Article Text

Abstract
Objective To measure and value the impact of combined etanercept (ETN) and methotrexate (MTX) therapy on work productivity in patients with early rheumatoid arthritis (RA) over 52 weeks.
Methods MTX- and biological-naïve patients with RA (symptom onset ≤12 months; Disease Activity Score based on a 28-joint count (DAS28) >3.2) received open-label ETN50/MTX for 52 weeks. The Valuation of Lost Productivity (VOLP) questionnaire, measuring paid and unpaid work productivity impacts, was completed approximately every 13 weeks. Bootstrapping methods were used to test changes in VOLP outcomes over time. One-year productivity impacts were compared between responders (DAS28 ≤3.2) at week 13 and non-responders using zero-inflated models for time loss and two-part models for total costs of lost productivity.
Results 196 patients were employed at baseline and had ≥1 follow-up with VOLP. Compared with baseline, at week 52, patients gained 33.4 h per 3 months in paid work and 4.2 h per week in unpaid work. Total monetary productivity gains were €1322 per 3 months. Over the 1-year period, responders gained paid (231 h) and unpaid work loss (122 h) compared with non-responders, which amounted to a gain of €3670 for responders.
Conclusions This is the first clinical trial to measure and value the impact of biological treatment on all the labour input components that affect overall productivity. Combination therapy with ETN50/MTX was associated with a significant productivity gain for patients with early RA who were still observed at week 52. Over the 1-year treatment period, responders at week 13 suffered significantly less productivity loss than non-responders suggesting this gain was related to treatment response.
Trial registration number ClinicalTrials.gov number NCT00913458
- Economic Evaluations
- Early Rheumatoid Arthritis
- DMARDs (biologic)
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Rheumatoid arthritis (RA) has a substantial effect on work productivity in the very early phase of the disease.
What does this study add?
This study measures how much productivity patients with early RA gain when on combination therapy with etanercept and methotrexate.
How might this impact on clinical practice?
The combination therapy is associated with a significant productivity gain for patients who remained on treatment at week 52.
Over a 1-year treatment period, early responders at week 13 had significant productivity gains compared with non-responders, which suggests this gain is related to treatment response.
Introduction
Rheumatoid arthritis (RA) is a systemic inflammatory disorder with an annual incidence of 3/10 000 adults.1 It has been demonstrated that RA has a substantial effect on work productivity and the effect can occur at the very early phase of the disease. Using a multinational database, Sokka et al2 found among 1756 patients whose symptoms had begun during the 2000s and who were working, 20% of them had stopped working at 2 years and 32% at 5 years. Furthermore, patients with recent-onset RA who are still in paid-employment often take sick leave. Merkesdal et al3 reported an average of 82 days of sick leave per person-year within the first 3 years of RA. The ability to work is one of the most valued areas for patients with RA.4 Developing effective treatments and strategies to improve patient work productivity in patients with early RA is therefore an important priority.
Recently, clinical trials have demonstrated that initial aggressive treatment of RA with a combination of disease-modifying antirheumatic drugs (DMARDs) or early intervention with a combination of biological therapy with methotrexate (MTX) can reduce duration of sick leave and RA-related work disability.5–7 However, these studies focused on measuring job loss and absent workdays, which provides only partial evidence of the effect of early intervention on overall productivity.
According to economic theory, production or output, is typically determined by three factors: capital input, labour input and technology.8 Thus, productivity loss due to health problems is the output loss due to reduced labour input attributable to poor health. Productivity loss is typically measured according to time loss, that is, the time a person is not at a job (job loss/stopping work), absent from work (absenteeism), not working while at work (presenteeism), or unable to do unpaid work due to poor health. Productivity loss is then monetised into productivity costs by multiplying time loss by the wage rate and a multiplier that adjusts the wage rate to account for actual output loss due to reduced labour input.8 ,9
The objective of this study was to comprehensively evaluate the impact of open-label treatment with a combination of etanercept (ETN) and MTX on work productivity in patients with early active RA over 52 weeks. To the best of our knowledge, no studies have measured the impact when considering all the different types of labour input components that affect productivity and the corresponding monetary value among patients with early RA.7 ,10 Thus, although it is well known that the short-term and long-term work disability are reduced in patients with early active RA receiving early intervention,11–13 it is still unknown how much exactly overall productivity gains accrue to these patients.
