Article Text

Abstract
Objective To investigate which structural MR abnormalities discriminate symptomatic knee osteoarthritis (OA), taking co-occurrence of abnormalities in all compartments into account.
Methods The Netherlands Epidemiology of Obesity (NEO) study is a population-based cohort aged 45–65 years. In 1285 participants (median age 56 years, 55% women, median body mass index (BMI) 30 kg/m2), MRI of the right knee were obtained. Structural abnormalities (osteophytes, cartilage loss, bone marrow lesions (BMLs), subchondral cysts, meniscal abnormalities, effusion, Baker's cyst) at 9 patellofemoral and tibiofemoral locations were scored following the knee OA scoring system. Symptomatic OA in the imaged knee was defined following the American College of Rheumatology criteria. Logistic ridge regression analyses were used to investigate which structural abnormalities discriminate best between individuals with and without symptomatic OA, crude and adjusted for age, sex and BMI.
Results Symptomatic knee OA was present in 177 individuals. Structural MR abnormalities were highly frequent both in individuals with OA and in those without. Baker's cysts showed the highest adjusted regression coefficient (0.293) for presence of symptomatic OA, followed by osteophytes and BMLs in the medial tibiofemoral compartment (0.185–0.279), osteophytes in the medial trochlear facet (0.262) and effusion (0.197).
Conclusions Baker's cysts discriminate best between individuals with and without symptomatic knee OA. Structural MR abnormalities, especially in the medial side of the tibiofemoral joint and effusion, add further in discriminating symptomatic OA. Baker's cysts may present as a target for treatment.
- Epidemiology
- Knee Osteoarthritis
- Magnetic Resonance Imaging
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Structural abnormalities in the knee joint assessed by MRI are frequent in individuals with and without symptomatic osteoarthritis (OA).
What does this study add?
Co-occurrence of all structural abnormalities in all compartments of the knee was taken into account when investigating which abnormalities can best discriminate between individuals with and without symptomatic OA.
Baker's cysts discriminate best between individuals with and without symptomatic OA. Structural MR abnormalities, especially in the medial side of the tibiofemoral joint and effusion, add further in discriminating symptomatic OA.
How might this impact on clinical practice?
The presence of Baker's cysts may especially present as a target for treatment.
Introduction
The knee joint is composed of three compartments: the medial and lateral tibiofemoral compartments and the patellofemoral compartment. Research in knee osteoarthritis (OA) focused mainly on the tibiofemoral joint,1 although OA can occur in all these compartments, either isolated or concurrent.2 OA in all compartments has been related to symptoms as pain and disability.3 ,4 However, the underlying relationships and attributions of osteoarthritic abnormalities in the different compartments to symptoms in OA are incompletely understood.
The knee joint comprises bone, cartilage, menisci and synovial tissue. Structural abnormalities have been observed in all these joint tissues, increasing with age.5 These structural abnormalities are not specific for OA, since they have also been observed in persons without OA.6–9 Clinical or symptomatic OA is classified on the basis of the presence of pain, clinical characteristics and abnormalities observed during physical examination,10 but which structural abnormalities contribute to symptoms and whether and which structural abnormalities can discriminate symptomatic OA is not clear.
Previous studies on the association between structural abnormalities, such as bone marrow lesions (BMLs), synovitis or cartilage defects, and symptoms in OA showed conflicting results; while some studies found an association between these structural abnormalities and OA symptoms, other did not.11–14 These discrepancies could be caused by the co-occurrence of structural abnormalities in different tissues, but it may all have resulted from the analyses, which were univariate or limited multivariate analyses, not adjusting for all tissue abnormalities in all joint locations.
Therefore, this study investigates which specific structural abnormalities in all compartments of the knee as assessed by MRI can best discriminate between individuals with and without symptomatic OA within the same knee, using a model that takes co-occurrence of all abnormalities into account.
