable for early detection of RA is undetermined. However, the recently formulated European League Against Rheumatism (EULAR) recommendations for the use of imaging in the management of RA suggest that MRI can improve the certainty of the diagnosis of RA and detect structural damage at an earlier time point than radiographs.7 Additionally, an imaging task force of the American College of Rheumatology recently concluded that, of all imaging modalities, MRI serves best to ascertain structural damage in trials.8 These recommendations were mainly based on MRI data of patients with RA; MRI features that are present in the general population were scarcely considered.7 ,8
Furthermore, many studies in RA are currently investigating the preclinical phases of the disease because the processes occurring in these phases may influence the long-term course of the disease. Potentially very early detection of RA may allow intervention in an asymptomatic preclinical disease phase. Indeed, several recent studies reported that MRI may play a role in the identification of joint inflammation in the phase before it becomes clinically detectable.9 ,10 More studies are needed to determine the value of novel imaging modalities in the early detection of RA and their ability to differentiate patients with the disease from the normal situation.
Thus, to arrive at an evidence-based evaluation on the role of MRI in the diagnostic process in the early clinical and preclinical phases of RA, it is necessary to investigate the occurrence of MRI features in the general population. In case certain MRI features (to a certain degree) are also present in persons without joint symptoms, these lesions are presumably not indicative for RA. No large-scale studies have been performed to investigate the prevalence of these features in the general population. However, several MRI studies included symptom-free persons as controls.10–41 We aimed to (1) evaluate the prevalence of MRI features in symptom-free persons and (2), based on these observations, to make recommendations for future studies. To this end, we systematically reviewed the literature.
Method
The databases PubMed, EMBASE and Web of Science up until September 2013 were searched with the assistance of a medical librarian (JWS). Central terms in our search were MRI, healthy volunteers, wrist, metacarpal, metatarsal and RA (complete details of the search strategy can be obtained by the author). Titles and abstracts were screened on whether data on symptom-free persons and MRI of hands or feet were available. Subsequently, full-text articles were read and additional articles were identified through hand searching of reference lists. Articles were included when the studies contained (1) symptom-free persons and (2) information on MRI detected erosions, bone marrow edema (BME), synovitis or tenosynovitis of hands or feet. Since the symptom-free persons were generally used as the control group, the quality of the overall study design was not valued. Further, in order to get a comprehensive overview, we decided to include all studies fulfilling these two criteria and not to exclude studies based on the quality of the scanner, the scan protocol or scoring protocol that was used.
A standardised form was used to extract the following data: (1) study population (population size, age, recruitment method, description of study population, MRI scanner, MRI sequences, joint region scanned and scoring method), (2) MRI features (erosions, BME, synovitis and tenosynovitis) and quantitative aspects (number of patients affected, number of joints/bones affected and grading of the MRI features) and (3) relevant characteristics (location of MRI features, dominant or non-dominant hands, age and sex of symptom-free participants). MRI features were present (‘positive’) when recorded as such; studies using the RA MRI score (RAMRIS) generally considered a score of ≥1 for that feature as positive.10 ,27–40 Data were extracted and reported such as done by the authors: either by presenting the prevalence of a feature or by presenting summary measures of continuous RAMRIS. According to RAMRIS, the range per bone/joint of erosion, BME and synovitis scores are 0–10, 0–3 and 0–3, respectively; scoring of the metacarpophalangeal (MCP) region and wrist region involved evaluation of 8 and 15 bones and 4 and 3 joints (radioulnar joint, radiocarpal joint and intercarpal-carpometacarpal joint), respectively, evaluation of the 5 metatarsophalangeal (MTP) joints involved evaluation of 10 bones. In case the same joint regions were assessed using similar scan protocols (ie, either with or without use of contrast enhancement) and similar scoring methodology (RAMRIS), it was considered acceptable to combine the results of different studies. Then mean frequencies (with 95% CIs) were calculated. Since it is known that contrast enhancement increases the reliability of assessment of synovitis,42 studies evaluating synovitis and tenosynovitis with and without contrast enhancement were not combined but analysed separately.