Methods
Study design
This study is based on phase 1 data from the PRIZE trial. The trial design included a three-phase study to evaluate the efficacy of combined ETN and MTX therapy in patients with early RA (phase 1) and to assess whether efficacy (remission) can be maintained with ETN dose reduction or biological-free (phase 2) or drug-free (phase 3).14 ,15 The participants had symptom (swollen joints) onset ≤12 months from enrolment and active disease as indicated by a Disease Activity Score based on a 28-joint count (DAS28) >3.2. Phase 1 was a 52-week open-label, single-arm period in which all participants were treated with ETN50 mg once weekly plus MTX. Participants who were not in sustained remission or who did not have low disease activity (DAS28 >3.2) at the week 39 visit were withdrawn from the study and treated in accordance with local clinical practice.
Valuation of Lost Productivity (VOLP) questionnaire and outcomes
The Valuation of Lost Productivity (VOLP) questionnaire measures all the time input loss components (absenteeism, presenteeism, employment status changes, and unpaid work productivity loss) as well as information on job and workplace characteristics, based on which wage multipliers can be calculated to value the productivity loss attributable to reduced time input of workers.9 The VOLP has been validated in patients with RA.16
In this study, the VOLP was measured approximately every 13 weeks. The main VOLP outcomes of interest at each administration were (1) paid work productivity loss (hours) in the past 3 months, the sum of hour loss from absenteeism, presenteeism and employment status changes; (2) unpaid work productivity loss (hours) in the past 7 days, quantified by the number of hours of getting help on unpaid work activities; (3) total costs of lost productivity in the past 3 months, the sum of the costs of paid and unpaid work productivity loss.
The main VOLP outcomes of interest during the 1-year study period were (4) paid work productivity loss (hours); (5) unpaid work productivity loss (hours); (6) total costs of lost productivity. These three outcomes were the sum of the corresponding outcomes at weeks 13, 26, 39 and 52. The Last Observation Carried Forward (LOCF) method was applied for any missing follow-up to calculate these outcomes. The main concern for this study is those patients who would be withdrawn from the trial if they did not achieve DAS28 ≤3.2 at week 39. The LOCF method underlies the assumption that these patients would not get the treatment and thus remain the same productivity level. As a sensitivity analysis, the missing data were also replaced by multiple imputations using the fully conditional specification method (the MI procedure in SAS 9.4, SAS Institute, Cary, North Carolina, USA).17 The details on the outcome definitions and multiple imputation method can be found in the online supplementary appendix.
Costing of productivity loss
Since this trial was conducted in multiple countries, we cost the paid work loss by converting the patients self-reported income into Euros in 2010 using Purchasing Price Parties obtained from World Bank.18 For unpaid work productivity loss, we used the 2010 hourly earnings (Euro) reported by the Eurostat for service and sales workers in each country.19 The VOLP enables the calculation of wage multipliers for absenteeism and presenteeism based on the workplace characteristics (team work status, availability of substitutes and their substitutability).9 Costs incorporating these multipliers represent productivity loss instead of wage loss and were calculated as ‘lost time×wage×multiplier’. Costs with multipliers are presented in the paper, while costs without multipliers are in the online supplementary appendix.
Productivity loss versus productivity gain
Productivity loss is an outcome that is calculated at each time point and cumulatively at 1 year. A productivity gain is defined when comparing outcomes between time-points and different groups. For example, when productivity loss at each time point decreased compared with baseline, the change in loss was defined as productivity gain over time. Moreover, when comparing productivity loss between responders and non-responders, if responders had reduced productivity loss in comparison to non-responders, this is referred to as a gain in productivity for responders.
