Article Text

Abstract
Background Spondyloarthritis (SpA) is a heterogeneous disease with hardly predictable potential courses. We aimed at determining prognostic factors of bad functional outcome at 2 years in patients with early inflammatory back pain (IBP).
Methods Data from patients included in the French multicentre devenir des spondylarthropathies indifférenciées récentes (DESIR) cohort, that is, suffering from IBP starting before 50 years of age and lasting for 3–36 months, were used. A bad functional outcome at 24 months was defined as an increase in bath ankylosing spondylitis functional index (BASFI), or BASFI at 2 years higher than the 75th centile in the cohort. Demographic, clinical, biological and radiological data collected at inclusion were compared in patients with bad functional outcome versus others, by χ2 test, then by a multivariate logistic regression model with stepwise selection of relevant factors.
Results 513 patients (54.4% females, 72.2% fulfilling ASAS criteria) were assessed. Of those, 130 (25.3%) fulfilled the aforementioned criteria of a bad functional outcome (BASFI increase ≥4 units or ≥36 at 2 years). Multivariate analysis revealed that not fulfilling ASAS criteria, female sex, age >33 years, lower educational level, active smoking status and high disease activity according to bath ankylosing spondylitis disease activity index (BASDAI) at baseline were independently associated with a bad functional outcome at 24 months. Sensitivity analyses restricted to patients fulfilling ASAS criteria for SpA resulted in similar results.
Conclusion We observed, in a large prospective cohort of patients with early IBP, formerly described bad prognostic factors, especially a low educational level, an older age and a high disease activity at onset, and revealed that active smoking status and female sex were also independently associated with a poor outcome. Fulfilment of ASAS criteria, on the other hand, was predictive of a better outcome, most likely due to the more consensual management of a defined disease.
- Spondyloarthritis
- Epidemiology
- Patient perspective
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Spondyloarthritis is a heterogeneous disease with a hardly predictable course. It can affect global health by many aspects, from purely subjective symptoms like pain or fatigue to objective inflammatory processes in the spine, joints, eyes, skin or gut.
What does this study add?
Focusing on patients with inflammatory back pain of recent onset and the evolution of their functional ability over the first months of disease, we revealed that several factors had a significant prognostic value and may predict a bad outcome, especially female gender, age over 33, lower educational level, active smoking status and initially high disease activity. Not fulfilling currently applied criteria for spondyloarthritis (assessment of spondyloarthritis (ASAS)) was also related to a bad functional outcome at 2 years.
How might this impact on clinical practice?
Pointing out several factors that might predict an unfavourable outcome from the patient perspective could help rheumatologists identify a patient showing a pattern of characteristics resembling the ‘unfavourable patient profile’.
Introduction
Spondyloarthritides (SpAs) are chronic inflammatory disorders encompassing different rheumatic diseases which share a common core of symptoms, with a variable presentation and association of axial, peripheral and extra-articular signs and symptoms.
Defining the severity of the disease remains a hard and debated task, and predicting it remains hazardous, as the disease course is usually made of successive inflammatory flares which in some patients can lead to limited spinal mobility, destructive peripheral arthritis or severe organ involvement, especially of the gut or eyes. Globally, it is estimated that roughly about 10% of the patients will suffer from a severe form of the disease, although this proportion may vary a lot, depending on the definition that will be used to define the severity itself.
Severity can thus be defined on the basis of global health status indicators like morbidity or mortality, assessments of functional status, quality-of-life scales, degree of spinal mobility impairment, radiographic degradation, and involvement of large joints (especially the hip) and of extra-articular organs (eyes, gut, heart, etc). Severity can also be appreciated by the patient himself: indeed, a more pragmatic approach of severity can be derived from results of several patient-reported outcomes (PROs), as they present the major advantage of combining and synthesising all potential impacts of the disease that play a negative role on perceived health status into a single and easily collected value. In particular, specific instruments developed in SpA focus on the limitations in several daily activities that are usually impaired by the disease, and summarise the reported abilities of the patient as a functional score or index. Despite several metrological limitations, the most used instrument in this domain is bath ankylosing spondylitis functional index (BASFI), which consists of the mean value of reported abilities in accomplishing 10 basic daily life tasks, each ranging from 0 (no difficulty) to 10 (impossible).1 It is then considered that the obtained value reflects the degree of functional impairment in a patient that is caused by the disease, assuming that most potential limitations have no alternative origin in that patient. Thus, it might be globally considered that a persistently severe functional impairment as reflected by a bad result in the reported BASFI does reflect either an unfavourable course of the disease, which caused any of the articular or extra-articular manifestations, or on the other hand can alternatively be due to a bad appreciation of his health status by the patient, despite the fact that no objectively severe symptom of SpA is present, because other factors (comorbidities) have led to a poor perceived health status. In any of these situations (severe disease with organic functional impact or benign disease with obvious functional disorders), and those consisting of an association of inflammatory processes, other musculoskeletal disorders and psychological consequences of the chronic illness all leading to altered perceived health, the patient will remain in an uncomfortable situation, and the SpA will be considered severe, at least by the patient himself.