Results
Selection of studies
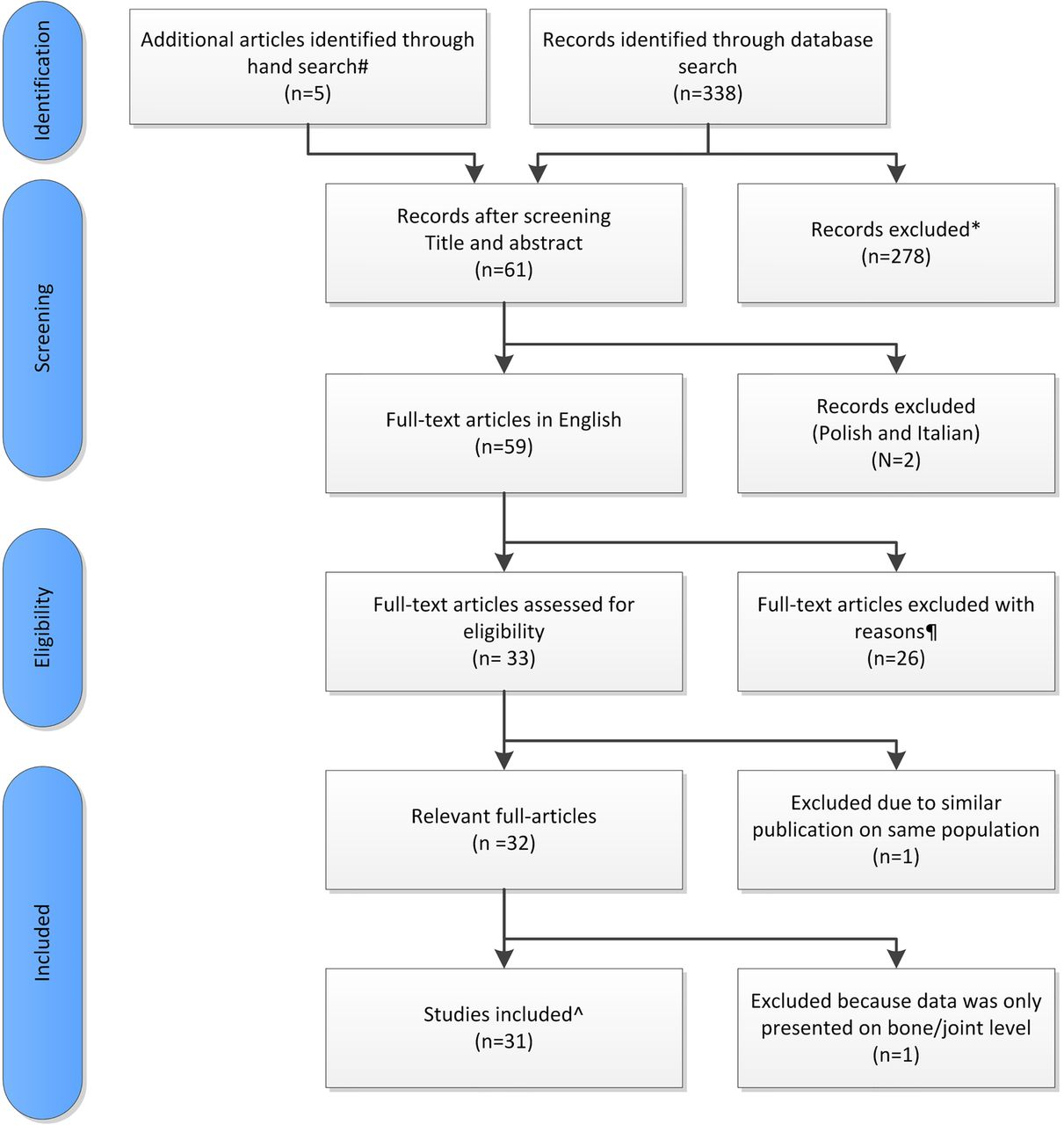
The literature search yielded 338 studies; five additional articles were found by hand searching of reference lists (figure 1). After screening, 61 articles were selected. Two studies were excluded because of a language other than English. Of the remaining articles, 33 were eligible for inclusion. One article was excluded as it concerned a population that was used in two articles. Consequently, data were extracted of 32 articles. Whereas 31 studies provided data on patient level (joint region), one study analysed the data only on individual bone/joint level; therefore, this study was only used when analysing results on bone/joint level.41

{kind=link}
Overview of literature research. #Articles identified bij hand searching of reference lists. *Articles were excluded when no data on symptom-free persons or MRI features of hands or feet were described. ¶Articles were excluded when no data were presented on erosions, BME, synovitis or tenosynovitis in symptom-free persons. ^The data of the 31 included studies provided data on patient level.