Analyses
Our analysis focused on the participants who were employed at baseline and who had ≥1 follow-up with VOLP (weeks 13, 26, 39 and 52). The main VOLP outcomes of interest at week 52 were compared to those at baseline to assess the productivity gained in patients receiving the combination therapy. Since the protocol allowed some patients to discontinue at week 39, we also compared the VOLP outcomes at week 39 to those at baseline. For categorical variables, McNemar's test was used to examine percentage changes while the paired t test was used for the comparison of continuous variables. Since the continuous VOLP outcomes were highly skewed with inflated zeros, bootstrapping methods were used to test hypotheses.20–22
Patients were categorised into two groups, early responders versus non-responders, according to their disease activity at week 13 (DAS28 ≤3.2 vs DAS28 >3.2). Bootstrapping t test was used to test for differences in VOLP outcomes over 1 year across groups. Our analytical objective was to measure the association of early response status with 1 year productivity loss. To ensure an unbiased coefficient of response status variable, we also adjusted for potential confounders and the unbalanced characteristics between responders and non-responders at baseline. Based on previous review papers on the predictors/variables related to work disability in RA,23 ,24 there was evidence showing sociodemographic variables, clinical variables and work-related factors were associated with work disability in RA. However, to avoid overadjustment and address the issue that some variables might be highly correlated (multicollinearity), we did not include all variables we measured at baseline in the final model. Details of the variable selection method can be found in the online supplementary appendix.
Since many patients had no productivity loss, we used zero-inflated negative binomial models (ZINB) to compare paid and unpaid work productivity loss (hours) during 1 year. For 1 year total costs of lost productivity, a two-part model (logistic regression for the probability of no costs and generalised linear model with γ distribution and log link for nonzero costs) was performed for the comparison.
Furthermore, to improve the interpretation of the coefficients of the ZINB and two-part models, we first computed the expected values for responders and non-responders, respectively, while holding the model covariates at their mean value. Then, we computed the difference in expected values between responders and non-responders, which we refer to as the marginal effects. Bootstrapping methodology was used to calculate the CIs.
Results
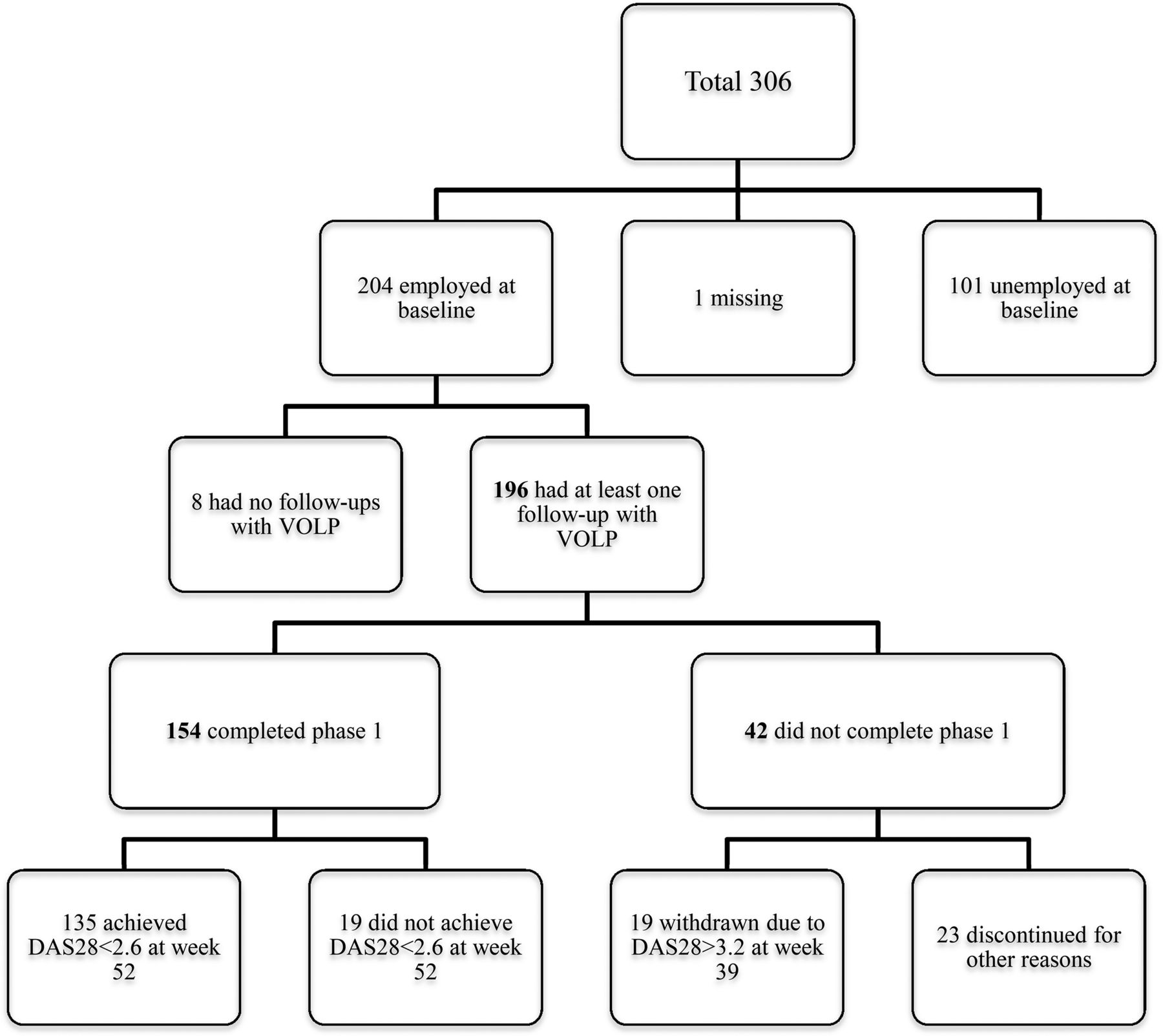
