Article Text

Abstract
Objectives To describe changes in drug treatment and clinical outcomes of ankylosing spondylitis (AS) during the past decade.
Methods The national database of the German collaborative arthritis centres collects clinical and patient-derived data from unselected outpatients with inflammatory rheumatic diseases. Cross-sectional data from 2000 to 2012 of around 1000 patients with AS per year were compared with regard to clinical presentation and quality of life indicators.
Results Non-steroidal anti-inflammatory drugs (NSAIDs) have been the predominant treatment choice in AS over the years with a prescription rate of 67% of patients in 2012. Currently, almost half of the patients with AS in German rheumatology centres are treated with tumour necrosis factor inhibitors (TNFi). Often, both treatments are used in combination (33%), followed by combinations of NSAIDs and synthetic disease modifying antirheumatic drugs (sDMARDs) with 23% or TNFi alone (21%). In 2012, 10% of patients each received NSAID or sDMARD monotherapy. Methotrexate, sulfasalazine, glucocorticoids and analgaesics alone or in combination with other treatments were given to 10% of patients, respectively. Over the years, we have seen remarkable improvements in disease control and patient reported outcomes. These developments are consistent with enhanced functional status, increasing employment rates and decreasing sick leave, hospitalisation and work disability.
Conclusions In the German rheumatology secondary/tertiary care setting, routine care of patients with AS has changed tremendously during the past decade. Increasingly, more efficacious treatment options are reflected in improved clinical outcomes, quality of life and participation in the labour force.
- Ankylosing Spondylitis
- Treatment
- Outcomes research
- Health services research
- Anti-TNF
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Ankylosing spondylitis (AS) is among the most common inflammatory rheumatic diseases and as a progressive disease leads to structural damage, functional disability and a decrease in quality of life.
Non-steroidal anti-inflammatory drugs (NSAIDs) are known to improve clinical symptoms in 70–80% of treated patients, and are recommended as the first choice treatment, while tumour necrosis factor inhibitors (TNFi) are recommended to be applied after non- or unsatisfactory response to NSAIDs.
What does this study add?
Routine care of patients with AS has changed tremendously during the past decade with NSAIDs and TNF inhibitors being the most frequent treatment choice in German rheumatology today.
Clinical outcomes, quality of life and participation in the labour force have remarkably improved.
How might this impact on clinical practice?
Our findings should encourage physicians to further optimise individual treatment, knowing that in addition to a better disease control they can also improve social and work participation, and, thereby, the quality of life of their patients.
Introduction
Ankylosing spondylitis (AS) is among the most common inflammatory rheumatic diseases and the major subtype of the group referred to as spondyloarthritides (SpA). This group can be divided into predominantly peripheral and predominantly axial forms of SpA, with AS being assigned to predominantly axial SpA.1 AS is more often diagnosed in men and has its usual onset between 25 and 40 years of age.2–4 As a progressive disease, it leads to structural damage, functional disability and a decrease in quality of life.4
Typically, AS leads to radiographic changes in the sacroiliac joints and spine, although the onset of low back pain often dates back several years, before radiographic signs can be found.5 Although MRI technology now allows for the detection of active inflammation of the sacroiliac joints, which is assumed to be one sign of a potentially evolving AS,5 ,6 the diagnosis and subsequent therapeutic interventions remain a challenge. While synthetic disease-modifying antirheumatic drugs (sDMARDs) are known to be effective in peripheral forms of SpA, no substantial outcome improvement could be verified for axial manifestations.7–9 For a long time, the only effective pharmacological treatment options for AS have been non-steroidal anti-inflammatory drugs (NSAIDs), improving clinical symptoms in 70–80% of treated patients.10 ,11 Consequently, NSAIDs are still recommended as the first choice of treatment.12 ,13 With the introduction of tumour necrosis factor inhibitors (TNFi), new treatment options have become available and, meanwhile, they are recommended to be applied after non-response or unsatisfactory response to NSAIDs.12 ,14 We have analysed how drug treatment has changed over the past decade and how recommendations for the management of AS are reflected in routine rheumatological care in Germany. This is complemented by the evaluation of outcome assessments, healthcare utilisation and employment situation.
