Article Text

Abstract
Objectives Patient Global Rating of Change (GRC) scales are commonly used in routine clinical care given their ease of use, availability and short completion time. This analysis aimed at assessing the validity of Patient Global Impression of Change (PGIC), a GRC scale commonly used in fibromyalgia, in a Canadian real-life setting.
Methods 167 fibromyalgia patients with available PGIC data were recruited in 2005–2013 from a Canadian tertiary-care multidisciplinary clinic. In addition to PGIC, disease severity was assessed with: pain visual analogue scale (VAS); Patient Global Assessment (PGA); Fibromyalgia Impact Questionnaire (FIQ); Health Assessment Questionnaire (HAQ); McGill Pain Questionnaire; body map. Multivariate linear regression assessed the PGIC relationship with disease parameter improvement while adjusting for follow-up duration and baseline parameter levels. The Spearman's rank coefficient assessed parameter correlation.
Results Higher PGIC scores were significantly (p<0.001) associated with greater improvement in pain, PGA, FIQ, HAQ and the body map. A statistically significant moderate positive correlation was observed between PGIC and FIQ improvement (r=0.423; p<0.001); correlation with all remaining disease severity measures was weak. Regression analysis confirmed a significant (p<0.001) positive association between improvement in all disease severity measures and PGIC. Baseline disease severity and follow-up duration were identified as significant independent predictors of PGIC rating.
Conclusions Despite that only a weak correlation was identified between PGIC and standard fibromyalgia outcomes improvement, in the absence of objective outcomes, PGIC remains a clinically relevant tool to assess perceived impact of disease management. However, our analysis suggests that outcome measures data should not be considered in isolation but, within the global clinical context.
- Fibromyalgis/Pain Syndromes
- Patient perspective
- Disease Activity
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Disease severity assessment among fibromyalgia patients remains difficult due to the absence of evaluable objective outcomes or biomarkers, therefore physicians commonly rely on patient global rating of change scales given their ease of use, availability and completion time.
What does this study add?
Higher Patient Global Impression of Change (PGIC) scores were significantly associated with greater improvement in pain, Patient Global Assessment (PGA), Fibromyalgia Impact Questionnaire (FIQ), Health Assessment Questionnaire (HAQ) and the body map though a weak correlation was observed between PGIC and the fibromyalgia outcomes improvement with the exception of FIQ which had a moderate positive correlation with PGIC.
Baseline disease severity and follow-up duration were identified as significant independent predictors of PGIC rating.
How might this impact on clinical practice?
PGIC represents a clinically relevant tool to assess perceived impact of disease management.
However, our analysis suggests that outcome measures data should not be considered in isolation but within the global clinical context.
Introduction
Fibromyalgia (FM) is a heterogeneous syndrome characterised by chronic widespread pain and the presence of a multitude of symptoms that vary considerably in terms of expression and intensity.1 ,2 Although it is now recognised that symptoms of FM seldom disappear completely, patients often experience a waxing and waning course, with treatment objectives directed towards a general reduction and stabilisation of symptoms. Symptoms that commonly coassociate with FM may include fatigue, sleep disturbance, cognitive dysfunction and psychological symptoms such as depression and anxiety.1 ,2 It has been estimated that between 30% and 60% of patients with FM experience psychiatric comorbidities.1 It is the overall combination of these symptoms that contribute to the overall burden of suffering experience by patients with FM.2
There is currently no consensus concerning the best method to assess treatment outcomes or symptom modifications in persons with FM.2 This may be explained by the difficulty in assessing disease severity when complaints are only subjective with absence of evaluable objective outcomes or biomarkers.3 As a result, physicians must solely rely on patient-reported symptoms.3
Patient Global Rating of Change (GRC) scales are useful in this regard since they aim to quantify disease activity relative to an anchor point.4 ,5 Specifically, patients are asked to calculate the difference between their current and previous health state based on a Likert scale. GRC scales offer various benefits in clinical practice. Although GRC scales typically comprise between 7 and 11 points which show optimal patient preference, discriminative ability and test–retest ability, they can be tailored to specific conditions and disease parameters as per the clinicians’ needs.4 ,6 Their applicability to a multitude of conditions as well as their availability to the patient population make them an appealing option for clinicians.4 Moreover, GRC scales are simple to employ; scores are easily calculated and no previous training is required for their use, as opposed to other health questionnaires.7 The allowance of patients to include which constructs they judge to be the most important in their health status guarantees the clinical relevance of the data collected.4 ,8 Nonetheless, certain limitations exist in the usage of GRC. Since different aspects of FM may be considered important by individual patients, this could render the comparison of patients’ GRC scales problematic.4 In addition, previous studies have shown that patients with less severe baseline dysfunction report smaller score variation over time as compared to patients with higher baseline dysfunction scores may be fraught with inaccuracy, particularly in scales with long periods of interest or with long follow-up periods where recall bias may arise.9 ,10
Given that meaningful interpretation of results can only be performed with due consideration of the clinimetric properties and strengths/weaknesses of each instrument, the aim of this analysis was to assess the validity of Patient Global Impression of Change (PGIC), a GRC scale commonly used in the management of patients with FM, in a Canadian routine clinical care setting.
