Article Text

Abstract
Objectives To assess and compare patient perceived quality of osteoarthritis (OA) management in primary healthcare in Denmark, Norway, Portugal and the UK.
Methods Participants consulting with clinical signs and symptoms of knee OA were identified in 30 general practices and invited to complete a cross-sectional survey including quality indicators (QI) for OA care. A QI was considered as eligible if the participant had checked ‘Yes’ or ‘No’, and as achieved if the participant had checked ‘Yes’ to the indicator. The median percentage (with IQR and range) of eligible QIs achieved by country was determined and compared in negative binominal regression analysis. Achievement of individual QIs by country was determined and compared using logistic regression analyses.
Results A total of 354 participants self-reported QI achievement. The median percentage of eligible QIs achieved (checked ‘Yes’) was 48% (IQR 28%, 64%; range 0–100%) for the total sample with relatively similar medians across three of four countries. Achievement rates on individual QIs showed a large variation ranging from 11% (referral to services for losing weight) to 67% (information about the importance of exercise) with significant differences in achievement rates between the countries.
Conclusions The results indicated a potential for improvement in OA care in all four countries, but for somewhat different aspects of OA care. By exploring these differences and comparing healthcare services, ideas may be generated on how the quality might be improved across nations. Larger studies are needed to confirm and further explore the findings.
- Osteoarthritis
- Quality Indicators
- Health services research
- Patient perspective
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known on this subject?
Clinical practice does not always reflect guideline recommendations.
What does this study add?
Patient-reported quality of care shows a large variation on different quality indicators.
The differences in achievement rates across four European countries may reflect differences in healthcare priorities.
How might this impact on clinical practice?
By exploring differences in quality of care and healthcare services, ideas for improving healthcare may be developed.
Introduction
Knee osteoarthritis (OA) is a prevalent chronic joint condition that affects the whole joint and may cause pain, stiffness and functional disability.1 Owing to the increase in the ageing population and the epidemic of obesity, the incidence of OA is increasing.2 OA is one of the leading causes of global disability3 ,4 and is expected to be the fourth leading cause of disability by the year 2020.1 Hence, the burden of OA will become a major challenge for health systems globally.1
Evidence-based recommendations have the potential to improve the quality of healthcare by promoting interventions of proven benefit and discouraging unnecessary, ineffective or harmful interventions. International and national guidelines for OA treatment, including those made by the European League Against Rheumatism (EULAR), American College of Rheumatology (ACR), Osteoarthritis Research Society International (OARSI) and the UK National Institute for Health and Care Excellence (NICE), have been available for some time.5–12 The first message that emerges from the guidelines is that there is a range of simple interventions for which there is evidence of clinical effectiveness. However, clinical practice does not always reflect these recommendations.13 ,14 Adherence to recommendations for care may be measured using process quality indicators (QI). A QI can be defined as a “measurable [element] of practice performance for which there is evidence or consensus that it can be used to assess the quality, and hence change in the quality, of care provided”.15 A limited number of QI lists for OA care have been developed.16–23
A small number of previous studies have examined the quality of OA care using QIs. The results show patient-reported achievement of OA QIs between 22% and 72%, suggesting that primary healthcare for older adults with OA is suboptimal.13 ,14 ,20 ,24–28 Although patient self-reported QI measures may have some limitations with regard to accuracy and recall bias, they provide an important perspective of the quality of OA care and mirror the care as perceived by the patient. Further, patient-reported measures can include elements of care that are less reliably captured from the medical records, for example, patient information or functional assessments. The patient perspective of OA QI attainment has so far received limited attention, and differences related to the QI items and study design make it challenging to directly compare study results. This EULAR-funded study is the first study that has applied the same set of QI items in four European countries, which allows a cross-national comparison of OA QI achievement.
This study aimed to determine the self-reported QI achievement for OA care among adults with knee OA and to compare QI achievement cross-nationally between Denmark, Norway, Portugal and the UK.