Methods
The national database of the German Collaborative Arthritis Centres is an ongoing prospective study established in 1993 as a long-term monitoring system for German rheumatology.15–17 It contains annually updated clinical data and patient-reported outcomes for unselected outpatients with inflammatory rheumatic diseases. The database received study approval from the ethics committee of the Charité—University Medicine Berlin (EA1/196/06).
Patients with an International Classification of Diseases Tenth Edition (ICD10) diagnosis of M45.xx ‘ankylosing spondylitis’ or M08.1x ‘juvenile ankylosing spondylitis’ were selected for analysis. Patients with provisional diagnoses according to the judgement of the treating rheumatologist were excluded. In the current study, data of the years 2000 to 2012 from those rheumatological units that had participated in the database over the entire time interval were used to avoid bias due to changing case mix and practice variation. Cross-sectional data from 11 years were compared with regard to medical therapy, clinical presentation and quality of life indicators. Owing to a changeover from paper-based to IT-based data collection accompanied by transition difficulties in the participating units, data from 2005 and 2006 are lacking sufficient completeness, are consequently not representative and therefore not shown. For illustration purposes in figures, values for these years were replaced by sliding average of the preceding and consecutive year.
The national database comprises physician-derived information, such as onset of symptoms, diagnosis according to the modified New York criteria,18 current treatment, Steinbrocker's functional class,19 physician's assessment of activity of the disease on a numerical rating scale (NRS) from 0 to 10, and physician's assessment of disease severity on a 5-point Likert scale (asymptomatic, mild, moderate, severe and very severe). The term TNFi includes etanercept and infliximab as study drugs from 2000 to 2002, and comprises all biological agents licensed for the treatment of AS in Europe from 2003 onwards.
The patients assessed quality of life indicators such as pain and health status on NRS from 0 (best) to 10 (worst status), employment situation (including sick leave due to rheumatic disease over the past 12 months), hospitalisation due to rheumatic disease and functional status. The latter was assessed with the Hannover Functional Status Questionnaire (FFbH), which is widely used in Germany. The 18-item version of the FFbH is highly correlated with the Health Assessment Questionnaire (HAQ).20 FFbH scores range from 0 to 100 to indicate the percentage of full functional capability. We calculated the shortened 12-item version of the FFbH, which is recommended for the assessment of axial disability.21
In order to estimate the impact of AS on the employment situation, we compared employment rates of patients with AS in our database to data from the general population by calculating employment rate ratios with population rates as denominator for men and women in different age groups,22 taking into account the age and sex distribution of patients with AS.
To test for time trends, simple trend tests based on mean square successive differences were performed,23 omitting adjustments for multiple testing; p values <0.05 were considered significant. IBM SPSS Statistics V.19.0 was used for data analysis.
Results
Between 2000 and 2012, the numbers of AS patients eligible for analysis ranged between 907 in 2000 and 1175 in 2012 (table 1, see online supplement S1). Patient data were documented in hospital tertiary care centres (56%) or in private rheumatological practices (44%). Since we excluded patients with provisional diagnosis, only about 9% per year were first-time referrals. Across the years, on average 63% of the patients were male and the mean age was 49 years. Mean disease duration was 15 years with an increase of 3 years during the observed period. Based on patients with first contact with a rheumatologist in the respective years, the mean disease duration at the first visit to a rheumatologist was 7.4 years in 2000 and 4.5 years in 2011 (with an as yet insufficient case number in 2012 for evaluation).
