Article Text

Abstract
Objectives To identify predictive factors of radiological progression in early arthritis patients treated by remission-steered treatment.
Methods In the IMPROVED study, 610 patients with early rheumatoid arthritis (RA) or undifferentiated arthritis (UA) were treated with methotrexate (MTX) and a tapered high dose of prednisone. Patients in early remission (disease activity score (DAS) <1.6 after 4 months) tapered prednisone to zero. Patients not in early remission were randomised to arm 1: MTX plus hydroxychloroquine, sulfasalazine and prednisone, or to arm 2: MTX plus adalimumab. Predictors of radiological progression (≥0.5 Sharp/van der Heijde score; SHS) after 2 years were assessed using logistic regression analysis.
Results Median (IQR) SHS progression in 488 patients was 0 (0–0) point, without differences between RA or UA patients or between treatment arms. In only 50/488 patients, the SHS progression was ≥0.5: 33 (66%) were in the early DAS remission group, 9 (18%) in arm 1, 5 (10%) in arm 2, 3 (6%) in the outside of protocol group. Age (OR (95% CI): 1.03 (1.00 to 1.06)) and the combined presence of anticarbamylated protein antibodies (anti-CarP) and anticitrullinated protein antibodies (ACPA) (2.54 (1.16 to 5.58)) were independent predictors for SHS progression. Symptom duration <12 weeks showed a trend.
Conclusions After 2 years of remission steered treatment in early arthritis patients, there was limited SHS progression in only a small group of patients. Numerically, patients who had achieved early DAS remission had more SHS progression than other patients. Positivity for both anti-CarP and ACPA and age were independently associated with SHS progression.
Trial registration numbers ISRCTN Register number 11916566 and EudraCT number 2006 06186-16.
- Ant-CCP
- Early Rheumatoid Arthritis
- Treatment
- Autoantibodies
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
Earlier treatment with combination therapy and a treat-to-target approach have resulted in earlier and better suppression of inflammation, and radiological progression in patients with rheumatoid arthritis.
Induction therapy followed by remission-steered treatment results in less Sharp/van der Heijde score (SHS) progression in rheumatoid arthritis and undifferentiated arthritis.
Age is associated with minimal SHS progression, which may represent primary hand osteoarthritis with increasing age causing joint space narrowing.
Combination of anticarbamylated protein antibodies and anticitrullinated protein antibodies positivity is also associated with minimal SHS progression, which represents a phenotype with particularly bad prognosis.
Identifying predictive factors of minimal SHS progression may be relevant for understanding RA phenotypes; however, it is unlikely that limited SHS progression will become clinically relevant in the intermediate future.
Introduction
Rheumatoid arthritis (RA) treatment has considerably changed in the past decades. Earlier treatment with combination therapy and a treat-to-target approach have resulted in earlier and better suppression of inflammation and radiological progression.1–7 It is thought that induction of disease activity score (DAS) remission, for which even stricter criteria are defined, will ensure optimal suppression of disease processes.8 With joint destruction becoming a rare outcome, this is mainly of pathophysiological interest, which patients remain most at risk for radiological progression.
Anticitrullinated protein antibodies (ACPA) positivity in RA is associated with more radiological joint damage; in undifferentiated arthritis (UA) and arthralgia it predicts progression to RA.9 ,10 Also, the recently identified anticarbamylated protein antibodies (anti-CarP) are associated with more radiological progression, specifically in ACPA-negative patients.9 The presence of anti-CarP predates clinical disease;11–13 in arthralgia patients it can predict the progression to RA regardless of ACPA status.10
In addition, previous research showed that loss of bone mineral density, as measured with Digital X-ray Radiogrammetry (DXR-BMD) in the metacarpals using standard hand radiographs, in the first 4 months is associated with radiological progression after 1 year.14 Local BMD loss occurs early in the disease course and may be caused by increased osteoclast activity caused by inflammation processes.
In the IMPROVED study, we treated patients with early RA and UA with the aim to induce and maintain clinical remission (DAS<1.6). DAS remission rates were high, and radiological progression low.7 ,15 Yet, some patients still developed radiological progression, and this provides an opportunity to look for factors associated with and potentially driving radiological progression. Thus, in this post hoc analysis we aimed to determine which baseline characteristics and 4-month outcomes are associated with joint damage after 2 years of remission-steered treatment.