Methods
Study design
This study includes data from cross-sectional surveys in primary healthcare in four European countries: Denmark (DK), Norway (NO),29 Portugal (PT) and the UK (UK).30 Ethical approvals were granted for all four surveys (see online supplementary file 1). Research partners have been involved in designing the surveys in the four countries, and in this study in the design and writing. This paper is written in concordance with the STROBE guidelines for reporting observational studies.31
Setting and participant recruitment
In all four surveys, the participants were recruited from primary healthcare. Adults aged 45 years and over consulting their general practitioner (GP) with a knee OA diagnosis recorded in the medical records were identified between 2012 and 2014. Participants with inflammatory arthritis, malignant illness or an inability to complete the questionnaire were excluded. There were some minor differences in eligibility criteria between the four surveys, and the details are provided in online supplementary file 1. Written consent was obtained and questionnaires were completed either immediately after the GP consultation on site (DK, NO and PT) or at home (DK, NO and UK) and returned in a prepaid envelope.
The questionnaire
A set of QI items for OA care was included in all four surveys (see online supplementary file 2). In three countries (NO, DK and PT), the OsteoArthritis QI (OA-QI) questionnaire was used. The OA-QI questionnaire was developed in 2010 using published QIs, an expert panel and patient interviews.20 Acceptable validity and moderate test-retest reliability were demonstrated in a Norwegian OA cohort.20 The OA-QI questionnaire has been subject to a forward and backward translation procedure into English and Danish, and then from English into Portuguese. The OA-QI questionnaire includes 17 items with ‘Yes’, ‘No’ response options and a third option if the item was not applicable (eg, ‘Not overweight’ for items on weight management) or the participant did not remember. The UK survey applied a variation of the QI set: the patient-generated MOSAICS QI questionnaire.30 Fourteen QI items were measured consistently in all four countries and included in the main analysis (QIs numbers 4, 9 and 12 from the OA-QI were not included). Five items addressed patient education and information about disease development, treatment alternatives, self-management, weight management and physical activity. Regular provider assessments are addressed in two questions. Four questions were related to pharmacological treatment and three addressed referrals.
Age, gender and body height and weight were self-reported or measured (DK), and the body mass index (BMI) was calculated. Comorbidity was self-reported (DK, NO and PT) or obtained from a medical record review for the previous 24 months (UK). Inflammatory arthritis included ankylosing spondylitis, Sjogren's syndrome, psoriasis, psoriatic arthritis, polymyalgia rheumatica, systemic lupus erythematosus and rheumatoid arthritis. Chronic comorbidity included heart disease, lung disease, osteoporosis, cancer and diabetes. Knee function was self-reported in DK, NO and PT using the Knee injury and Osteoarthritis Outcome Score (KOOS),32 whereas the Western Ontario and McMaster Universities Arthritis Index Short Form 8-item (WOMAC SF-8)33 function scale score was used in the UK. The WOMAC function scale score can be derived from the KOOS, so the WOMAC SF-8 function scale score was calculated for all countries. The eight items include: descending stairs, ascending stairs, rising from sitting, walking on a flat surface, getting in/out of a car, shopping, putting on a sock and getting on/off the toilet. The scale score ranges from 0 to 100, with 0 indicating no functional problems. The KOOS was not initially included in the questionnaire in PT and only 30% of patients from PT had an SF-8 score determined.
Statistical analyses
QIs were considered as achieved if the participant had checked ‘Yes’ to an indicator. Responses were excluded (not eligible) from analysis for that QI if there was a missing/ambiguous response or if the participant had responded ‘Don't remember’, ‘Not overweight’, ‘No such problems’, ‘No pain/discomfort’ or ‘Not severely troubled’. Hence, the number of eligible items varied from participant to participant.
The median (with IQR and range) number of eligible QIs (ie, checked ‘Yes’ or ‘No’) and the median (IQR, range) percentage of eligible QIs achieved in each country were determined on the basis of the 14 QIs measured in all 4 countries. Further, the percentage of people having all eligible QIs achieved (checked solely ‘Yes’), and the percentage with no eligible QIs achieved (checked solely ‘No’) was determined. Differences in the number of QIs achieved between countries, using the number of eligible QIs for each person as the exposure variable, were determined using negative binomial regression, first unadjusted and then adjusted for age, gender, BMI and comorbidity. Results are reported as rate ratios (RR) and 95% CI using NO as the reference country. In sensitivity analyses, we repeated the analysis only in people from NO, DK and the UK for whom a WOMAC function scale score was available, and further adjusted for functional limitation; and then restricted the analysis to those without inflammatory arthritis comorbidity.