Study description
The 31 included studies contained information on 3–42 (range) symptom-free persons per study; in total, 516 symptom-free persons were studied (table 1). Descriptions of the recruitment method is given in only seven studies.12 ,23 ,24 ,26 ,31 ,32 ,36 Most of these studies are reported to have studied hospital staff. Methods to exclude the target disease were described in 26 articles; four studies did not include this information and described their symptom-free persons as ‘healthy volunteers’11 or ‘healthy controls’14 ,37 ,38 and one study was described to have performed MRIs of ‘healthy volunteers’ and persons with wrist instability.26 The methods of excluding target disease differed. Thirteen studies described that there was no history of joint disease, arthritis or joint symptoms.15–17 ,19–22 ,24 ,28–30 ,36 ,39 Twenty studies mentioned that there were no current musculoskeletal/joint symptoms.10 ,12 ,13 ,18 ,20 ,21 ,23–25 ,27–34 ,36 ,39 In four studies, persons underwent clinical assessment by a rheumatologist,24 ,27 ,29 ,36 and in two studies laboratory investigations were done and persons were excluded in case they were rheumatoid factor positive or had increased C reactive protein levels.32 ,33
Characteristics of the 31 selected studies
Of the 31 included studies, 19 used an MRI with ≥ 1 T, 11 with an <1 T MRI and one study used two different scanners (one with 1 T and one with 0.6 T).34 Contrast enhancement was used in 17 of the 31 studies.
Sixteen studies did not use a validated scoring method; evaluations were done by experienced radiologists (in 12 studies), an experienced rheumatologist (1 study) and an ‘observer’ (2 studies), and in one study no information was provided. In 15 studies, MRIs were scored according to RAMRIS.43 MRI scoring was done blinded for clinical status in 18 of the 31 studies. In seven studies, scoring of patients and controls was not performed blindly,10 ,15 ,20 ,23 ,27 ,34 ,40 and in six studies (140 symptom-free persons) only symptom-free persons were evaluated.22 ,23 ,28 ,30 ,32 ,36
Prevalence of erosions
The studies that did not use a validated scoring method reported a lower prevalence of erosions than did the studies using RAMRIS (table 2). A wrist was scanned on one or both sides and assessed using RAMRIS in 69 and 44 persons, respectively. When combining data of the wrist, a total RAMRIS erosion score ≥1 was reported in 52.2% (mean, 95% CI 40.6 to 63.5, unilateral wrist)27 ,34 ,37 and 40.9% (95% CI 27.7% to 55.6%, both wrists)35 ,36 of symptom-free persons, respectively. Unilateral MCP joints were evaluated in 97 persons and revealed erosions in 33% (95% CI 24.4% to 42.9%).27 ,34 ,38 ,39 No studies described the prevalence of erosions when using higher cut-offs for positivity (for instance, a total RAMRIS erosion score of ≥2).