Methods
Subjects and study design
The IMPROVED study is a multicentre, randomised clinical trial with 610 patients ≥18 years having symptom duration ≤2 years, and not treated with previous antirheumatic therapy, diagnosed with early RA (2010 classification criteria16) or UA, defined by at least one inflammatory arthritis and one other painful joint, clinically suspected for early RA according to the treating rheumatologist. Medical Ethics Committees of all participating centres approved the study protocol and all patients gave written informed consent.
All patients started treatment with methotrexate (MTX) 25 mg/week and prednisone tapered from 60 mg/day to 7.5 mg/day in 7 weeks. After 4 months, patients who achieved a DAS<1.6 (early DAS remission) tapered prednisone to 0. If remission was maintained at 8 months, MTX was tapered to 0. Patients who were not in early DAS remission after 4 months were randomised to arm 1: MTX, hydroxychloroquine (HCQ), sulfasalazine (SSZ) and prednisone, or to arm 2: MTX+adalimumab. If patients in arm 1 were in remission after 8 months, first prednisone, then SSZ and finally HCQ were tapered to 0. Four months later, MTX could be tapered to 0 if patients achieved remission. In arm 2, after 8 months, adalimumab was tapered to 0 if patients achieved remission and if the remission was maintained 4 months later, MTX was tapered to 0. Treatment adjustments were made every 4 months; medication was tapered and finally stopped in case of remission, but increased or switched in case of no remission. Fifty patients who did not achieve early DAS remission were not randomised as the protocol required; they were treated outside of protocol (OP) according to their rheumatologist based on the DAS. Details about the study protocol were previously published.7 We used data from 488 patients who had full sets of radiographs of hands and feet at baseline and after 2 years. For the other patients either a baseline or 2-year radiograph was missing.
Measurements
Radiological damage was assessed from radiographs of hands and feet annually in random order using the Sharp/van der Heijde score (SHS) as the mean of two independent readers, blinded for patient identity.17 Radiological progression was defined as an increase in SHS≥0.5 point. Since only a small group of patients (50/488) showed progression, reliability could not be measured by intraclass coefficients.18 Consensus scores were reached for radiographs with inter-reader difference of ≥2 points progression. Suitable routine digital X-rays of both hands were used to measure DXR-BMD by DXR online (Sectra, Linköping, Sweden)19 at baseline and 4 months. ‘DXR-BMD loss’ was defined as a loss in DXR-BMD of ≥1.5 mg/cm2/4 months calculated by subtracting DXR-BMD at 4 months with DXR-BMD at baseline.14
Anti-CarP were measured in sera at baseline by ELISA using carbamylated FCS in-house as described before.9 ACPA were determined at baseline using the anticyclic citrullinated peptide (anti-CCP2) test.
‘Boolean remission’ was defined by the 2011 American College of Rheumatology European League Against Rheumatism (ACR/EULAR) remission criteria8 and was measured after 4 months.
Statistical analysis
For the analysis of continuous data we used the independent t test and for categorical data, the χ2 test. Mann-Whitney test and χ2 test were used for non-Gaussian data.
Clinical and radiological predictors at baseline and 4-month outcomes were put into the univariable logistic regression analysis with SHS progression as binary outcome. Variables with a p value <0.2 were entered into the multivariable model.
Early DXR-BMD loss showed a p value <0.2; however, this was a variable with almost half of the missing values due to unsuitability of the X-rays to measure the DXR-BMD. In order to avoid bias and to increase power, the variable was imputed using multiple imputation in 442 patients who had at least one DXR-BMD measure.
Anti-CarP and ACPA could not be entered into the same model due to multicollinearity. Therefore, a combined variable was entered into the model. Data was analysed by the statistical program SPSS V.20.0.