Achievement of each QI was compared between countries using logistic regression, again unadjusted and then adjusted for age, gender, BMI and comorbidity.
Analysis was performed using Stata/MP 13.1 for Windows.
Results
Participants
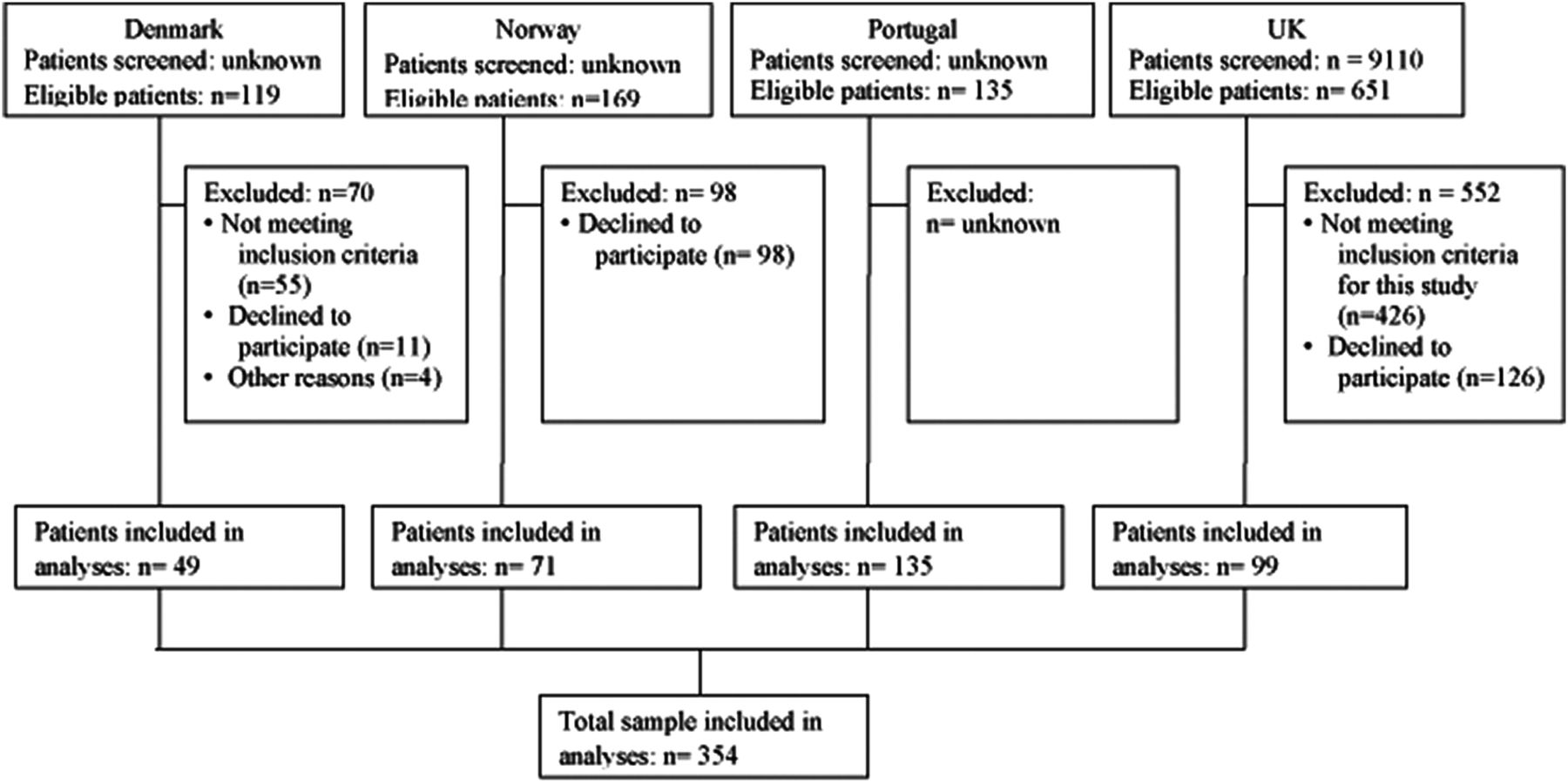
In total, 354 patients were included in the analyses (figure 1). The mean age was 67.7 years (SD 10.1), the proportion of females was 67%, and the mean BMI was 28.5 kg/m2 (SD=4.8; table 1). The WOMAC SF-8 function scale score showed better function among the subsample of the Portuguese participants and Danish participants compared with the Norwegian and UK participants. The presence of inflammatory arthritis was highest in the Danish cohort compared with the other cohorts, and the presence of a chronic disease was higher in the Danish and Portuguese cohorts. The UK had the lowest comorbidity levels, but this was based entirely on medical records rather than self-report.