Patient characteristics
Drug treatment
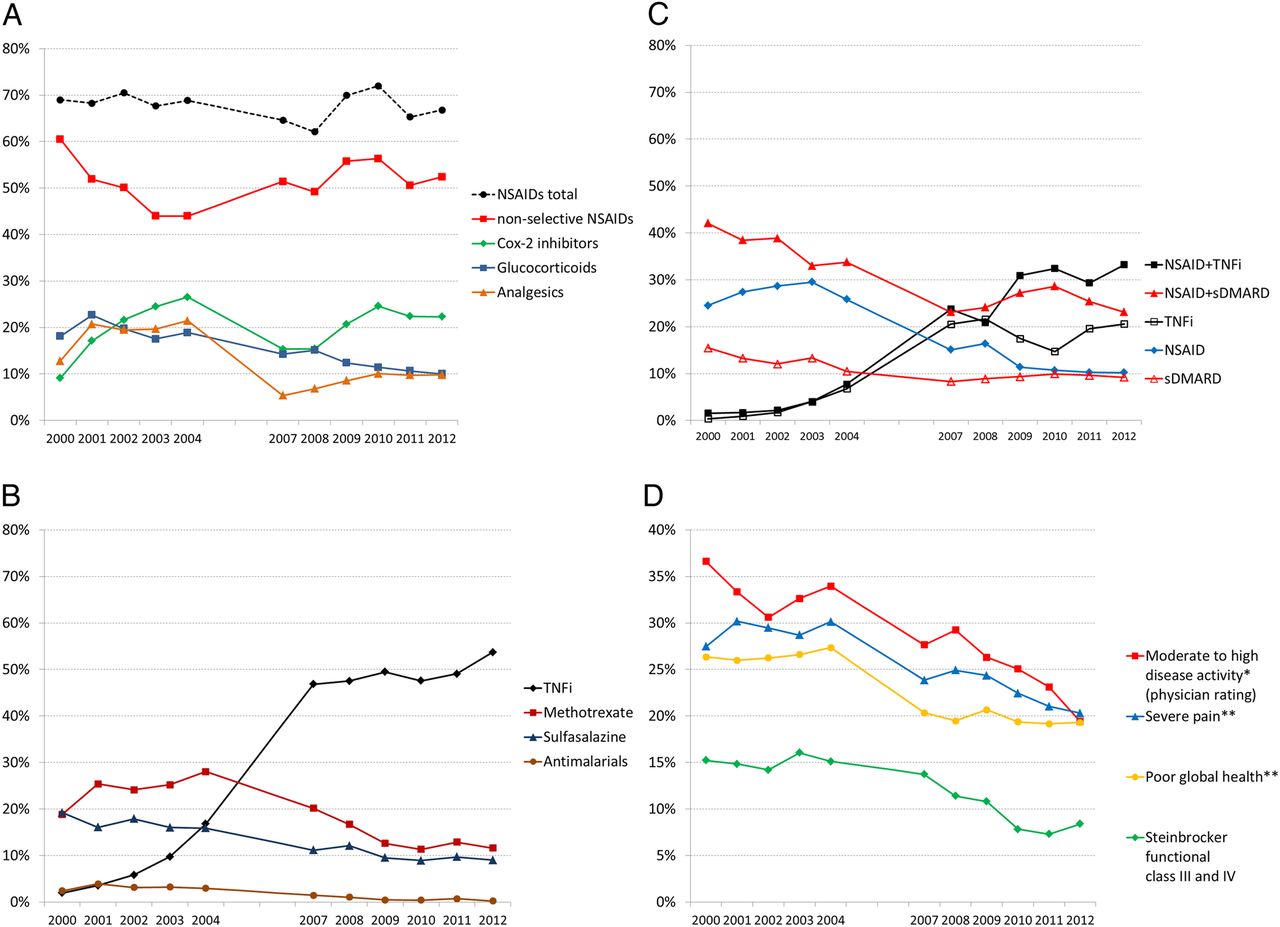
Figure 1 shows the development of the pharmacological treatment of patients with AS in routine care. As the first choice therapy, NSAIDs were prescribed to 69% of patients in 2000 and to 67% of patients in 2012 (figure 1A). In particular, the rate of non-selective NSAIDs declined by 17% until 2004 (p<0.01) with a concurrent rise in the use of cox-2 inhibitors by 18% (p<0.01). In 2012, 52% of patients received non-selective NSAIDs and 22% of patients received coxibs. The prescription rates of glucocorticoids decreased from 18% (2000) to 10% (2012) (p<0.001). The proportion of patients who received higher doses of glucocorticoids (>7.5 mg/d) receded from 3.1% to 1.8%. Analgaesics were used in 5–21% of the patients across the years.