Results
Clinical characteristics and treatment
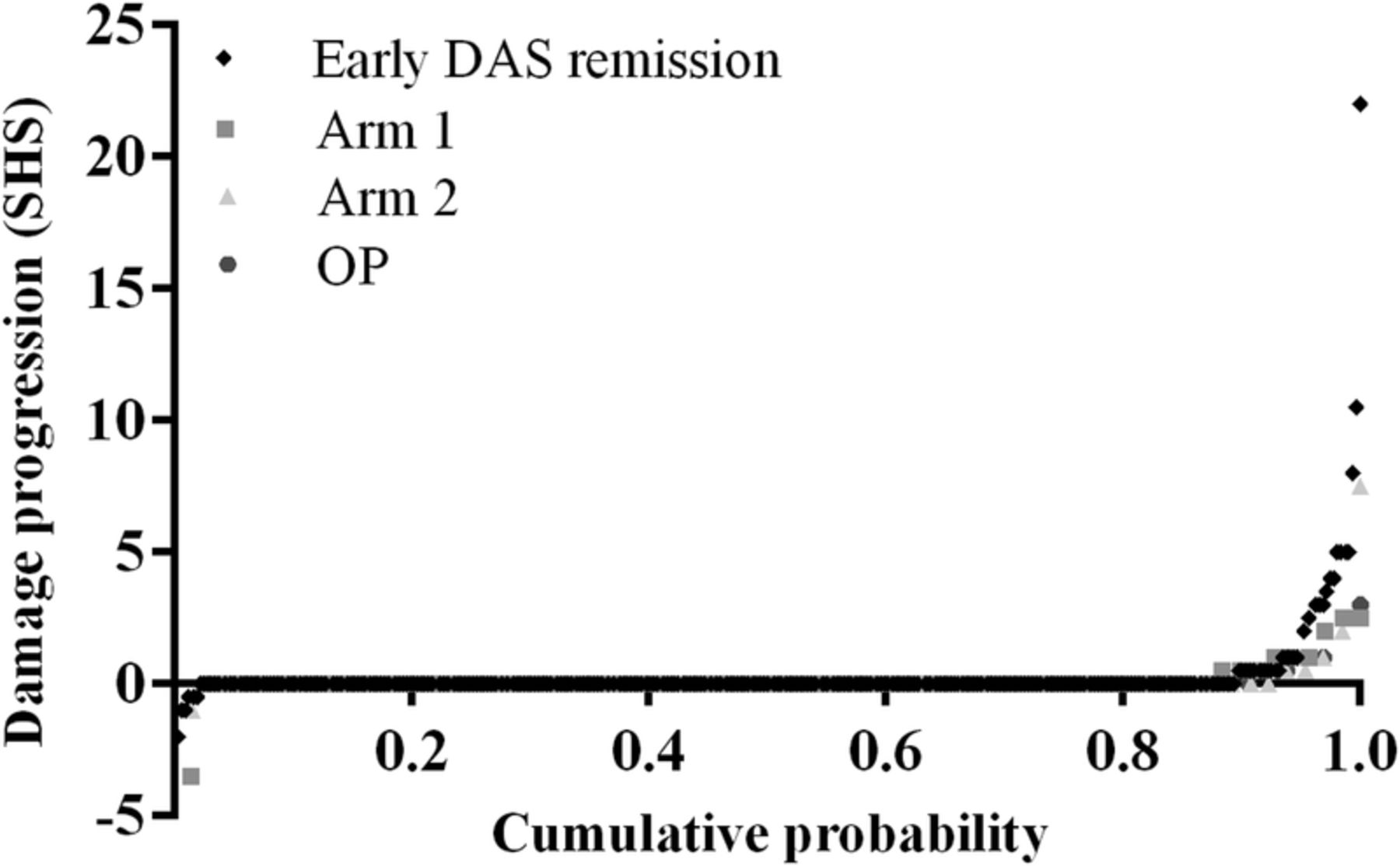
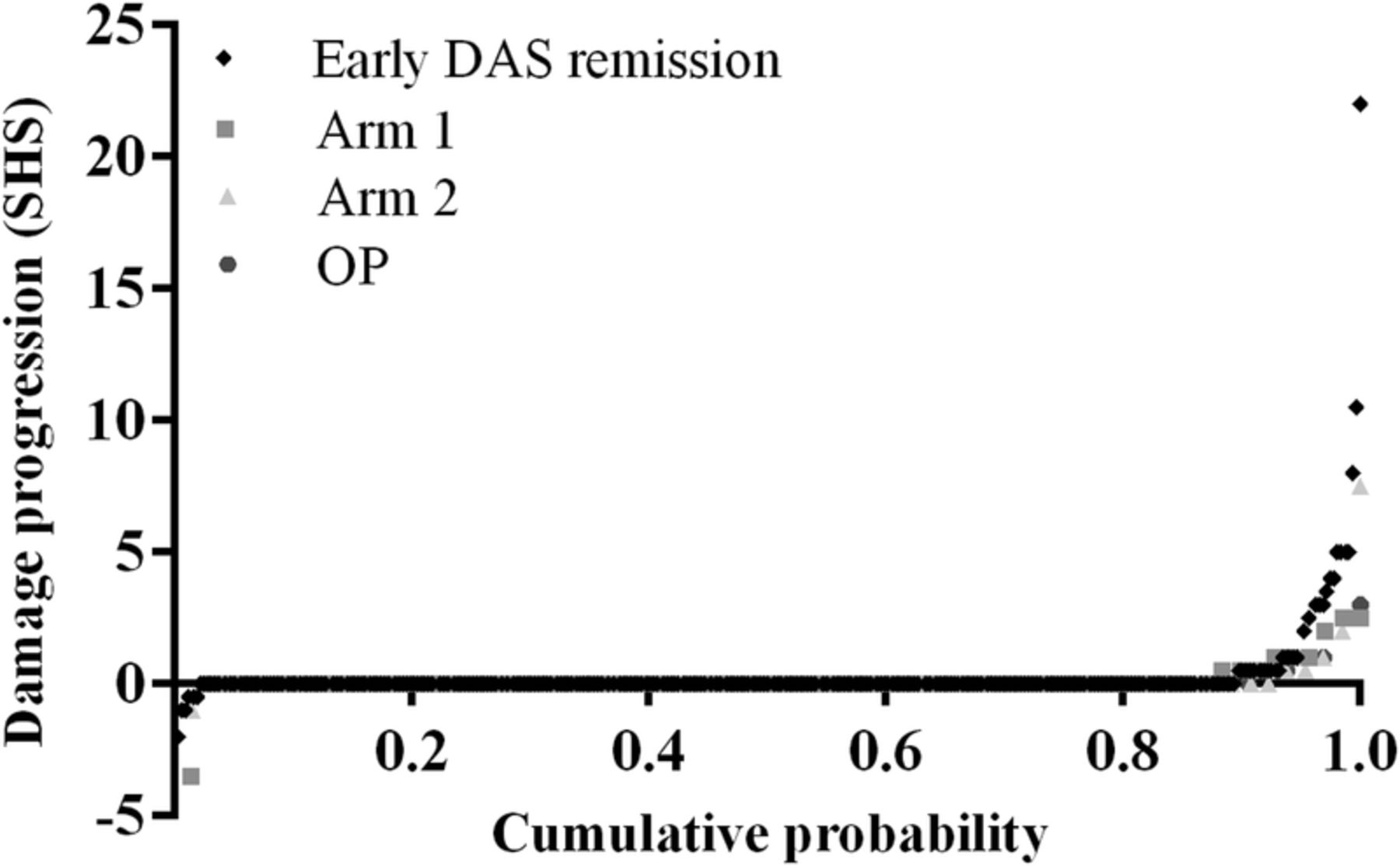
After 2 years, median SHS progression in all groups (early DAS remission, arm 1, arm 2, and OP) and in patients with RA and UA was 0 (range 0–22). Fifty of 488 patients (10%) had SHS progression: 33/387 (9%) in early DAS remission, 9/83 (11%) in arm 1, 5/78 (6%) in arm 2, 3/50 (6%) in the OP group (table 1 and figure 1). JSN progression was seen in 23/33 patients in early DAS remission, 9/9 in arm 1, 4/5 in arm 2, and 2/3 in the OP group. Erosion progression was scored in 17/33 patients in early DAS remission, 0 in arm 1, 2 in arm 2, and 1 in the OP group. Eight of 50 (16%) patients (all RA, 7 in early DAS remission and 1 in arm 2) had ≥5 SHS progression (minimal clinically important difference and smallest detectable difference20) (see online supplementary table S1). Twenty-two of 50 (44%) patients (20 patients with RA and 2 patients with UA, 16 in early DAS remission, 3 in arm 1, 2 in arm 2, and 1 in OP group) had ≥2 SHS progression (smallest detectable change21). Ten of 33 early DAS remission patients with SHS progression were in drug-free remission (DFR) after 2 years. One of 33 patients had ≥5 SHS progression (see online supplementary table S1).
Supplementary table
Treatment steps during 2 years of follow up in patients with SHS progression n=50
Baseline characteristics and clinical outcomes for the total population, SHS progression and no SHS progression
{kind=link}
Probability plot of SHS progression over 2 years for the different treatment groups (uploaded as a separate file: figure 1). DAS, disease activity score; OP: outside of protocol group; SHS: Sharp/van der Heijde score.