Characteristics of participants
{kind=link}
Flow diagram.
Number of QIs achieved in the total sample and by country
The study participants considered most of the 14 QIs to be relevant (eg, checked ‘Yes’ or ‘No’), and the median number of eligible QIs was 12 (IQR=10–14, range 0–14). The median percentage of eligible QIs achieved (checked ‘Yes’) was 48% (IQR=28%, 64%; range 0–100%). For 5% of the total sample, none of the QIs were achieved, and for 2% all eligible QIs were achieved.
The median percentage of QIs achieved by country was relatively similar across three of the countries, but significantly lower in DK (23%; unadjusted RR compared to NO=0.54; 95% CI 0.43 to 0.68; table 2). DK still had a significantly lower level of achievement after adjustment for age, gender, BMI and comorbidity (RR=0.49; 0.39, 0.62), when further adjusted for the WOMAC function scale score (RR=0.47; 0.38, 0.59), and when restricted to those without inflammatory arthritis comorbidity (RR=0.47; 0.34, 0.66). None of the covariates were associated with the number of QIs achieved in the final models.
Number of quality indicators (QI) achieved by country*
Achievement of individual QIs in the total sample
Achievement of individual QIs ranged from 11% to 67% (table 3). QIs with the lowest percentage achievement were related to referral to services for losing weight (11%), functional assessments (appliances and aids 13%; walking aids 31%), consideration of corticosteroid joint injections (25%) and referral for evaluation for surgery (36%). QIs with the highest percentage achievement were around delivery of information about the importance of exercise (67%), information about their joint problem (55%), information about OA treatment (55%), information about anti-inflammatory (side) effects (59%), and the recommendation of paracetamol as first-line medication (59%).
Achievement of individual quality indicators (QI) for the total study sample*
Achievement of individual QIs by country
Among the four countries, the UK study showed the highest achievement rates for the information QIs around the joint problem, treatment, and managing OA, and for stronger medication and joint injection QIs (table 4). The Norwegian study had the highest achievement rates for exercise information, referral for physical activity and recommendation of paracetamol. The Portuguese study showed the highest achievement rates for advice to lose weight and referral to services for losing weight. DK had the lowest percentage achievement for 13 of the 14 QIs measured in all four countries.
Individual quality indicator achievement by country
Discussion
This study aimed to determine patient self-reported QI achievement for OA care among adults with knee OA and compare QI achievement across four European countries. The percentage of participants in the total sample who achieved the individual QIs varied widely across QIs, and the number of QIs achieved by patients revealed some differences between the countries. There were similarities and differences between the countries in relation to achievement of the individual QIs.
QIs achieved in the total sample and by country
In contrast to two previous studies, which showed that age, gender, education and severity of the OA disease were related to QI achievement,13 ,14 patient characteristics in the present study were not associated with QI achievement. The median percentage of QIs achieved for the total study sample was similar to the rates in two previous studies of patient-reported OA QI achievement rates in primary healthcare,24 ,27 ,34 higher median than in three studies14 ,20 ,28 and lower median than in one study.26 It has previously been shown that adherence to QIs in OA care was lower compared to that in gout or other chronic conditions in older adults.25 ,28 ,35 According to Grol,36 achievement rates of approximately 60–70% have been demonstrated for most chronic diseases, which is higher than the rates in this study.