Among the total of 306 patients participating in phase 1, 204 reported they were employed at baseline, 101 were unemployed and 1 patient's employment status was missing (figure 1). 196 employed patients who had ≥1 follow-up with VOLP were included in our final analysis. Among them, 154 completed the phase 1 and 42 did not, including 19 patients who were withdrawn due to not achieving low disease activity at week 39 and 23 patients who discontinued for reasons including adverse events, participant request, investigator judgment, protocol violation or sponsor's decision.
Average age of study participants was 46 years and 68% were women (table 1). About 62% were working full time and 11% did heavy work or carried very heavy loads. Average working time was 36.01 h or 4.87 days per week. The estimated wage multipliers implied that the productivity loss was 1.58 or 1.55 times more than the wage loss due to absenteeism and presenteeism, respectively. For example, a productivity loss due to a 1 h absence from work would be calculated to be 1.58 times the hourly wage of the patient.
Baseline patient characteristics
Table 2 presents descriptive statistics of VOLP outcomes by visits. The bolded row shows the numbers of non-missing values used to generate the statistics for each outcome. Decreasing numbers of non-missing values were partially due to the missing responses and partially due to discontinuation. A small percentage of patients changed their employment status, for example, stopped working, due to their poor health. The percentage of patients who stopped work due to their health became smaller over the follow-ups and there were also a few patients who restarted working after their initial work stoppage. At baseline, about 58% of patients reported being absent from work over the past 3 months. On average, the absent hours were 75.7 h, which accounted for 17% of their usual working time. About 39% of patients reported that they would complete the same work in less time if they did not experience any health problems. The percentage of time loss while working due to health in the past 7 days was 8%.
The descriptive statistics of VOLP outcomes by visits
Both absenteeism and presenteeism showed a declining trend over the 52-week follow-up. Overall, paid work loss was 111.7 h over the past 3 months at baseline, accounting for 25% of usual working time, and decreased to 60.1 h at week 52, which accounted for 13% of usual working time. Similarly, unpaid work loss was 6.3 h per week at baseline and declined to 1.8 h per week at week 52. Total costs of lost productivity over the past 3 months were €3483 at baseline and €843 at week 52. The reductions in these outcomes imply significant gains in paid and unpaid work productivity at week 52 (table 3). Patients gained 33.4 h per 3 months in paid work and 4.2 h per week in unpaid work. The total monetary gains in paid work and unpaid work were about €1322 per 3 months. Significant paid and unpaid work productivity gains were also observed at week 39.