After 4 months, 144 patients (all in early DAS remission) were in ‘Boolean remission’. Mean (SD) age in ‘Boolean remission’ patients was 51.2 (14.3) years, and 51.8 (13.9) years for patients not in ‘Boolean remission’, p=0.662 (table 2). ACPA positivity (86 (60%) vs 223 (53%), p=0.106) and anti-CarP positivity (47 (33%) vs 116 (28%), p=0.166) were similar in both groups. SHS progression was seen in 16/144 (11%) of ‘Boolean remission’ patients and 31/420 (7%) patients not in ‘Boolean remission’ (p=0.264). The other three patients who had SHS progression had missing data to calculate ‘Boolean remission’. Median (IQR) SHS progression was not different in patients in ‘Boolean remission’ 0 (0–0), and patients not in ‘Boolean remission’ 0 (0–0), p=0.357.
Baseline characteristics and clinical outcomes according to ‘Boolean remission’ measured after 4 months
SHS progression
Median (IQR) SHS progression in patients with SHS progression was 1.0 (0.5–3.0); joint space narrowing (JSN) progression 1.5 (0.8–3.0), and erosion progression 0.5 (0.0–1.0). Thirty-eight of 488 patients (30 RA and 8 UA, p=0.831) had JSN progression and 20/488 (19 RA and 1 UA, p=0.145) had erosion progression. Patients with SHS progression were older (5/50 patients with SHS progression were <45 years vs 122/438 patients without SHS progression were <45 years, p=0.035), had a longer symptom duration (11/50 symptom duration <12 weeks vs 146/438, p=0.092, respectively), were more often anti-CarP-positive (p=0.012) and numerically also more often ACPA-positive or RF-positive, and had a higher erythrocyte sedimentation rate (ESR) (31/50 ESR >28 mm/hr vs 183/438, p=0.006, respectively) (table 1).
Anti-CarP
One hundred thirty-nine of 488 patients (28%) were anti-CarP-positive; 274/488 (56%) were ACPA-positive; 273/488 (56%) were RF-positive; 122/488 (25%) were double positive for anti-CarP and ACPA; and 107/488 (22%) were positive for all three. Double positivity occurred more in patients with RA than in patients with UA (table 3). In anti-CarP-positive patients there was no difference between ACPA-positive and ACPA-negative patients in SHS progression (median (IQR) 0 (0–0) vs 0 (0–0), p=0.354). Median (IQR) SHS at baseline and 2 years was comparable between anti-CarP-positive and anti-CarP-negative patients (table 3). Besides, median SHS at baseline was comparable between double positive (0 (0–1)) and ACPA-positive but anti-CarP-negative patients (0 (0–2), p=0.088) and also at 2 years this was comparable 0 (0–0) vs 0 (0–0.5), p=0.073.
Baseline characteristics and clinical outcomes according to anti-CarP status
Predictors of SHS progression
Univariable predictors for SHS progression after 2 years that were entered into the multivariable model showed double positivity for anti-CarP and ACPA (p=0.011), anti-CarP alone (p=0.014) (ACPA alone showed a trend (p=0.056)), age (p=0.009), baseline ESR>28 mm (p=0.007), baseline SHS (p=0.041) and symptom duration <12 weeks (showed a trend p=0.096; table 4). Early DXR-BMD loss was associated with SHS progression (p=0.019); however, the imputed variable was not associated (p=0.100) and therefore, not entered in the model. Only age (OR (95% CI): 1.03 (1.00 to 1.06)) and the combination of anti-CarP and ACPA positivity (2.54 (1.16 to 5.58)) were independent significant predictors (table 4). Symptom duration <12 weeks (0.49 (0.23 to 1.04)), ESR>28 mm (1.90 (0.95 to 3.81)), and SHS (1.04 (0.98 to 1.11)) were not significantly associated, but were entered in the model because of a probable association with SHS progression.
Univariable and multivariable logistic regression analysis with SHS progression as binomial outcome variable
An additional multivariable model including only ACPA and not anti-CarP showed that symptom duration, age and ESR were independent significant predictors (data not shown). A model with anti-CarP instead showed that only anti-CarP was the independent predictor (data not shown). The model with ACPA was a stronger predictor with a R2 of 0.053 compared to 0.047 for the model with anti-CarP.