Since detecting those patients at risk of an unfavourable course might require specific attention and management, we aimed at evaluating which characteristics of the disease at an early stage of development might be associated with such a bad perceived outcome.
Methods
Data from patients included in the French multicentre devenir des spondylarthropathies indifférenciées récentes (DESIR) cohort, that is, suffering from inflammatory back pain (IBP) due to a probable axial SpA, starting before 50 years of age and lasting for between 3 months and 3 years, were evaluated in this study.2 The data set used for this analysis was locked on 3 December 2012. The primary outcome, that is, presence of a bad functional outcome, was defined as an increase in BASFI superior to the 75th centile of observed progression in the cohort from the inclusion visit to the 24-month assessment, or BASFI at 2 years higher than the 75th centile of observed values at this latter time point.
Primary objective
Applying the given definition of severity to patients at the time of the 24-month visit, influence or association of baseline characteristics collected at the inclusion visit on this outcome was evaluated. Formerly published factors potentially influencing the disease course were tested, as well as others which we thought might play a role in the context.
Sociodemographic data: gender, age, educational level;
Clinical data: presence or history of peripheral arthritis, history of uveitis, smoking status;
Biological data: presence of the HLA-B27 gene, raised acute phase reactants (estimated sedimentation rate (ESR)>28 mm, C reactive protein (CRP) above normal level);
Disease activity as assessed by bath ankylosing spondylitis disease activity index (BASDAI)3 or ankylosing spondylitis activity score (ASDAS)CRP;4
Radiological data: presence of sacroiliitis on MRI or X-rays as reported by the local investigator, baseline modified Stoke ankylosing spondylitis spinal score (mSASS) ≥0.5 (average value of 2 central readers, ie, at least 1 reader scoring any abnormality).
As a sensitivity analysis, we also conducted the same analyses in a restricted population of patients fulfilling assessment of spondyloarthritis (ASAS) criteria for axial SpA at inclusion time.5
Statistical analyses
Baseline characteristics of the patients were described and analysed in order to compare the two defined groups of patients, that is, those having a ‘bad functional outcome’ versus others ‘not fulfilling the formerly defined definition of bad functional outcome’.
Bivariate analyses were conducted to compare distribution or values of assessed variables between the two defined groups of patients (with vs without disease severity characteristics). χ2 (or Fisher's exact tests if required) was used for categorical variables, after dichotomisation according to the observed median value or clinically relevant cut-offs if applicable for continuous variables. Factors showing a potential association with disease severity (p<0.2 in bivariate analysis) were included in a multivariate model, aiming at evaluating their potentially independent value in predicting a more severe outcome in patients with early SpA. A logistic regression model, with stepwise inclusion of variables, was applied to test the predictive value of formerly described factors, with disease severity being used as the dependent variable in the model.
Results
Five hundred and thirteen patients (54.4% females mean age at inclusion visit 34±8.8 years, 72.2% fulfilling ASAS criteria) were included in this study. The remaining patients could not be included because of missing data for BASFI at baseline and/or 24 months visits. The characteristics of the 2 groups were similar, except for the proportion of smoking patients that was higher in the ‘excluded group’ ((53.9% vs 34.7%), and regarding the educational level (less patients with a level higher than college in the excluded group: 52.5% vs 61.8%)).
Of those, 130 (25.3%) fulfilled the aforementioned criteria of a bad functional outcome (with a BASFI increase of at least 4 units or value at 2 years ≥36 on a 100 units scale; figure 1).