Patients and methods
Study design and study population
The Netherlands Epidemiology of Obesity (NEO) study is a population-based prospective cohort study including 6671 individuals aged 45–65 years, with an oversampling of persons with overweight or obesity. Detailed information about the study design and data collection has been described elsewhere.15 In short, men and women between 45 and 65 years with a self-reported body mass index (BMI) of 27 kg/m2 or higher living in the greater area of Leiden were eligible to participate. In addition, all inhabitants aged 45–65 years from one municipality (Leiderdorp) were invited irrespective of their BMI.
All participants completed questionnaires on demographic and clinical data and visited the NEO study centre for several baseline measurements, including measurement of weight (kg) and height (cm) to calculate the BMI (kg/m2), and an extensive physical examination. A random sample of 1285 study participants without contraindications (metallic devices, claustrophobia, body circumference >170 cm) underwent MRI of the right knee. The present study is a cross-sectional analysis of baseline measurements of these 1285 participants. The study was approved by the medical ethics committee of the Leiden University Medical Center and all participants gave written informed consent.
Magnetic resonance image
MRI was performed using a dedicated knee coil in a 1.5T system (Philips, Medical Systems, Best, The Netherlands). Our standardised scanning protocol consisted of1 Coronal proton density (PD) turbo spin echo (TSE), repetition time (TR)/echo time (TE) 2335/35 ms; echo train length (ETL) 6,2 coronal frequency selective fat-suppressed PD TSE (TR/TE 2334/35 ms; ETL 6, 3 mm slice thickness);3 sagittal PD TSE (TR/TE 2338/35; ETL 6; 3.5 mm slice thickness);4 sagittal frequency selective fat-suppressed T1-weighted three-dimensional gradient echo sequence (TR/TE 11/5.5; 25° flip angle; 150 mm field of view, 272×512 acquisition matrix, 2 mm slice thickness with a 1 mm overlap between images);5 axial frequency selective fat-suppressed PD TSE (TR/TE 3225/15; ETL 6, 4 mm slice thickness). In all TSE sequences, we used a 150–160 mm field of view and a 304×512 acquisition matrix. Total acquisition time, including the initial survey sequence, was 30 min.
Scoring of MRI
A trained reader (AWV, supervised by JLB) used the validated semiquantitative knee OA scoring system blinded to clinical data.16 Presence or absence of osteophytes, cartilage loss, subchondral BMLs and subchondral cysts was scored at the following locations: patellar crest, medial and lateral patellar facet, medial and lateral trochlear articular facet, medial and lateral femoral condyle and medial and lateral tibial plateau.
Osteophytes were defined as focal bony excrescences, extending from a cortical surface and measured from base to tip, graded 0 (absent), 1 (<3 mm), 2 (3–5 mm) or 3 (5 mm).
Cartilage loss was graded 0 (absent), 1 (<50% reduction), 2 (≥50% reduction) or 3 (full-thickness cartilage loss).
BMLs were defined as ill-defined areas of increased signal intensity on T2-weighted images in the subchondral bone extending away from the articular surface and graded 0 (absent), 1 (diameter <5 mm), 2 (5 mm–2 cm) or 3 (>2 cm).
Subchondral cysts were defined as well-defined foci of high signal intensity on T2-weighted images in the subchondral bone and graded on the basis of their measured greatest dimension as 0 (absent), 1 (<3 mm), 2 (3–5 mm) or 3 (>5 mm). Both BMLs and cysts were required not to be associated with meniscal or ligamentous attachments.
The menisci were reviewed for presence of subluxation, maceration and degenerative tears. Subluxation was defined as protrusion over the tibial plateau edge and graded 0 (absent), 1 (<1/3 meniscal width bulging), 2 (1/3–2/3 bulging) or 3 (>2/3 involved). Maceration was defined as an intrameniscal focus of intermediate signal intensity and graded 0 (absent), 1 (a small, central focus in meniscus), 2 (intrameniscal focus surrounded by a broad, hypointense peripheral rim) or 3 (a thin, hypointense peripheral rim outlining the intrameniscal focus). Tears were defined as regions of intermediate signal intensity within the meniscus, communicating with the surface or inner margin on more than one section, graded 0 (absent) or 1 (present).