Although the median percentage of QIs achieved was relatively similar for three of the countries, the median for the Danish cohort in this study was significantly lower even after adjustments for patient characteristics. Although a real difference cannot be ruled out, it might be due to a selection bias as the Danish data were extracted from baseline data among a small number of participants recruited to a randomised controlled trial of pharmacological versus exercise treatment.
Achievement of individual QIs in the total sample and by country
There was substantial variation in the achievement of individual QIs across the countries. Differences in healthcare systems (ie, access to dieticians, physiotherapists, occupational therapists and orthopaedic surgeons; or the healthcare economy and patient payment) may explain a substantial proportion of the variation in individual QI achievement rates seen in this study. The observed variation could also be related to differences in patient expectations or attitudes towards OA, and in knowledge about OA and recommended treatment. There may also be variation in the timing of when people choose to consult a healthcare professional for their OA symptoms. Hence, the patients’ disease severity and burden of disease may vary at the time of consultation.
The UK data showed the highest achievement rates among the four countries regarding information about the joint problem, treatment alternatives and self-management as compared to the other three countries. Compared to two previous UK studies,13 ,28 the achievement rates in this study were substantially greater (76% vs 30/18%). This may have been related to the recruitment procedures in the MOSAICS study where eligible participants were identified via electronic pop-up screens in general practices, which could have reminded GPs about treatment recommendations for OA and led to higher achievement rates.
The total study sample showed substantially higher achievement rates for advice to exercise compared to a Canadian study (69% vs 25%),14 and much higher referral rates to supervised exercise (physical therapy) compared to a recent Australian study (52% vs 4%).37 The Norwegian cohort had the highest achievement rates regarding advice to exercise and referrals to supervised exercise. Whether this is due to differences in the healthcare system and organisation, gross domestic product and healthcare economy, national health authority strategies, or due to differences in GPs’ knowledge or attitude towards exercises and physical therapy could not be investigated in this study.
In the total study sample, the low rate for referrals to services (ie, dieticians) for support on losing weight is in line with the results in a recent Australian study.37 However, the low rates are in contrast to the evidence showing that obesity is a risk factor for OA progression and that even modest weight reductions may reduce symptoms.38 A UK survey showed that BMI monitoring and adherence to exercise were less frequently monitored by GPs as compared to pain, function and analgesia. The authors suggest that lack of time, lack of confidence in providing advice and effectiveness of interventions, lack of reimbursements, and lack of patient adherence and motivation represent major barriers to GPs discussing lifestyle interventions (eg, exercise and losing weight) with their patients.39 In this study, the Portuguese cohort had the highest achievement rate for advice on losing weight. Although the Portuguese GPs’ referral rate to weight loss services was only 21%, this was much higher compared to the achievement rates in the other three countries. This finding most likely reflects a priority in the Portuguese healthcare services since most healthcare centres in the region of Algarve have been staffed with a dietician or nutritionist, which is in contrast to that in the other three countries.
Apart from QIs related to weight, the QIs for functional assessments, corticosteroid injections and referrals for surgery represented the lowest achievement rates in this study. This could reflect a lower priority among health professionals for these aspects of OA care or limited access to or availability of such assessments and treatment. The UK and Portuguese cohorts had (non-significantly) higher achievement rates for assessment for walking aids, whereas the Norwegian cohort had the highest rates for daily living appliances/aids. There was a higher achievement rate for recommendation of paracetamol in the Norwegian cohort, and of stronger painkillers in the UK cohort. This may reflect differences in national pharmacological guidelines or differences in the medical practice between the countries.
Strengths and limitations
The application of the same set of QIs across primary healthcare in the same time period and in similar settings in four different European countries allowed for cross-national comparisons and represents a major strength of this study. However, there were some minor differences in the phrasing of the UK QI items compared to the QIs in the other three countries, which may possibly have influenced the patient-reported achievement. Some GPs may have been aware of the items in the questionnaire. If they changed their behaviour due to this, it may have resulted in somewhat higher achievement rates. The populations in the four countries might have been somewhat different due to differences in the inclusion criteria and the target population, which may have influenced the characteristics of participants and the achievement rates. Comorbidity was self-reported in most countries, but extracted from medical records in the UK, so this may have induced some differences between the study populations. However, none of these variables were associated with the number of QIs achieved in the final models. The unknown number of people screened in three countries and the somewhat limited number of participants recruited in each country implies that some caution should be applied in generalising the study results to the general populations in the four countries. However, the results from the Norwegian cohort were similar to the results from a recent nationwide survey, which strengthen the generalisability. It is also a limitation that we had no data on psychological distress or depression, expectations, knowledge on OA treatment and healthcare utilisation and that we were not able to adjust analyses for the differences in healthcare systems and access to OA care across the countries.