Change of productivity loss from baseline to week 39/52
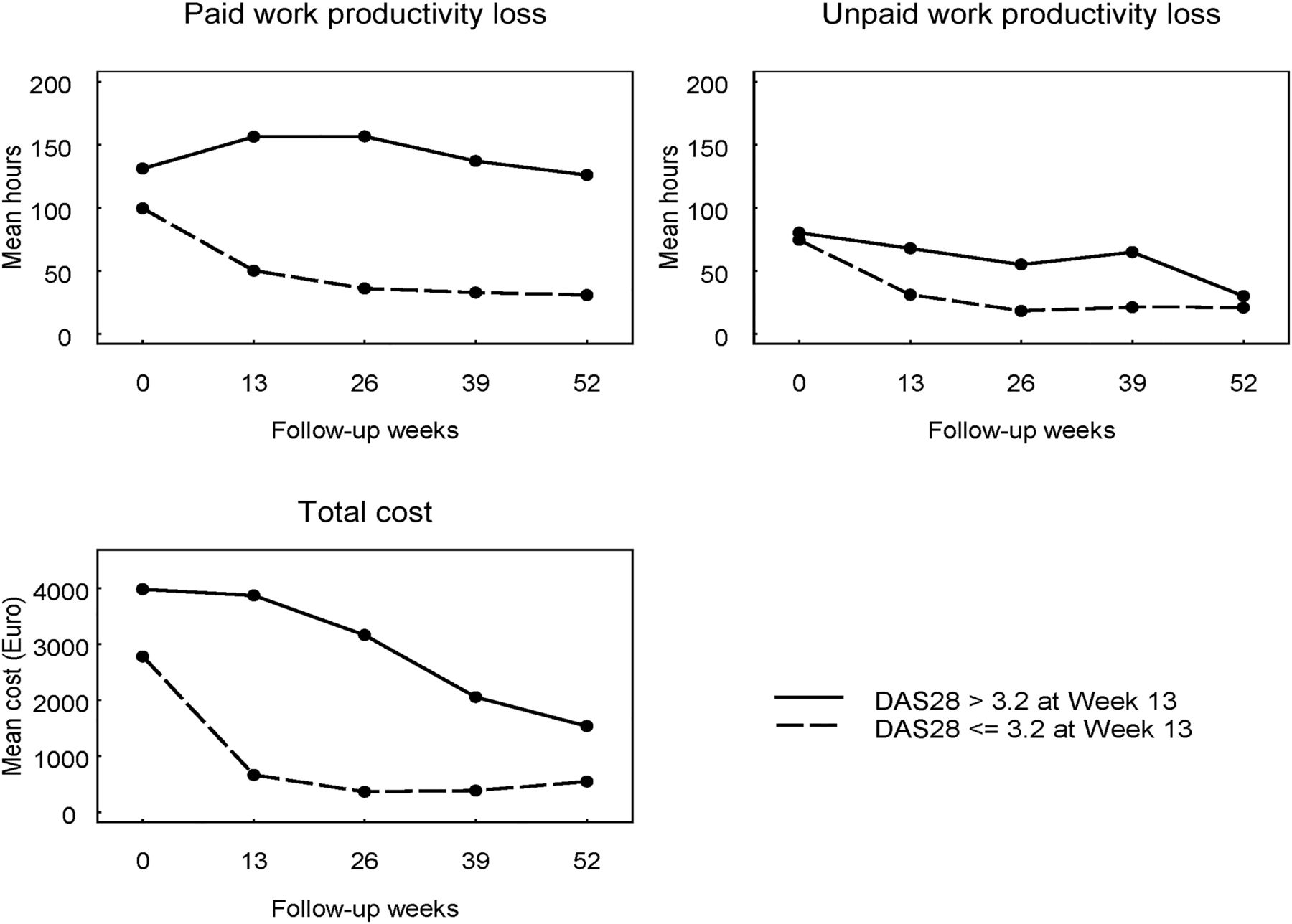
A total of 115 patients (60.5%) were responders at week 13 and 75 patients were non-responders. We could not categorise six patients into responders or non-responders due to the missing DAS28 data at week 13. Productivity loss for responders and non-responders is clearly shown in figure 2. For responders, each outcome dropped at week 13 and subsequently flattened. For non-responders the outcomes dropped only slightly or even increased (eg, paid work productivity loss) at week 13 and subsequently dropped relatively sharply. This seems to correspond to the progress of disease activity of non-responders. This might be explained by that disease activity of non-responders at week 13 might be improving after week 13, and that those with high disease activity at week 39 withdrew from the study.