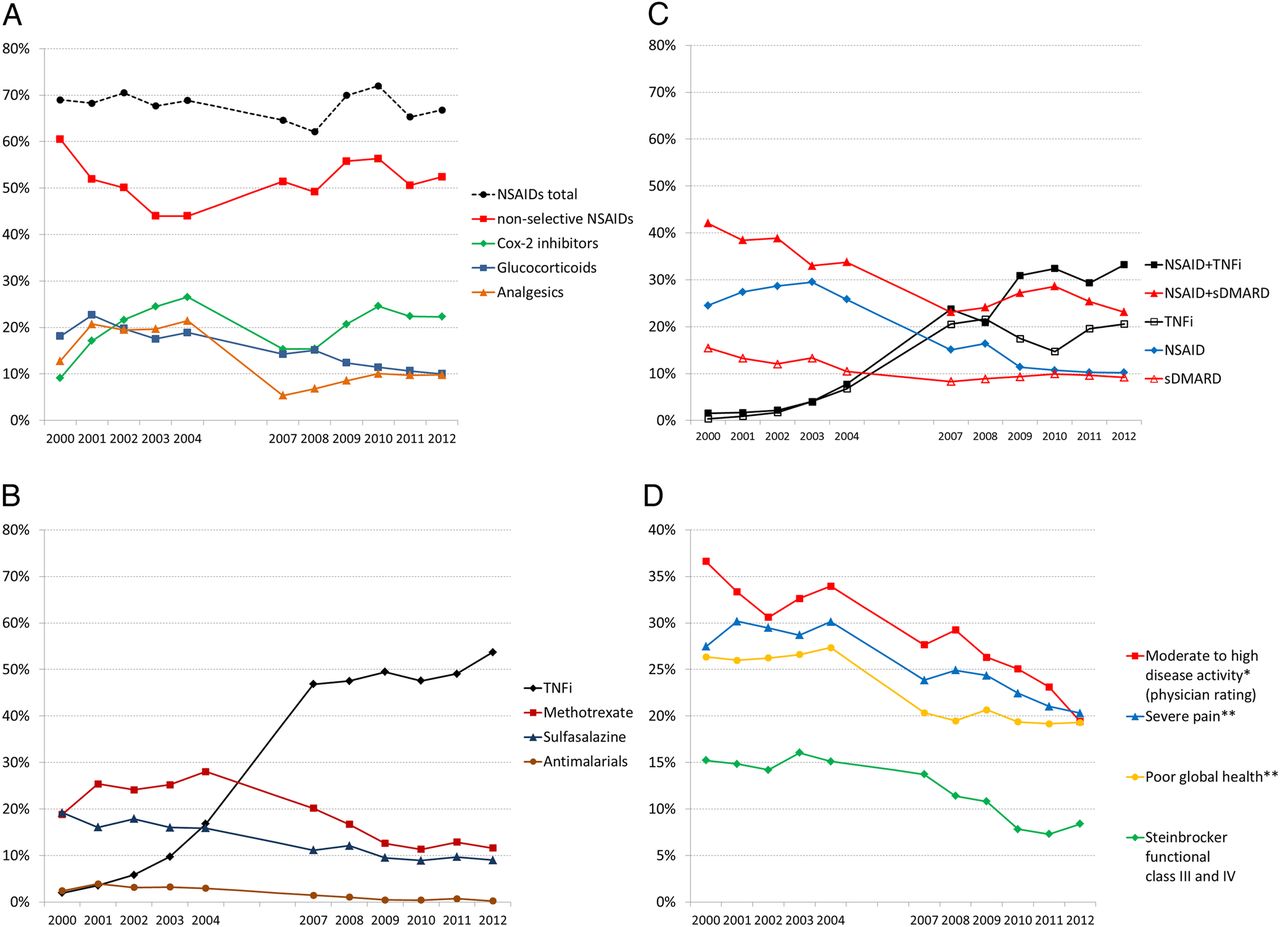
Prescription rates of (A) NSAIDs, glucocorticoids and analgaesics, (B) TNF inhibitors and synthetic DMARDs and (C) combination therapy of NSAIDs with TNF inhibitors, NSAIDs with synthetic DMARDs, or monotherapies with NSAIDs, TNF inhibitors or synthetic DMARDS, respectively. (D) Proportions of poorly rated physician-reported and patient-reported outcomes (scores *4–10 or **7–10 on a numerical rating scale with range 0–10). NSAID, non-steroidal anti-inflammatory drug; TNFi, tumour necrosis factor inhibitor; sDMARD, synthetic disease-modifying antirheumatic drug.