Methods
Study design
This was a single centre prospective observational cohort study of patients diagnosed with FM and followed at the Alan Edwards Pain Management Unit, a tertiary care multidisciplinary clinic in Canada, between May 2005 and March 2013. The mission of this clinic is the evaluation and management of patients with FM according to the specific needs of the patients. The study cohort has been previously described.11 Treatment was not predetermined; patients received a tailored treatment according to best clinical practice. Patients with another primary cause of pain, even with an associated diffuse pain syndrome, were excluded from the study. Moreover, patients who refused to participate or who were unable to answer French or English questionnaires were further excluded. Most patients were referred by primary care physicians though some were referred by other specialists. Finally, to be eligible for this analysis, men and women were clinically diagnosed with FM, were at least 18 years old and had at least one follow-up assessment.
The registry is approved by the institutional review board of the Montreal General Hospital. All patients signed informed consent forms prior to enrolment.
Outcome measures
In addition to the PGIC, disease severity was assessed with the pain visual analogue scale (VAS), the Patient Global Assessment (PGA), the Fibromyalgia Impact Questionnaire (FIQ), the Health Assessment Questionnaire (HAQ), the McGill Pain Questionnaire (MPQ) and a body map.
The PGIC evaluates overall health status as perceived by the patient in a seven-point single-item scale ranging from ‘very much worse’ to ‘very much improved’. For descriptive purposes, patients were classified into three categories according to the PGIC score: disease deterioration (0–3 points), stable disease (4 points) or disease improvement (5–7 points) since the initial baseline visit. The pain VAS is a simple measure which allows patients to mark the average severity of their pain on a 10 cm scale (ranging from ‘no pain’ at 0 cm to ‘worst imaginable pain’ at 10 cm) over the preceding week.12 The PGA is also a numerical measure of global disease severity over the preceding week and ranges from 0 cm (‘very well’) to 10 cm (‘very poorly’).13 The FIQ is a functional and symptom based questionnaire specific to FM, assessing FM-related consequences including the ability to perform routine physical tasks as well as pain and psychological variables.14 The HAQ is a reliable, valid and user-friendly tool which assesses five dimensions of health: disability, pain, medication effects, costs of care and mortality.15 The MPQ evaluates pain using three descriptors: sensory, affective and evaluative for a total of 78 questions.16 The body map comprises a drawn manikin, with a front and back view, and is shaded by the patient to record location of pain. It is completed by the patient and 50 areas are quantitatively scored (26 back and 24 front) with a score of 1 or 0.17
Statistical methods
Descriptive statistics were produced for all variables. Central tendency (mean) and dispersion (SD) statistics were produced for continuous variables and frequency distributions for categorical variables. Between-group differences in disease parameters were assessed for statistical significance with one-way analysis of variance. Multivariate linear regression was used to assess the relationship between PGIC and changes in disease parameters over time while adjusting for duration of follow-up and baseline levels of each parameter. Parameter correlation was assessed with the Spearman's rank coefficient (r) using the following cut-offs: weak: <0.4, moderate: between 0.4 and 0.6, strong: >0.6. The level for statistical significance was set a priori at 0.05. All statistical analyses were performed using SPSS V.21.0 for Windows (SPSS Inc., Chicago, Illinois, USA).