Frequency of erosions, BME, synovitis and tenosynovitis in symptom-free persons
Prevalence of BME
The recorded prevalence of BME was higher in the studies using RAMRIS than in the studies using other methods. Combining the data of the 63 persons in whom unilateral wrists were scanned yielded a mean frequency of BME (RAMRIS BME score ≥1) of 15.9% (95% CI 8.7% to 27.0%).27 ,34 Similarly, BME was present in 9.5% (95% CI 4.1% to 19.6%)27 ,34 of persons in whom unilateral MCPs were evaluated. Combining studies assessing unilateral wrist and MCPs showed a mean frequency of BME of 0.0% (95% CI 0.0% to 6.8%).29 ,30 No studies categoried BME features with higher cut-off values.
Prevalence of synovitis and tenosynovitis
Synovitis was assessed without contrast enhancement in 8 studies and with contrast in 13 studies. In the studies that used no validated scoring method, synovitis was present in 0–4.8% (range) of persons when no contrast was used13–15 ,20 and 0–44.4% (range) when contrast was used.11 ,16–19 ,22 ,26 In the studies that were scanned with contrast enhancement and scored according to RAMRIS, synovitis was present (total synovitis score ≥1) in 26.7% (95% CI 15.8% to 41.2%); these studies assessed wrist and MCP joints together.29 ,30 Data on the studies that provided results of wrist or MCP joints separately were not combined due to differences in scanning or scoring protocols. Tenosynovitis was assessed infrequently (table 2).
Continuous RAMRIS-scores
Three studies did not report categorised data but reported continuous RAMRIS, incorporating a semiquantitative evaluation of the severity of the features.10 ,27 ,28 The mean RAMRIS for erosions and BME were low (≤3.2 and 0.9, respectively, table 3). For synovitis, contrast enhancement was used in one study;28 this study revealed higher mean RAMRIS synovitis scores than did the two studies without contrast (mean synovitis scores >3 vs <1, respectively; table 3).10 ,27
Mean RAMRIS score in symptom-free persons
Prevalence of lesions at the bone and joint level
In the aforementioned studies, total scores per joint region were evaluated. Several studies evaluated the prevalence of MRI features on the level of individual bones and/or joints, all defining a RAMRIS of ≥1 as positive.24 ,29–32 ,36 ,39 ,41 Erosions were analysed in six studies; among the 4696 bones evaluated, 161 showed erosions 3.4% (95% CI 2.9% to 4.0%).30–32 ,36 ,39 ,41 BME was analysed in only two studies; among the 1182 bones evaluated, five were positive for BME 0.4% (95% CI 0.2% to 1.0%).24 ,32 Three studies analysed 471 joints on synovitis and reported the prevalence of synovitis in 42 joints 8.9% (95% CI 6.6% to 11.9%).29 ,30 ,41
The severity of the individual lesions was scarcely reported. Three studies contained information on the severity of erosions and reported that 80.8% (mean, 95% CI 72.8% to 86.9%) of the recorded erosions had a score of 1.31 ,32 ,36 None of the studies reported on the severity of BME or tenosynovitis at the local level. Two studies described the synovitis scores in more detail; 21 joints had a RAMRIS of 1 (95.5%), a RAMRIS synovitis score of 2 was seen in 1 joint (4.5%) and no joints had a RAMRIS of 3.29 ,30
With regard to the location of the MRI features, erosions and synovitis were more often observed in the wrist than in the MCP joints.20 ,31 ,32 The locations of erosions were evaluated in seven studies at the bone level; most erosions were observed in the carpal bones; however, there was no clear agreement on which carpal bones showed erosions most frequently.30 ,32 ,35 ,36 ,41 Erosions were rarely scored on the metacarpal-1 and trapezium (bones that might also be affected by osteoarthritis).30–32 ,35 ,36 Locations of BME and synovitis were not clearly reported.