Joint effusion was graded 0 (a small physiological sliver of synovial fluid), 1 (a small amount of fluid distending 1 or 2 joint recesses), 2 (>2 joint recesses partially distended), or 3 (full, marked distention of all joint recesses).
A Baker's cyst was defined when a circumscribed mass with intermediate signal intensity on PD-weighted and high signal intensity on T2-weighted dual SE sequences was observed, originating from the dorsomedial tibiofemoral joint space. Baker's cysts were graded 0 (absent), 1 (minimal), 2 (moderate) or 3 (severe).
A random 10% of the MRI (n=120) were scored twice to test the reproducibility; intraclass correlation coefficients were for meniscal maceration 0.61, meniscal tear 0.87, meniscal subluxation 0.93, cyst 0.64, BML 0.93, cartilage loss 0.90, osteophytes 0.97.
Symptomatic knee OA
Self-reported pain and morning stiffness were measured using standardised questionnaires. Physical examination of both knee joints was performed by trained research nurses, using a standardised scoring form. OA was defined on the basis of the clinical criteria of the American College of Rheumatology as presence of pain on most days of the prior month and at least three of the following criteria:1 age >50 years,2 stiffness <30 min duration,3 crepitus on active motion,4 bony tenderness,5 bony enlargement,6 no palpable warmth.10
Statistical analysis
Data were analysed using SPSS V.20 (SPSS Inc, Chicago, Illinois, USA), Matlab version R2014a (MathWorks, Natick, Massachusetts, USA) and R V.3.0.1 (R foundation; http://www.r-project.org).
The prevalence of structural abnormalities was analysed in the total study population and stratified by symptomatic OA status. The relation between different structural abnormalities was visualised by network graphs, constructed using R (package ‘glasso’), by estimating a sparse inverse covariance matrix using a lasso (L1) penalty. The basis for the graphical lasso calculation was the pooled variance–covariance matrix across both outcome groups (individuals with and without symptomatic OA).
To investigate which specific abnormalities discriminate best between individuals with and without symptomatic OA, the following analyses were performed including all structural abnormalities graded 0–3 (only meniscal tears were graded 0/1).
Since the number of individuals without symptomatic OA was much higher than the number of OA cases, we split the set of individuals without OA into three parts and repeated the subsequently described model analysis for each of these three parts to assess stability of computations. Individuals without OA were randomly assigned to three mutually exclusive sets; each of these sets was then combined with the OA cases, rendering three calibration sets. The subsequently described discriminant analysis was then applied (repeated) for each of these sets. A logistic ridge regression model (see Hastie et al17 for description) was fitted to each of the above constructed calibration sets using a double cross-validatory approach.18 The double cross-validatory approach provides unbiased class probabilities for each individual in each of the above three calibration sets. Cross-validated deviances were used to select optimal models within the double cross-validatory assessment. Receiver-operating characteristic curves, area under the curve (AUC) and classification statistics were used to summarise the double cross-validatory classifications. Double cross-validation uses a separate model fit for each left-out datum to generate unbiased classification summaries. For model parameter interpretation, we therefore refitted the logistic ridge regression model to the calibration data, using the optimum shrinkage (penalty) term identified in the preceding double cross-validatory calculation. Regression coefficients for all assessed structural abnormalities in the different locations within the joint were calculated on the basis of this final fitted model. Penalised estimates such as those provided by ridge regression reduce variance of estimation by allowing for bias in the estimation of the effects, which implies that classical estimates of the variance of these estimates can no longer be meaningfully interpreted.
Both crude analyses and analyses adjusted for age, sex and BMI were performed. Higher regression coefficients reflect better discrimination between presence or absence of symptomatic OA, taking co-occurrence of all abnormalities into account.