Since the approval of TNFi for the treatment of AS in 2003, the prescription rates continuously increased to 47% in 2007 and stabilised from 2007 onwards at around 50% of patients (figure 1B). The prescription rates of office-based rheumatologists were slightly lower (43% in 2012) than of hospital outpatient clinics (60%). The use of methotrexate increased from 2000 until 2004 (19% to 28%) and then declined to 12% since 2011. The use of sulfasalazine also decreased from 19% (2000) to about 9% since 2009. Antimalarials were used in 4% in 2001 and nearly disappeared as a therapeutic choice since 2009. All these trends are significant (p<0.001).
Figure 1C illustrates the prescription rates of TNFi, sDMARDs and NSAIDs including coxibs alone or in combination. NSAIDs have been applied increasingly in combination with TNFi, in particular from 2008 onwards with a maximum rate of 33% in 2012. The rate of TNFi monotherapy increased to 21% in 2012. Concomitant treatment with sDMARDs and NSAIDs declined from 42% (2000) to 23% (2007). The frequency of NSAID monotherapy was 30% in 2003 and then continuously declined to 10% since 2010. Monotherapy with sDMARDs decreased from 16% in 2000 to 9% since 2007. All these trends are significant (p<0.001).
Disease activity and patient-reported outcomes
The proportion of patients whose disease activity was rated moderate or high (4–10 on a NRS 0–10) by the treating rheumatologist decreased from 37% in 2000 to 19% in 2012 (p<0.001, figure 1D). Disability also declined from 15% of patients classified as Steinbrocker functional class III or IV in 2000 to 8% in 2010 (p<0.001). Patient-reported assessments of global health and pain improved continuously (p<0.001). In particular, the percentages of patients with impaired health status (7–10 on a NRS 0–10) declined from 26% to 19% and of those with severe pain (7–10 on a NRS 0–10) decreased from 28% to 20% between 2000 and 2012. The portion of patients with good functional status (FFbH12>75, corresponding to HAQ<1) increased from 36% in 2000 to 49% in 2012 (table 2).
Patient status and resource utilisation: function, early retirement, sick leave and hospitalisation
Employment
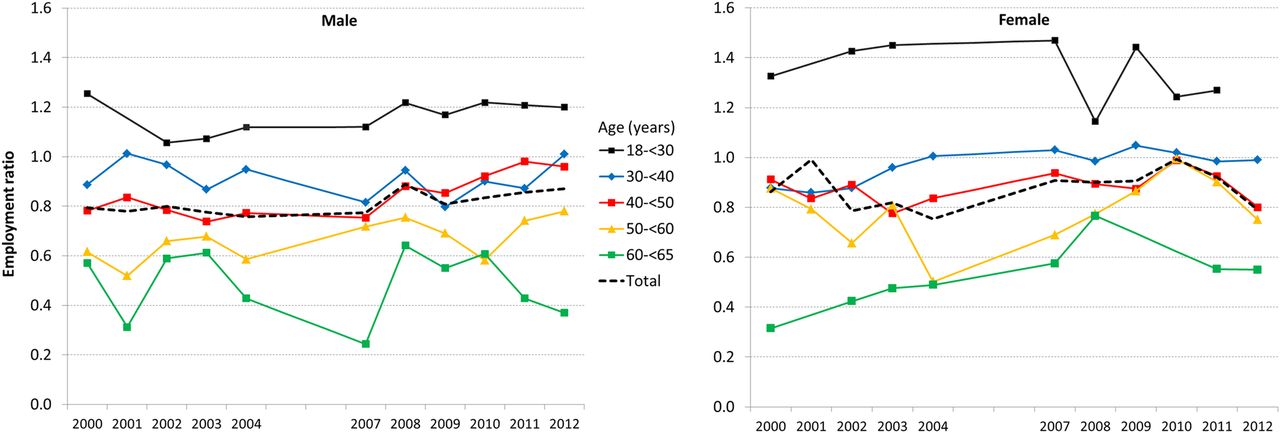
Fifty-three per cent of the patients aged 18–64 years were employed in 2000 and 65% in 2012 (data not shown). At the same time, early retirement among those <65 years of age declined from 19% to 14%, predominantly in men (21% to 12%, table 2). The proportion of gainfully employed patients increased slightly in women (from 51% to 56%) but significantly in men (54% to 71%). Moreover, a substantial increase was seen in patients aged 41–50 (+16%) and in those aged 51–60 (+17%). Slightly higher employment rates were also seen in the age-group ≤40 years (+7%) and in patients aged ≥60 (+6%). Accounting for a coincidental increase of employment rates in the general population, we calculated employment rate ratios: in women with AS aged 30–60 years, employment rates in the three 10-year age groups were lower in 2000 (rate ratio 0.88–0.91) and approximated the population rate in later years (2011: rate ratio 0.90–0.98) but receded in 2012 (figure 2). A similar tendency was also seen for women aged ≥60 with a low ratio of 0.31 in 2000 improving to 0.55 in 2012. For male patients with AS aged 50–60, the ratio increased from 0.62 in 2000 to 0.78 in 2012. In male patients aged 30–50, the ratios of 0.78 and 0.89 in 2000 improved to 0.96 and 1.01 in 2012.