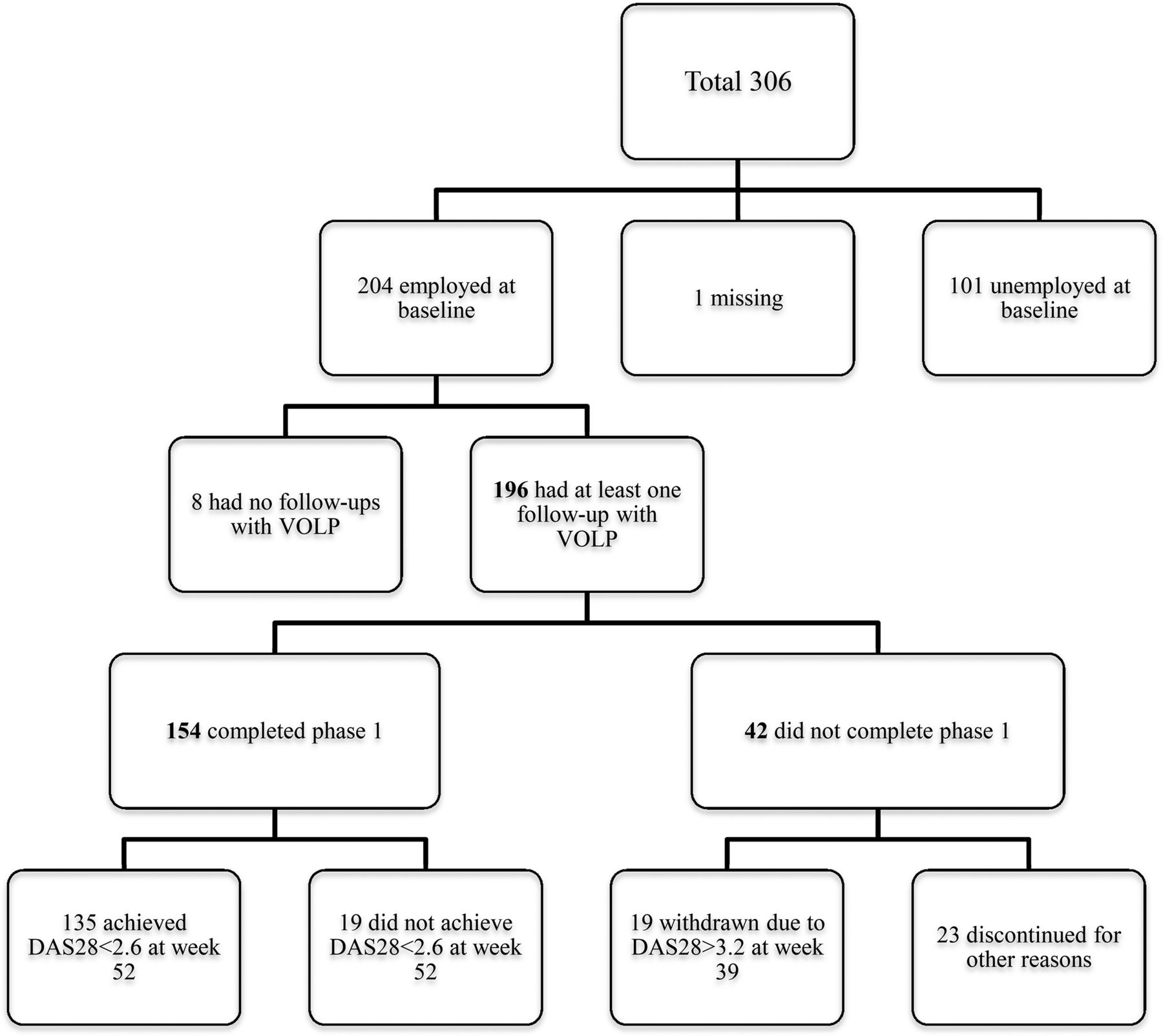
Study cohort flowchart. DAS28, Disease Activity Score based on a 28-joint count; VOLP, the Valuation Of Lost Productivity questionnaire.