Results
One hundred and sixty-seven patients were included, of whom 152 (91.0%) were female. Mean±SD age and pain duration were 48.8±9.8 and 10.9±10.2 years, respectively. The mean±SD follow-up duration was 30.0±15.3 months. In regard to disease severity measures, mean±SD pain, PGA, body map, FIQ, HAQ and MPQ were 6.6±2.2 cm, 6.5±2.3 cm, 27.0±9.9, 66.1±17.0, 1.10±0.64, and 41.5±15.2, respectively (table 1). Overall, the baseline patient profile of the cohort was typical of patients with FM.
Patient demographics and characteristics
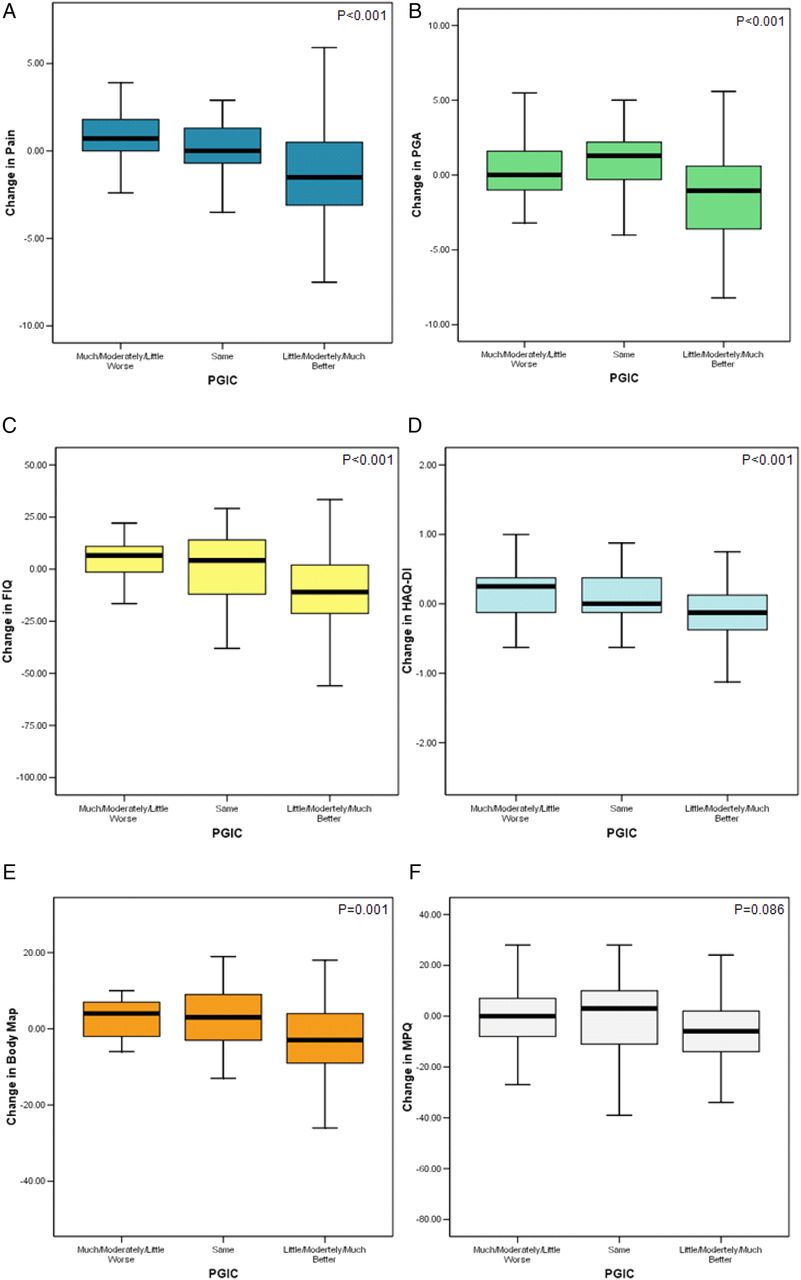
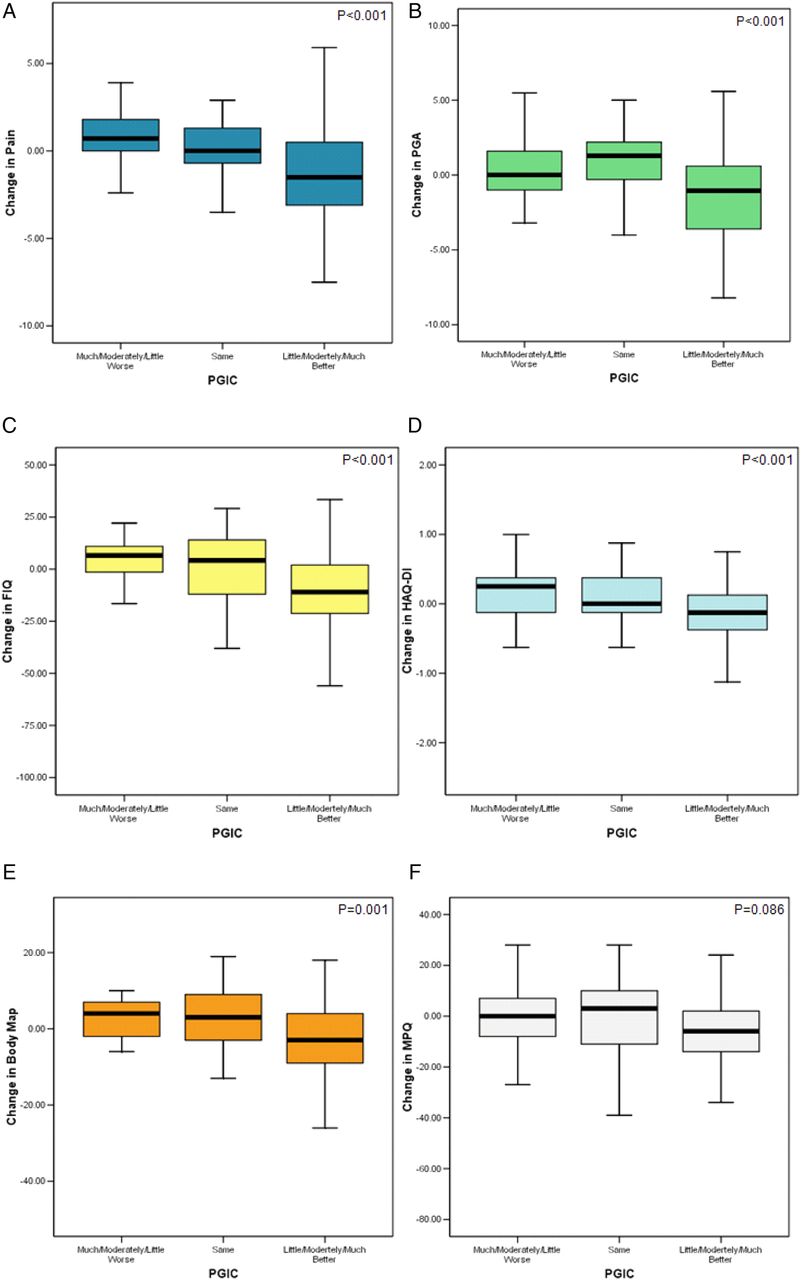
Higher PGIC scores were significantly associated with greater improvement in pain, PGA, FIQ, HAQ and the body map (figure 1). Specifically, patients rating their condition having improved (little, moderately, or much better) since treatment initiation reported having experienced significantly (p<0.001) greater reduction in pain from baseline, compared to patients rating their condition as stable or deteriorating (much, moderate, little worse) (1.03 cm vs 0.31 cm vs −1.31 cm unit, respectively) (figure 1A). Similar results were observed for the remaining disease severity measures suggesting the presence of a positive association with PGIC. The only exception was the MPQ which showed a statistical trend (p=0.086) but did not reach statistical significance (−0.66 vs −1.88 vs −6.58 in patients rating their global disease status as better, stable or worse, respectively) (figure 1F).
{kind=link}
Association between PGIC and change (Δ) in (A) Pain (VAS), (B) PGA, (C) FIQ, (D) HAQ, (E) Body Map, (F) MPQ). HAQ, Health Assessment Questionnaire; MPQ, McGill Pain Questionnaire; PGA, Patient Global Assessment; PGIC, Patient Global Impression of Change; VAS, visual analogue scale.