{kind=link}
{kind=link}
Development of the employment rate ratio relative to the general population by sex and age groups; weighted trend over all age groups is shown as a dashed line. For illustration, in years with case numbers ≤20 calculated values were replaced with moving averages and identification marks were omitted.
Sick leave and hospitalisation
The proportion of employed patients with at least one episode of sick leave due to AS within 12 months declined from 44% (2000) to 29% (2012). This was accompanied by a reduced mean number of days on sick leave per year from 70 to 60 days in patients with episodes of sick leave. Taking all employed patients as a denominator, the days on sick leave per person declined from 21.4 (2000) to 10.4 (2012).
While the annual incidence of inpatient treatment remained stable with about 10–12% of all patients across the years, the annual cumulative duration of hospitalisation decreased from 22 days in 2000 to 16 days in 2012. This trend accounts for a decline in per capita annual hospital days from 2.3 to 1.4 days for all patients.
Discussion
In the past century, pharmacotherapeutic options for patients with AS were limited to NSAIDs and sDMARDs, with the latter having no proven efficacy on the clinical manifestation of axial inflammation.12 ,24 The introduction of biological therapies enlarged the pharmacotherapeutic armamentum, with strong evidence for clinical and functional efficacy of TNFi in patients with AS.12 ,25 While these treatments have successively entered routine care during the past decade, real-life data describing trends in drug treatment and clinical outcomes in patients with AS are scarce. Our national database enables us to investigate large samples of patients with AS for over more than a decade, enrolled annually by a stable setting of rheumatological hospital outpatient centres and private practices in Germany. We observed that the proportion of patients with AS treated with TNFi increased to more than 50%. This reflects that in Germany, while patients with AS in the population are mainly treated by general practitioners or orthopaedic surgeons, those with the most severe disease are referred to rheumatologists, often because of the indication for biological treatment. It has to be noted that patients with AS in the national database were reported in almost equal shares by tertiary care centres and private practices, while specialised care in rheumatology was about 75% practice-based.26 Considering the TNFi prescription rates of 43% in private practices and of 60% in tertiary care centres in 2012—reflecting the more severely ill patients in tertiary hospital centres—the adjusted estimate of total prescription rates of TNFi to patients with AS in German rheumatology would be 47%. Extrapolation from these numbers to the total prescription rates of TNFi for AS in Germany is not possible since data are lacking on the proportion of patients in the population treated by rheumatologists. In any case, the prescription rate for AS in the population will be far lower. In parallel with the increase in TNFi prescription, the use of sDMARDs and glucocorticoids decreased. In accordance with the current ASAS/EULAR recommendations on the management of AS,12 ,27 NSAIDs are used as the first choice treatment, and they have been prescribed increasingly in combination with TNFi therapy.