Relevant characteristics
We next evaluated to what extent differences in the scanner or differences in persons’ characteristics influenced the results. No different prevalences were observed when comparing extremity-MRI10 ,12 ,13 ,27 ,31–33 ,35 with whole-body MRI.11 ,14–26 ,28–30 ,36–40 When comparing the prevalence of MRI features in studies that used MRI scanners with <1 Tesla (T)12 ,13 ,16 ,20 ,31–33 ,35–38 and those with >1 T,10 ,11 ,15 ,17 ,18 ,23 ,24 ,26 ,28 ,29 ,39 ,40 a higher prevalence of erosions was detected with <1 T scanners (mean 38% vs 24%). Owing to the heterogeneity between studies, no summary results can be provided with regard to the prevalence of MRI inflammatory features in relation to the field strength of the MRI. When comparing the studies that evaluated the MRIs blindly versus those that scored the MRIs knowing that the persons were symptom-free, no differences in the prevalences of the different MRI features were observed.11–14 ,16–19 ,23–26 ,29 ,31 ,33 ,35 ,37–39
The dominant and non-dominant hands were evaluated in two studies and no significant differences were observed.31 ,36 Differences in the frequency of features between sexes were also not detected.32 Four studies compared the prevalence of MRI features between age categories and showed a non-significant tendency to27 ,32 or a significant31 ,36 higher prevalence of MRI erosions in older persons. Synovitis and BME were less frequently studied in relation to age, although a significant difference in two studies was observed with higher prevalences at older age.31 ,36 No information was provided on the location or the grading of the erosions and the inflammatory features observed in symptom-free persons of different age categories.
Discussion
MRI is an imaging method that is very sensitive in detecting inflammation and also bone erosions. This makes MRI an interesting tool to measure the course of the disease in randomised clinical trials and this suggests that MRI may also be useful in the diagnostic process. When MRI would be implemented in practice in the diagnostic workup of joint symptoms, it is crucial to consider the prevalence of MRI features in the general population to prevent false-positive findings due to positive labelling of features that are (also) present in the normal situation. We reviewed the literature systematically to get an overview of the reported prevalence of features in symptom-free persons. The large majority of these studies were not designed to determine the frequencies of MRI features in the general population but used symptom-free persons as the control group. In addition, there were considerable differences in methodology of the selection of volunteers, MRI protocols and MRI scoring. This resulted in heterogeneous data. Indeed, considerable differences in the frequencies of MRI features in symptom-free persons were observed in the different studies. We combined the data of the studies that had similar scanning and scoring protocols and, based on the data available, we observed that all MRI features studied were present regularly and that MRI detected erosions were present most frequently (in 33–52% of symptom-free persons).
Most studies described their findings at the patient/joint region level and not at the level of individual bones or joints. However, studies that did include evaluation at the bone level showed that most lesions were mild (RAMRIS of 1). Furthermore, we noted a lower prevalence of all MRI features (erosions in particular) in studies not using RAMRIS than in those using the RAMRIS method. This may possibly reflect that the RAMRIS method is sensitive and that radiologists evaluating the MRIs using clinical experience may more often report an MRI as normal. Additionally, most of the studies that did not use the RAMRIS method were done when MRI techniques were less developed.11 ,12 ,14–22 ,24 ,25 ,44
Of all MRI features, the prevalence of synovitis varied the most between studies. This cannot be explained only by the absence or presence of contrast enhancement that may increase the sensitivity and specificity of identifying MRI-detected synovitis as both types of studies were evaluated separately.42 ,45 ,46 The reasons for these differences between studies are unclear to us.