In correlation analysis, a statistically significant moderate positive correlation was observed between PGIC and FIQ improvement (r=0.423; p<0.001) (table 2). The remaining disease severity measures showed statistically significant (p<0.001) weak positive correlations with PGIC. More specifically, the correlation coefficient between PGIC and each measure were: pain (VAS) (r=0.387), PGA (r=0.327), Body Map Score (r=0.287), HAQ (r=0.343), and MPQ (r=0.250) (table 2).
Correlation between PGIC and change (Δ) in disease severity measures
Regression analysis confirmed the presence of a significant (p<0.001) positive association between improvement in all disease severity measures and PGIC (table 3). In addition, increased baseline disease severity, as defined by all disease severity measures, was associated with significantly (p≤0.001) lower PGIC scores (less improvement). Longer duration of follow-up was also identified as an important predictor of lower patient reported global impression of change, with each additional month of follow-up being associated with a lower PGIC rating by −0.01 to −0.02.
Association of PGIC with Duration of Follow-Up*
Discussion
To our knowledge, this analysis is the first to validate prospectively the PGIC scale among patients with FM over a long-term period. Overall, a statistically significant weak positive correlation exists between PGIC and improvement in standard FM outcome measures. This is in agreement with previous studies by Stratford et al18 and Stucki et al19 which showed that patients with a clinically relevant GRC change reported more disease improvement in the Roland-Morris Back Pain Questionnaire and SF-36 physical scale, respectively. The FIQ showed the highest correlation with PGIC as compared to the specific measurement of pain, PGA, body map, HAQ and McGill questionnaires. This could be explained by the fact that these questionnaires measure specific aspects of FM whereas FIQ, similar to PGIC, generally incorporates a variety of constructs, both function and symptom based, that are important to each individual patient.4
Baseline disease severity, irrespectively of measure assessed, was also identified as a significant predictor of patient perception of disease improvement. Patients rating their baseline disease as more severe reported a lower global impression of change (indicating disease deterioration or lower improvement), compared to patients experiencing similar changes in disease severity measures over comparable follow-up duration. This association remained significant even after adjusting for education, as a marker of socioeconomic status, which is a known predictor of patient perception of illness.20 These findings may serve to highlight the heterogeneity in disease burden experienced by individual patients with FM. Some patients may experience symptoms at the mild end of the spectrum with ability to maintain function, whereas others may experience more severe disease and impaired function. This concept of categorising patients into disease severity perception subgroups could be a useful clinical tool to facilitate patient care and requires further exploration.
In addition to baseline disease severity, duration of follow-up was also found to have a statistically significant, although not necessarily clinically meaningful, impact on PGIC; patients followed up for longer periods rated their disease as having lesser improvement, compared to patients with shorter follow-up experiencing similar changes in disease severity measures. This could be due to patient recall bias or, alternatively, the reprioritisation of the importance of certain constructs (eg, fatigue, sleep disturbance, cognitive dysfunction and psychological symptoms) over time modifying the rating of the scale. Although the optimal length of time to minimise recall bias with GRC scales has not been established, Schmitt and Abbott5 showed that GRC correlations with changes in functional status scores had overlapping CIs between recall periods of less than 1 month and periods up to 6 months, thus suggesting that even short follow-up periods may have an impact on the internal validity of GRC scales.
In summary, the current analysis has shown that only a weak positive correlation exists between PGIC and improvement in standard FM outcome measures. Despite this, in the absence of hard outcomes in FM, physicians must rely on patient-reported symptoms, rendering PGIC a clinically relevant tool in the assessment of perceived impact of FM disease management. Based on our analysis, data from outcome measures, particularly PGIC, should not be considered in isolation but within the global clinical context. Furthermore, our analyses identified baseline disease severity and duration of follow-up as independent predictors of PGIC rating, suggesting that the evaluation of serial measures may be preferable to self-reported change when follow-up time stretches to several months.
References
Footnotes
Contributors All authors satisfy the ICMJE authorship criteria, namely: Substantial contributions to the conception or design of the work, or the acquisition, analysis or interpretation of data. Drafting the work or revising it critically for important intellectual content. Final approval of the version published. Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Competing interests None declared.
Patient consent Obtained.
Ethics approval This study involved human subjects. Ethics committee/institutional review board approval was obtained from the Montreal General Hospital institutional review board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.