In terms of VOLP outcomes during the 1-year study period, overall, paid work productivity loss was 295 h (about 17% of usual working time), unpaid work productivity loss was 162 h, and the total costs were €5223 (table 4). Paid and unpaid work productivity losses for responders (155 and 93 h, respectively) were significantly lower than that for non-responders (522 and 254 h). Total costs of lost productivity for responders (€1993) were significantly smaller than those for non-responders (€10 676).
Total productivity loss during the 1-year study period by response at week 13
Table 5 presents marginal effects from models comparing 1 year productivity loss between responders and non-responders (see online supplementary appendix). For 1 year paid work productivity loss, while holding covariates at their mean value at baseline, the expected probability of being zero loss was 44% for responders and 27% for non-responders; the expected paid work hour loss in part 2 of the ZINB model was 266 h and 519 h, respectively; overall, the expected paid work productivity loss was 149 h and 380 h, respectively, with a 231 h significant difference. Similarly, the difference in unpaid work productivity loss was significant and equalled 122 h. For total costs of lost productivity, responders had a 32% higher probability of having no costs than non-responders. Overall, responders gained €3670 in productivity compared with non-responders. In the main analysis, we applied the LOCF method to impute the missing data. As a sensitivity analysis, we applied the multiple imputation method and the results were consistent (see online supplementary appendix). After multiple imputations, we found that responders gained €3847 in productivity compared with non-responders. Our results are robust to the two different missing handling methods.
Expected values by response at week 13 and marginal effects using sample means shown in table 1 from the regression models
Discussion
The PRIZE study is the first clinical trial to measure the 1-year impact of biological treatment on all the labour input components that affect overall productivity and the corresponding monetary value among people with early RA.7 ,10 This study found that paid and unpaid work productivity was significantly improved over 52 weeks. We also compared patients who responded to treatment at week 13 with those who did not to help confirm that it was the achievement of clinical response that produced these changes. For 1 year productivity loss, responders had gained 231 h from paid work and 122 h from unpaid work compared with non-responders, which amounts to an output value of €3670 gained by responders compared with non-responders.
Several previous clinical trials have examined the impact of early aggressive treatment on work productivity in terms of absenteeism among patients with early RA. The PREMIER trial assessed the effect of adalimumab+MTX on absenteeism compared with MTX monotherapy among patients with disease duration <3 years.25 ,26 The number of missed workdays due to RA in the first year was 11.1 days and 24 days, respectively.26 The COMET study measured the effect of ETN+MTX versus MTX on absenteeism among patients with disease duration <2 years and found that the 1-year missed workdays due to health were 14.2 days versus 31.9 days.6 In the study of Puolakka et al,5 patients with recent-onset RA (<2 years) were randomly assigned to receive combination therapy of DMARDs or single DMARD. During the 5-year follow-up, they found 23 days of sick leaves per patient-observation year in combination therapy group and 48 days in single therapy group. Our study population was patients with RA ≤1 year and found that the number of missed work hours due to health during 1 year was about 106.9 h, amounting to 14.5 days. Thus, the absenteeism estimates from our study were closer to those from the treatment arm in above studies even though the design, treatment, RA population and definition of absenteeism differed across studies.