Results
Population characteristics
After exclusion of individuals with missing data of physical examination (n=1), data from 1284 participants were analysed. Of the studied individuals, 55% were women. Median age was 56 years (IQR 50–61), median BMI 30.0 kg/m2 (27.9–33.0). Symptomatic OA in the imaged knee was present in 177 individuals. The 1107 individuals without symptomatic OA were divided into three mutually exclusive sets of 369 individuals for further analyses.
Prevalence of structural MR abnormalities
The prevalence of structural abnormalities in the total study population is presented in table 1. All assessed structural abnormalities except for subchondral cysts were observed frequently. However, the prevalence differed across locations within the joint.
Prevalence of structural abnormalities as assessed on MRI on different locations in the knee in the total NEO study population
In the tibiofemoral and patellofemoral compartment, osteophytes were commonly observed, especially in the medial tibiofemoral compartment (medial femoral condyle 86%, medial tibial plateau 38%) and the medial patellar facet (59%). Cartilage defects were also frequently observed in both compartments, especially medially (medial femoral condyle 58%, medial tibial plateau 68%, medial patellar facet 65%, medial trochlear facet 53%) and in the patellar crest (65%). BMLs were observed less frequently, mostly located in the patellar crest (22%).
Meniscal abnormalities were observed most commonly in the medial meniscus; maceration was most prevalent (35%), followed by tears (23%) and subluxation (15%).
As presented in table 2, a higher prevalence of osteophytes, cartilage defects, BMLs and meniscal abnormalities were seen in individuals with symptomatic OA as compared to individuals without.
Prevalence of structural abnormalities as assessed on MRI on different locations in the knee stratified by symptomatic knee OA status
Effusion was also highly prevalent (80%), in individuals with and without symptomatic OA. Higher grades of effusion were especially observed more often in individuals with symptomatic OA than in those without. The same was observed for Baker's cysts (overall prevalence 30%); grade 2 and grade 3 were especially observed most often in individuals with OA.
Relation between structural abnormalities
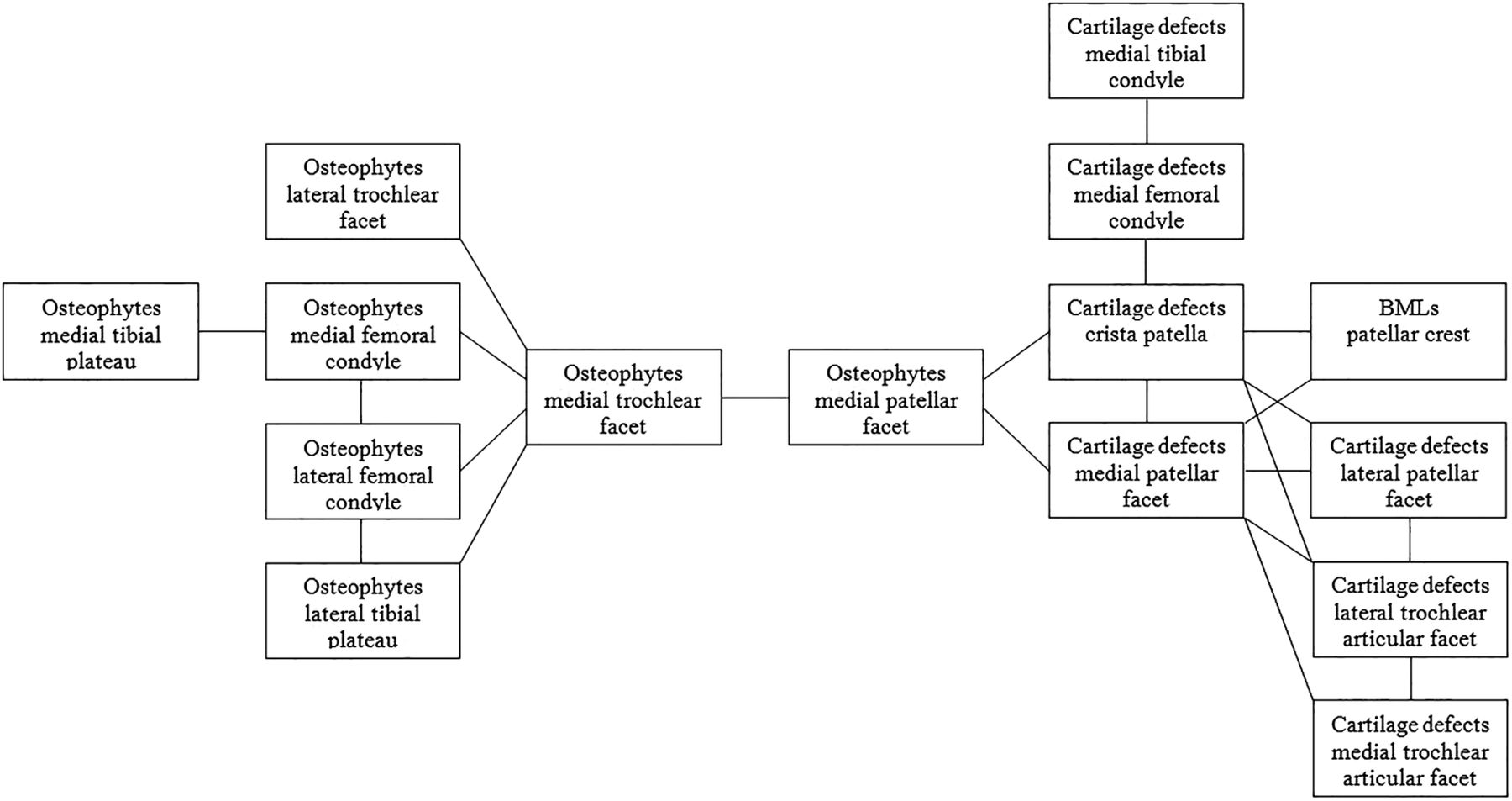