Implications
Quality improvement initiatives targeting OA care are becoming increasingly important as the prevalence of OA is expected to further increase, and implementation of evidence-based OA treatment is likely to reduce the associated burden of disability.9–12 Carefully designed QIs have the potential to quantify and address gaps in clinical care,40 and can improve delivery of provided care through an appropriate measurement of healthcare system performance across providers, system levels and regions.41 This study represents a novel attempt to implement the same set of QIs and compare QI achievement rates across populations from four different countries. Adherence to process QIs in rheumatology has recently been shown to be associated with improved patients’ outcomes,42 and a recent study demonstrated that by implementing core recommendations for OA treatment, the need for total joint replacements may be postponed.43 Hence, health professionals should aim for higher adherence to standards of care and guideline recommendations. However, multifaceted approaches, including system-level interventions and patient-focused interventions among others, may be needed to improve the quality of OA care.44 Joint initiatives and cross-country collaborations to improve OA care and implementation of international guidelines could be explored as one of several potential ways to meet this healthcare challenge.
In conclusion, the results of this study indicate that there exists a potential for improvement in OA care in all four countries, but for somewhat different aspects of OA care. QIs may be used to assess and monitor the quality of OA care, and larger studies with more countries and larger sample sizes may allow for further explorations of differences in QI achievement between countries. By exploring such differences and comparing healthcare services across countries, ideas may be generated on how the quality of OA care might be improved internationally.
Acknowledgments
The authors would like to thank the Keele OA Research Users’ Group, the study teams, colleagues and administrative staff at all authors’ workplaces for their support and assistance with this study. They would also like to thank all of the staff and patients at the participating general practices.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
- Data supplement 2 - Online supplement
Footnotes
Contributors HL, KBH, KD and NØ conceived the project and planned the project design together with AH, BC, CC, KPJ and SP. BC, GG, GP, JJE and the MOSAICS study team collected the data. KPJ performed statistical analyses and drafted the results section and tables. NØ drafted the rest and finalised the manuscript. All the authors provided feedback on drafts of this paper and have read and approved the final manuscript.
Funding This project was made possible by funding from the EULAR Health Professional Grant. The Norwegian Fund for postgraduate training in physiotherapy funding NØ through the FYSIOPRIM project is gratefully acknowledged. This paper presents independent research commissioned by the National Institute for Health Research (NIHR) Programme Grant (RP-PG-0407–10 386). The views expressed in this paper are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health. This research was also funded by the Arthritis Research UK Centre in Primary Care grant (grant number 18139). KD is also part funded by the National Institute for Health Research (NIHR) Collaborations for Leadership in Applied Health Research and Care West Midlands by a Knowledge Mobilisation Research Fellowship from the National Institute for Health Research. JJE was supported by an In-Practice Fellowship from the National Institute for Health Research (NIHR). Research of CC was partially funded by Fundação para a Ciência e Tecnologia through the project PEst-OE/MAT/UI0006/2014.
Competing interests KD was a member of the NICE Guideline Development Group and the NICE quality standards group for osteoarthritis.
Patient consent Obtained.
Ethics approval Danish Data Protection Agency, on the 22nd of June 2012 + the Norwegian Regional Committee for Medical and Health Research Ethics on the 19th of October 2011 (REK South-East B 2011/1963 + the Regional Health Administration (ARS-Algarve) on the 27th of July 2012 (077/12 DSPP) + the North West 1 Research Ethics Committee, Cheshire (REC reference: 10/H1017/76) on 26th October 2010 and was monitored by an Independent Trial Steering Committee and Data Monitoring Committee (Trial registration number ISRCTN06984617).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.