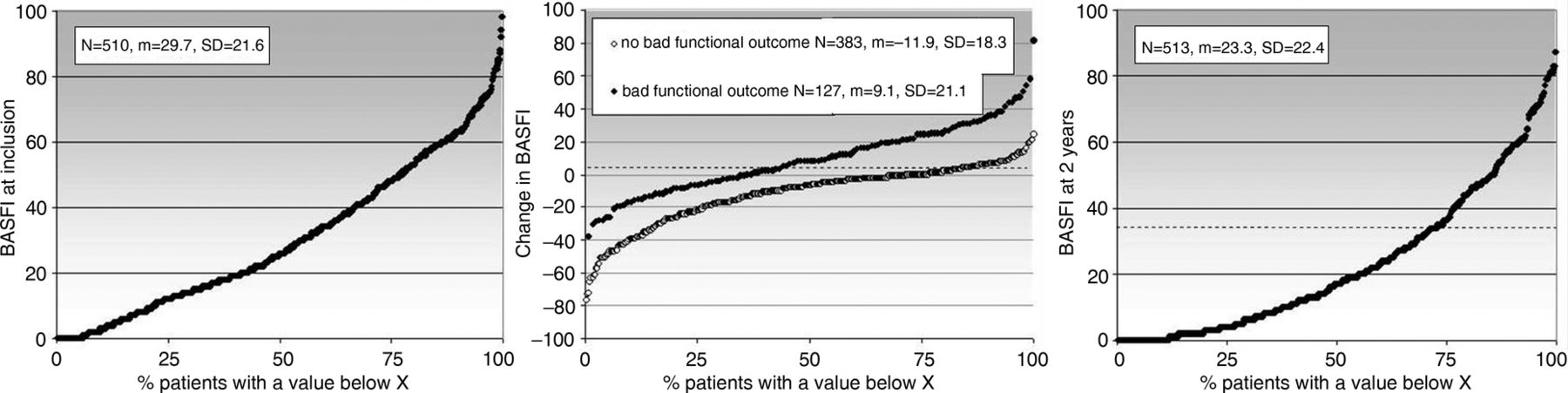{kind=link}
Probability plots of observed values of BASFI at inclusion and at the 2-year follow-up visit, and of change scores over this time period.
A bad outcome was more frequently observed in the subgroup of ‘older’ patients, that is, aged over 33 years at disease onset, or with an educational level lower than college (both p<0.0001). Smoking (p<0.001), female sex (p<0.008) and a high disease activity at baseline (ASDASCRP>3.5 and BASDAI>45) were also associated with a bad functional outcome (p<0.0001; table 1).
Analysis of the association between baseline characteristics of the patients and presence of a bad functional outcome at the 2-year follow-up visit
Patients not fulfilling ASAS criteria or HLA B27−, having normal X-rays or MRI of sacroiliac joints, and with a history of active peripheral arthritis were also more prone to have poor functional outcome (all p<0.05).
Multivariate analysis revealed that not fulfilling ASAS criteria, female sex, age >33 years, a lower educational level, an active smoking status and a high disease activity according to BASDAI at baseline were independently associated with a bad functional outcome at 24-month follow-up (table 2).
Predictive factors of a bad functional outcome at the 2-year follow-up visit (results of multivariate analysis)
When focusing on patients fulfilling ASAS criteria at the baseline visit only (N=490, with 369 patients having available BASFI at inclusion and/or 24-month visits to determine the outcome), the distribution of BASFI and its evolution over the first 2 years were similar: on the basis of the same distribution-based definition of bad functional prognosis, the cut-offs were defined as having a change ≥3 points or BASFI at 2 years ≥34, which was the case for 140/369 patients (121 missing values). The results of the multivariate analysis were similar in this restricted population, with a higher likelihood of poor functional evolution in female patients having a higher disease activity at the inclusion visit, although the ASDASCRP showed a better discriminatory ability in this population of patients fulfilling classification criteria than BASDAI (table 3).
Predictive factors of a bad functional outcome at the 2-year follow-up visit (results of multivariate analysis, restricted to patients fulfilling ASAS criteria)
Again, active smoking had a negative impact on perceived health as assessed by reported functional ability, while higher educational level showed a protective effect. Age, however, had no significant impact (despite a median age in this subpopulation of 32.5 years, ie, identical to the entire DESIR cohort). As a sensitivity analysis, we repeated the analysis in the ASAS+cohort with the outcome defined by the cut-off values derived from the entire DESIR cohort (change in BASFI ≥4 or BASFI at 24 months ≥36), and the results of the logistic regression were very similar, except for baseline ASDASCRP ≥3.1 that did not reach statistical significance anymore (p=0.054; data not shown).