The most important limitation of this review is the heterogeneity of the data collected, which is a result of the methods with which data were collected in the individual studies. For instance, in many studies the symptom-free persons were used as the control-group and information on how the symptom-free persons were recruited was missing. Some studies included symptom-free persons only and did not use the symptom-free persons as controls.22 ,23 ,28 ,30 ,32 ,36 A consequence of this latter approach is that the evaluators per definition were aware that they had evaluated scans of symptom-free persons. Hypothetically, awareness of the clinical status may affect the scoring with lower scores being given to symptom-free individuals. In addition, the methodology to rule out rheumatic diseases differed between the studies. A difficult issue is to what extent osteoarthritis was ruled out; joint space narrowing or other osteoarthritic features were not assessed in these studies, so no definite conclusions can be drawn as to what extent the presence of asymptomatic osteoarthritis has affected the results. Furthermore, recent studies indicated that ACPA can affect the bone in the absence of clinically apparent arthritis and that subclinical inflammation may precede clinical arthritis.9 ,10 In two studies, the symptom-free persons underwent laboratory testing and in three studies the symptom-free persons were even followed (for 1–5 years); none of these persons developed RA.
Another important limitation relates to the issue when it is allowed to combine the results of different studies. We combined results of studies that used similar scan protocols (same joints and uniformity in contrast enhancement) and similar scoring protocols. Still, the summary measures that we provided should be interpreted with care as the readers of the different studies were not trained together and inter-reader differences and other causes of heterogeneity most likely exist. Nevertheless, this review gives a first impression of the MRI features present in the general population.
It can be argued that more stringent quality criteria should be applied before it is acceptable to combine the results of different studies. For instance, the following quality criteria might be reasonable: (1) the recruitment method was described, (2) appropriate methodology was used to exclude persons with joint symptoms or joint disease, (3) the field strength of the MRI was ≥1 T and (4) scans were scored according to the RAMRIS method. None of the 32 studies included in this review fulfilled all these four criteria. This underlines that large, high quality studies on this subject are needed. Recommendations for the set-up of such studies are proposed in box 1.
Recommendations for high-quality studies, formulated based on the findings of this review
Include a large number of symptom-free persons
Include persons of different age categories
Apply population-based recruitment methods
Describe the recruitment methodology
Apply thorough anamnesis and physical examination to exclude the presence of joint symptoms or signs of joint disorders.
Perform similar MRI scans in all persons
MRI strength of ≥ 1 Tesla
Use contrast enhancement
Score the MRIs according to RAMRIS
Also include MRIs of persons with joint diseases (eg RA) and score the MRIs blinded to the clinical status
Perform analyses stratified for age
Furthermore, several questions still have to be answered. More detailed studies are needed on the prevalence of MRI-detected erosions, BME, synovitis and tenosynovitis in the symptom-free persons in relation to age. Furthermore, the location and the co-occurrence of erosions and inflammation (BME, synovitis or tenosynovitis) could be important for differentiation. In none of the studies was it reported whether the erosions were accompanied by inflammatory lesions, which may also be relevant to differentiate early disease from normal variants, as disease-specific erosions might presumably more often be accompanied by measures of inflammation. Also the extent or severity of the lesions may be useful to take into account. Ultimately, comparing a large number of MRI scans of healthy persons and early RA patients will reveal which combination of features are disease specific and will allow MRI criteria specific for early disease to be defined.
In conclusion, MRI features, erosions in particular, occur frequently in symptom-free persons and are more prevalent with increasing age. Before MRI can be implemented in the diagnostic process of arthritis, further evaluation of these features in symptom-free persons is required. Preferentially, this is done in large studies, ensuring homogeneity in the scan-protocol and scoring method, by evaluating scans of symptom-free persons as well as early arthritis patients blinded to the clinical status.
References
Footnotes
Contributors LM and AHMvdHvM contributed to the conception and design of the study. All authors acquired or analysed the data. LM and AHMvdHvM contributed to the interpretation of the data. All authors contributed to the final version of the manuscript.
Funding The research leading to these results was funded by a Vidi-grant of the Netherlands Organisation for Scientific Research, he FP7 HEALTH program under the grant agreement FP7-HEALTH-F2-2012-305549, a grant of the Dutch Arthritis Foundation and the EU euroTEAM.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.