Discussion
Of 488 early patients with arthritis who were treated with induction therapy followed by remission-steered treatment, only 50/488 (10%) patients showed SHS progression ≥0.5 after 2 years and only 8 patients showed SHS progression ≥5 which is considered to be the minimal clinically important difference in SHS. We looked at potential predictors of radiological progression (after 2 years of treatment) in these patients where disease activity was generally low, and radiological progression was generally effectively suppressed as this allowed us to look for factors associated with radiological progression unconnected to (suppression of) inflammation. This may be relevant for understanding RA phenotypes. It is unlikely that limited SHS progression will become clinically relevant for these patients in the intermediate future.
To determine why this group still shows SHS progression, we investigated associations between baseline characteristics and 4-month outcomes with SHS progression. We found that SHS progression comprised more of progression of JSN than of progression of erosions. Small numbers prevented us from analysing both forms of progression separately. Independent predictors for total SHS progression were higher age and the combination of anti-CarP and ACPA positivity. In a reverse of an association between higher disease activity and more damage progression, we found more SHS progression in patients who had achieved early (4 months after treatment start) DAS remission, or even early ‘Boolean remission’. Although these patients even after drug tapering as required by protocol on average have lower DAS than patients who did not achieve early remission and for whom medication was intensified, it may be possible that there was residual inflammation which triggered the SHS progression. Discontinuation of prednisone may also have removed a drug which even without influencing the DAS may prevent damage progression.22 As online supplementary table S1 suggests, discrepancies in clinical response and radiological damage progression may indicate that in some patients antirheumatic treatment may effectively suppress symptoms of inflammation, while the underlying processes driving joint destruction may still be present.
Although for most patients treated for DAS remission the SHS progression may be a clinically irrelevant finding, for some patients initial SHS progression will still result in later permanent disability23 that will require tailored treatment decisions. In addition, identifying risk factors for SHS progression in this population may point towards underlying mechanisms and possibly to new drug targets.
Small numbers limited our choice of analyses and interpretation of results. Since both ACPA and anti-CarP have been shown to be related with SHS progression in other RA cohorts, it is likely that this combination of risk factors indicate a RA phenotype with a bad prognosis for joint damage. As there were few patients with anti-CarP but with negative ACPA, we could not test which of the antibodies was the stronger predictor. However, it appears that in this early and progressively treated patient group, presence of ACPA is a risk factor for SHS progression only if anti-CarP was also present. Although data in animal studies suggested a direct effect of human ACPA on osteoclastogenesis, several questions remain open regarding the biochemical nature of ACPA and the specificities involved.24 The effects of anti-CarP in joint destruction on such a mechanistic level is currently unknown, but epidemiological studies show a clear association between anti-CarP and joint destruction, especially in the ACPA-negative patients.9 ,11 Also with regard to double positivity of anti-CarP and ACPA, the diagnostic value was clear with high OR for RA. As ACPA and anti-CarP can bind to different antigens,13 it is possible that especially the combined presence is sufficient to drive bone destruction. However, even though mice can harbour anti-CarP antibodies,25 experimental evidence to indicate a pathological role for anti-CarP is still lacking.
We found age to be a predictor of SHS progression. As we found that SHS progression was dominated by JSN progression rather than erosion progression in these patients, some JSN progression may represent primary hand osteoarthritis. This has been also previously suggested in a study by Khanna et al.26
Short symptom duration showed a trend as a protective factor; however, possibly due to small numbers, this was not statistically significant. It is also possible that the intensive remission steered treatment in all patients obscured potential advantages of early treatment start. Previous research indicates that shorter symptom duration in RA is associated with less SHS progression.27 ,28 SHS progression occurred numerically more often in patients with RA than in patients with UA. This corroborates the FINRA-Co and NEORA-Co findings that included not UA but only patients with RA, who despite remission-steered treatment showed more SHS progression than the IMPROVED patients. It may also reflect that classification as RA according to the 2010 classification criteria, used in our study, can rest strongly on the presence of ACPA.
It was not possible to calculate progression in 122 patients due to missing radiographs at baseline or at 2 years. Of these 122 patients, 79 were lost to follow-up and 43 patients had missing radiographs while they were in the study. We could not detect systematic errors concerning these missing radiographs and therefore, consider that we have analysed a considerable part of the data.
A threshold for SHS progression of 0.5 seems clinically irrelevant. The majority of our patients had ‘zero progression’. Only a small group had progression within a small range. This damage progression is at least pathophysiologically of interest. JSN that is scored may represent OA mechanisms in our patients; this was also found as a result of our regression analysis.