Discussion
In summary, we observed that a bad perceived health status as approached by the functional status in patients with early IBP was significantly more likely to occur in women, if no definite diagnosis of SpA had been made according to ASAS classification criteria,5 and when self-reported activity of the disease was high at onset. Active smoking status might also be associated with a degraded functional evolution. Younger patients and those with a higher level of instruction, on the other hand, were found to less frequently show this pattern in the early course of their disease.
In formerly reported studies on this issue, functional impairment, as measured by BASFI, was already found to be correlated with a lower instruction level, smoking, associated comorbidities, a physically demanding job and active smoking status.6 Doran et al7 showed an association of BASFI with initial radiographic status (as measured by BASRI), high disease activity (assessed with BASDAI) and smoking status. On the basis of health assessment questionnaire for the spondyloarthropathies (HAQ-S), Ward et al6 found that functional impairment over time was increased with ageing, active smoking status and absence of social support. Regular physical exercising and good social support, on the other hand, were associated with decreased functional impairment of the patients.8
This work has several strengths that can be pointed out; in particular, it allows a global insight into the pattern of distribution of PROs (BASFI here), in a population of patients with recent IBP. Despite the fact that a certain homogeneity of patients could have been expected in this context of similar symptoms and ancientness, it is remarkable how extremely heterogeneous the reported functional impact is either present, or perceived and reported by the patients. Indeed, the use of BASFI, a purely subjective questionnaire, to define our main outcome, that is, changes in functional impairment over the first 2 years of the disease management, needs also to be discussed: in the context of recent axial SpA, using PROs has the advantage over physician-derived assessments of capturing most relevant information of the disease, as many of these patients have important symptoms and significant impairment of health quality while objective signs or clinical findings remain poor, if not absent.9 Our definition of the bad functional outcome was defined on the basis of an arbitrary choice of cut-offs in observed values of BASFI. We, indeed, aimed at discriminating these patients with outlying results in comparison to the global sample, but with a sufficient number of participants required to conduct statistical analyses appropriately, and the 75th centiles were chosen in this context. On the other hand, some limits need also to be acknowledged, especially the fact that independent comorbidities might play a crucial role in the level of background functional ability in a patient, as well as on its appreciation. The design and inclusion criteria of the cohort, as well as the usually short symptom duration in patients included in the DESIR cohort, however, make this situation quite unlikely: indeed, these young patients are unlikely to have other musculoskeletal disorders like major degenerative lesions or osteoarthritis, and their main symptom, namely IBP, has been considered by the rheumatologist to be related to a probable SpA before the patient was considered eligible for inclusion in the DESIR cohort. Other comorbidities that might very well be associated in this context like depression or fibromyalgia, however, cannot be ruled out. This latter situation by the fact might also explain part of another finding in our work, that not fulfilling ASAS criteria for SpA increases the likelihood of showing a bad functional prognosis over the first months of follow-up. Indeed, an alternative aetiology to explain IBP might be present, in which therapeutic interventions have a clearly less marked impact than what is usually observed in axial SpA. The possibility of another diagnosis, especially fibromyalgia, in this context of recent symptoms, is a potential explanation of this observation. Another potential reason for these results might be related to the availability of effective treatments in case of established disease (eg, education, physiotherapy, non-steroidal anti-inflammatory drugs, biologics) and the lack of these therapies in non-established disease, such as in the case of IBP without other clinical symptoms suggestive of SpA and/or without obvious imaging abnormalities at the sacroiliac joint level.
The impact of a biological treatment on the function of patients is of course of major interest. We, however, chose to not include therapeutic interventions in our analyses because they cannot be regarded as prognostic factors by definition, since they are based on baseline characteristics of patients as well as observations made along the follow-up. In addition, introduction of an antitumour necrosis factor (TNF) drug mainly reflects the confidence in the diagnostic of SpA, and the appraisal of activity/severity of the disease, which are respectively approached by the variables ‘ASAS criteria, HLA B27, MRI sacroiliitis’ and ‘ASDAS, BASDAI, CRP, ESR, etc’, which we took into account and tested in our analyses. When formally testing this assumption, and the influence of an anti-TNF treatment on functional outcome, we found a statistically significant association in univariate analysis: 75/348 (21.6%) patients having not received a biological treatment over the first 2 years of follow-up had a bad functional outcome as described in our analyses, while 55/165 (33.3%) did so in the group of patients who had been treated in this time period (p=0.003). However, when we tested the influence of including the variable ‘having been treated by an anti-TNF during the first 2 years of follow-up’ in the final model of logistic regression, this variable had no independent association with the outcome (p=0.52), which confirms that the decision of starting an anti-TNF drug was made on the basis of information that was already captured by the variables we have found in the final model of the main analysis.