AS leads to impaired spinal mobility which, together with pain, stiffness and fatigue, decreases patients’ ability to perform daily activities and it may severely impair quality of life.12 Longer disease duration and increasing age are associated with decreased functioning.28 Although the majority of patients in our database have longstanding AS and are aged around 50, patient-reported outcomes and physical function improved over the years. According to German statutory pension insurance data from 2000 to 2012, rehabilitation measures were reduced by one-third, most significantly in men with AS.29 Although the hospitalisation rate is stable, the mean duration of inpatient treatment decreased from 3 to 2 weeks. This decrease may be attributable to better treatment options but may also be due to changes in the reimbursement system for hospitals in Germany during this time period. Data from a randomised trial of adalimumab in patients with AS revealed that improvements in quality of life and the physical consequences associated with AS have a direct relationship with a patient's ability to work.30 In a literature review of studies from the 1980s and 1990s, in European cohorts with comparable disease duration but 7–9 years younger age on average, rates of disability retirement between 15% and 36% were reported.31 Since AS typically begins in early adulthood, structural spine damage, pain and disability affect the patients’ working ability and quality of life in a pervasive manner.32 In our data, despite increasing disease duration, early retirement rates decreased from 19% to 14%, and in male patients down to 12%. A current analysis of German health insurance data shows a stronger decrease in the incidence of work disability pensions because of AS rather than because of all non-rheumatic diseases.33 A positive impact on all work-related outcomes was seen for treatment with biologics in AS in a recent systematic review, yet statistical significance was not met, most likely due to methodological limitations.34 Improved working ability is also suggested in our data by the continuous trend across most age groups, approaching employment rates of the general population. Sick leave rates among employed patients decreased by 15%, accompanied by a notable reduction of the duration of sick leave episodes.
The study has a number of limitations. First, with regard to disease outcomes, our analyses were limited to global physician and patient assessments since no information on structural damage is collected in the framework of the national database. We did not show changes in AS-specific indices such as BASMI, BASDAI or BASFI, since they were introduced in the national database in 2007 only and, therefore, are not available for the entire period of interest. Second, it is not possible to transfer our results to the general population with AS in Germany. Patients with AS are typically referred to a rheumatologist by their general practitioner or orthopaedic surgeon if standard care is not sufficient and changes in treatment, including biological therapy, are necessary. In addition, we may have underestimated the overall improvements over time since patients with good treatment response are less likely to return to the rheumatologist.
On the other hand, despite these limitations, we were able to demonstrate that routine rheumatological care of patients with AS has changed tremendously during the past decade, mainly driven by the introduction of TNF inhibitors. At the same time, disease control and patient-reported outcomes remarkably improved, also reflected in reduced healthcare utilisation and increasing participation in the labour market.
Acknowledgments
The authors acknowledge the invaluable contributions and the enthusiasm of all German consultant rheumatologists who contributed data of their patients with inflammatory rheumatic diseases to the National Database since 1993. In particular, the authors would like to acknowledge the significant contributions of R Alten (Berlin), M Aringer (Dresden), M Backhaus (Berlin), H Burkhardt (Frankfurt/Main), R de la Camp (Erlangen), T Eidner (Jena), K Fischer (Greifswald), U von Hinüber (Hildesheim), G Hoese (Stadthagen), I Kötter/J Henes (Tübingen), U Müller-Ladner (Bad Nauheim), W Ochs (Bayreuth), S Späthling-Mestekemper (München) and J Richter (Düsseldorf).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Funding The National Database was funded by the Federal Minister of Research from 1999 to 2007 [01GI0344/3]. Since 2007, the Database has been funded through unconditional grants from the German Collaborative Arthritis Centres and from a consortium of 11 pharmaceutical companies to the German Academy for Continuing Medical Education in Rheumatology.
Contributors DH, KT, MR, KCA, SB and AZ conception and design, analysis and interpretation of data. AK, KK and SW took part in acquisition of data. DH, KT, KCA and AZ took part in drafting the article. MR, AK, KK, SW and SB took part in revising it critically for important intellectual content. DH, KT, MR, KCA, SB, AK, KK, SW and AZ took part in final approval of the version to be published.
Competing interests None declared.
Patient consent Obtained.
Ethics approval The national database received study approval from the ethics committee of the Charité—University Medicine Berlin (EA1/196/06).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The national database, established in 1993, collects annually updated clinical and patient-derived data from patients with different inflammatory rheumatic diseases. The data from the national database are solely available to researchers from the German Rheumatism Research Centre, Epidemiology unit, and their clinical collaborators.