Finally, SHS progression appeared slightly higher in patients who had achieved early DAS remission. By protocol, patients were required to taper and eventually discontinue all disease-modifying antirheumatic drugs (DMARDs) when DAS remission was achieved, but had to restart as soon as DAS remission was lost. Previously, we found no radiological damage progression in patients with RA who had drug-free remission in the BeSt study, regardless of whether drug free remission was lost or not.29 Compared to the IMPROVED patients, however, BeSt patients had tapered medication over a long period of low disease activity and subsequent remission before the last DMARD was stopped. In the current study, initiated in 2007, tapering and drug discontinuation was carried out more quickly as we also included patients with UA, some of whom could have had a self-limiting, non-damaging type of arthritis. It is possible that if DMARDs are discontinued too quickly the RA disease activity is not sufficiently suppressed, allowing SHS progression in some patients. Studies involving imaging techniques in patients who are in clinical remission also suggest that residual inflammation may be present, which can be associated with subsequent damage progression.30–32 In our study we did not perform additional imaging to detect this residual subclinical disease. The 2010 EULAR recommendations advise to taper DMARDs slowly only in patients with stable remission and discontinuation of DMARDs is not encouraged, although it is considered to be an option in some patients. However, we found that DFR was achieved in similar percentages of patients who had achieved early DAS remission with or without SHS progression. To continue treatment when patients are in DAS remission might prevent further SHS progression; however, without clear clinical benefits this probably would entail overtreatment with unnecessary (risks of) side effects.
In conclusion, after 2 years of remission-steered treatment in early arthritis patients who started induction therapy, minimal SHS progression occurs in a small group of patients. Independent predictors for SHS progression were age (associated with JSN possibly related to osteoarthritis), and the combination of anti-CarP and ACPA positivity, which appears to represent a phenotype with particularly bad prognosis even when suppression of inflammatory activity by remission-steered treatment prevents damage in other patients. Further research may show whether previous associations of presence of ACPA with bad outcomes of arthritis rests with mechanisms related to ACPA itself, presence of both ACPA and anti-CarP, or mainly with anti-CarP.
Acknowledgments
The authors would like to thank all patients as well as the following rheumatologists (other than the authors) who participated in the IMPROVED study group (all locations are in the Netherlands): WM de Beus (Medical Center Haaglanden, Leidschendam); MHW de Bois (Medical Center Haaglanden, The Hague); M de Buck (Medical Center Haaglanden, Leidschendam); G Collée (Medical Center Haaglanden, The Hague); JAPM Ewals (Haga Hospital, The Hague); RJ Goekoop (Haga Hospital, The Hague); BAM Grillet (Zorgsaam Hospital, Terneuzen); JHLM van Groenendael (Franciscus Hospital, Roosendaal); AL Huidekoper (Bronovo Hospital, The Hague); SM van der Kooij (Haga Hospital, The Hague); ETH Molenaar (Groene Hart Hospital, Gouda); AJ Peeters (Reinier de Graaf Gasthuis, Delft); N Riyazi (Haga hospital, The Hague); HK Ronday (Haga hospital, The Hague); AA Schouffoer (Haga Hospital, The Hague); PBJ de Sonnaville (Admiraal de Ruyter Hospital, Goes); I Speyer (Bronovo Hospital, The Hague); the authors would also like to thank all other rheumatologists and trainee rheumatologists who enrolled patients in this study, and all research nurses for their contributions.
References
Footnotes
Contributors GA performed the statistical analysis, interpreted the data and drafted the manuscript. MKV, LH, KVCW-dB, YPMG-R, MvO, JBH, CB, GMS-B, LRL and LAT contributed to the acquisition of data and revision of the manuscript. TH participated in the study design, contributed to the acquisition of data and was involved in revising the manuscript. CFA participated in the study design, contributed to the acquisition of data, and was involved in the analysis and interpretation of the data, and helped to draft the manuscript. All authors read and approved the final version of the manuscript.
Funding This work was financially supported by AbbVie in the first year of the IMPROVED study. Study design, trial management, data collection, data analysis and interpretation, and preparation of the manuscript were performed by the authors without input from the sponsor. The work of Dr Trouw was supported by a ZON-MW Vidi grant and a fellowship from Janssen-biologicals.
Competing interests None declared.
Patient consent Obtained.
Ethics approval The medical ethics committees of all participating centres approved the study protocol and all patients gave written informed consent.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement GA had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. The data is from a full database of the IMPROVED study. Additional unpublished data are not available.