Most factors that were found to be associated with a bad reported functional outcome are non-modifiable, meaning that except the fact that a physician could be more attentive to a patient showing a pattern of characteristics resembling the ‘unfavourable patient profile’, no direct relevant specific action can be made. Our interpretation of the results is that more attention should be paid to a patient having, in the context of IBP of recent onset, a similar ‘profile’ to what was revealed by our analyses. This does not necessarily mean a more intensive treatment (which will be limited by the fact that this patient does probably not fulfil diagnostic criteria for SpA and will not be eligible for intensive drug therapy like TNF blocking agents), but this might encourage a more periodic evaluation and adjustment of therapeutic interventions (physiotherapy, painkillers, education, self-management strategies, etc) whenever this is possible. It could also be advised that the persistency of functional symptoms in the absence of inflammatory signs in a patient should systematically raise the possibility of a differential or additional diagnosis, especially fibromyalgia. In addition, we found that, likewise, in many other diseases, active smoking status has a clear impact on the outcome, meaning that encouraging smoking cessation should be recommended in this population of patients with a global and cardiovascular objective, as well as to optimise the chance of achieving a good clinical prognosis. The association of smoking status and prognosis in patients with SpA has already been reported in numerous publications, with an impact on disease onset, clinical, biological and radiological activity and prognosis.10 Female sex, however, usually considered as a protective factor in ankylosing spondylitis (AS) with regard to stringent outcomes like loss in spinal mobility, development of coxitis or extra-articular manifestations of the disease, was related to a poorer functional outcome after 2 years of follow-up when self-assessed functional status was considered.11
In conclusion, we determined, in a large prospective cohort of patients with early IBP, bad prognostic factors that had formerly been reported in established AS, especially low educational level, older age and high disease activity at onset, and revealed that an active smoking status was also independently associated with poor outcome. Fulfilment of ASAS criteria, on the other hand, was predictive of better outcome, most likely due to more consensual management of a clearly defined disease.
Acknowledgments
The DESIR cohort is conducted under the control of Assistance Publique-Hopitaux de Paris via the Clinical Research Unit Paris-Centre and under the umbrella of the French Society of Rheumatology and INSERM (Institut National de la Santé et de la Recherche Médicale). The database management is performed within the department of epidemiology and biostatistics (Professor Paul Landais, DIM, Nîmes, France). The authors thank the different regional participating centres: Professor Maxime Dougados (Paris—Cochin B), Professor André Kahan (Paris—Cochin A), Professor Olivier Meyer (Paris—Bichat), Professor Pierre Bourgeois (Paris—La Pitié-Salpetrière), Professor Francis Berenbaum (Paris—Saint Antoine), Professor Pascal Claudepierre (Créteil), Professor Maxime Breban (Boulogne Billancourt), Dr Bernadette Saint-Marcoux (Aulnay-sous-Bois), Professor Philippe Goupille (Tours), Professor Jean-Francis Maillefert (Dijon), Dr Xavier Puéchal (Le Mans), Professor Daniel Wendling (Besançon), Professor Bernard Combe (Montpellier), Professor Liana Euller-Ziegler (Nice), Professor Philippe Orcel (Paris—Lariboisière), Professor Pierre Lafforgue (Marseille), Dr Patrick Boumier (Amiens), Professor Jean-Michel Ristori (Clermont-Ferrand), Dr Nadia Mehsen (Bordeaux), Professor Damien Loeuille (Nancy), Professor René-Marc Flipo (Lille), Professor Alain Saraux (Brest), Professor Corinne Miceli (Le Kremlin Bicêtre), Professor Alain Cantagrel (Toulouse), Professor Olivier Vittecoq (Rouen).
References
Footnotes
Contributors CL and BC were involved in conception and design. CL, BC and MD were involved in analysis and interpretation of data. CL was involved in drafting the manuscript. BC and MD were involved in critical revision of the manuscript for important intellectual content. CL was involved in statistical analysis.
Funding The DESIR cohort is financially supported by unrestricted grants from the French Society of Rheumatology and Pfizer, France.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Approval from Ethics Committee obtained within the DESIR cohort project.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.