Only one previous clinical trial has estimated presenteeism and unpaid work productivity loss in terms of time loss and costs.7 ,10 The PREMIER study measured presenteeism according to a visual analog scale (0–100) but did not translate it into time loss and the associated costs.25 The COMET study did not directly measure presenteeism among its study participants.6 The only study that measured and estimated the cost of absenteeism, presenteeism and unpaid work productivity loss was a substudy of CanAct trial.27 However, this study only evaluated the 12-week impact of adalimumab on work productivity and was not restricted to patients with recent-onset RA.
The main limitation of our study is its single-arm design. By looking at the change in productivity loss over 52 weeks only, we cannot determine whether the change is attributable to the treatment or the natural fluctuations of worker productivity over time especially due to regression towards the mean. Therefore, we compared 1 year productivity loss between responders and non-responders by adjusting for potential confounders. We found that treatment response was associated with a reduction in productivity loss. In this study, if the response was induced by the treatment of ETN plus MTX, then it could be inferred that the cost of ETN therapy can be viewed as being partially offset by cost savings accruing to responders. It is possible that the cost savings would apply to any treatment that induces similar clinical response. However, there might be residual confounding between non-responders and responders although we have put an effort to adjust for potential confounders. For example, in predicting total days of sick leaves and work disability, Olofsson et al28 found only 21% of the variability was explained by the included predictors. As there might be potential confounders that we did not measure and thus could not adjust for in our study, our estimate of the productivity gain of responders compared with non-responders might be subject to the confounding bias.

{kind=link}
{kind=link}
Plots of 3-month productivity loss and costs at each visit by response at week 13. DAS28, Disease Activity Score based on a 28-joint count.
In this study, based on the human-capital approach we valued productivity loss by incorporating multipliers that adjust wage to represent the actual impact of the resulting reduced labour input on productivity. As an alternative valuation method, the friction-cost method only takes account of productivity loss within a ‘friction period’ if absent workdays exceed the period.29 Productivity loss estimates could be further undervalued if the potential impact of compensation mechanisms is also considered.30 ,31 That is, no productivity loss would occur if missed work could be compensated for during normal working hours and the absent worker or colleagues who take over the work do not have to sacrifice their leisure time or take more effort to make up the lost work.8 In the literature, the choice of valuation method has been debated and there is no current consensus on appropriate methodology. It should be noted that if applying FC method and considering potential impact of compensation mechanisms in our study, the estimated costs of productivity loss would be smaller.
Our results suggest that patient productivity was significantly improved for those who remained on treatment at week 39 or week 52. Over the 1-year treatment, early responders at week 13 had significant productivity gains compared with non-responders, which suggests this gain was related to treatment response. Future studies should examine treatment effects on paid and unpaid work productivity comprehensively, as this appears to be an important component to improve.
Acknowledgments
WZ is a recipient of the Michael Smith Foundation for Health Research Postdoctoral Fellowship Award.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
Contributors RP and SK were involved in the study design of the clinical trial and data collection. WZ, NB, AHA, RP and SK designed this study. HS and WZ analysed the data. All the authors critically interpreted the results. WZ prepared the first version of the manuscript. All the authors reviewed the draft versions and gave their approval of the final version of the manuscript.
Funding This study was sponsored by Pfizer Inc.
Competing interests AHA and NB are members of the Scientific Staff, and WZ is a trainee, of the Arthritis Research Centre (ARC), which received financial support from Pfizer Inc. in connection with the development of this manuscript. HS is a member of Centre for Health Evaluation and Outcome Sciences (CHEOS), and CHEOS was compensated by ARC in connection with the development of this manuscript. RP and SK are employees of Pfizer. Outside the submitted work, AHA has received research funding and/or honoraria from Pfizer Inc. and AbbVie Corporation, both of whom manufacture biologics. AHA has also received payment for lectures, which include service on speakers bureaus, from International Value Coalition and AbbVie Corporation.
Ethics approval For the clinical trial, the institutional review board or ethics committee at each participating center approved the study protocol. The clinical trial was conducted in accordance with the ethical principles of the Declaration of Helsinki and the Good Clinical Practice guidelines of the International Conference on Harmonisation. This study was approved by the Behavioural Research Ethics Board of the University of British Columbia (certificate number H13-00894).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.