In the total study population, including individuals with and without symptomatic OA, the relation between structural abnormalities was visualised by network graphs, showing multiple relations between abnormalities on different locations within the joint. A number of network graphs were performed, the number of relations shown in the graph depending on the used lasso penalty. All network graphs showed relations between osteophytes on different locations within all compartments of the knee and between cartilage defects on different locations. Furthermore, osteophytes and cartilage defects within the same compartment were also related. Figure 1 shows 15 structural abnormalities with 22 relations between them. Besides osteophytes and cartilage defects at different locations within the joint, BMLs in the patellar crest were present in the network graph, related to cartilage defects in the patellar crest and medial patellar facet.

Network graph illustrating the relation between the assessed structural abnormalities on different locations within the knee joint in the total NEO study population. Lines represent a relation between the presence of two abnormalities. BMLs, bone marrow lesions; NEO, the Netherlands Epidemiology of Obesity study.
Structural abnormalities discriminating symptomatic OA
Next, we investigated which specific abnormalities could best discriminate between individuals with and without symptomatic OA, taking co-occurrence of all abnormalities into account.
Regression coefficients of the assessed structural abnormalities for presence of OA as obtained by logistic ridge regression analyses are listed in table 3. Depicted are regression coefficients for all three analyses sets and a mean regression coefficient for these sets. The higher the regression coefficient, the better the corresponding structural abnormality discriminates symptomatic OA, adjusted for co-occurrence of abnormalities. The regression coefficients for subchondral cysts were all below 0.030.
Regression coefficients for presence of symptomatic knee OA as obtained by logistic ridge regression analyses
Baker's cysts showed the highest regression coefficient for OA, followed by osteophytes in the medial tibial plateau and medial trochlear facet. The next strongest regression coefficient was found for effusion, followed by BMLs in the medial tibiofemoral compartment and osteophytes in the medial femoral condyle.
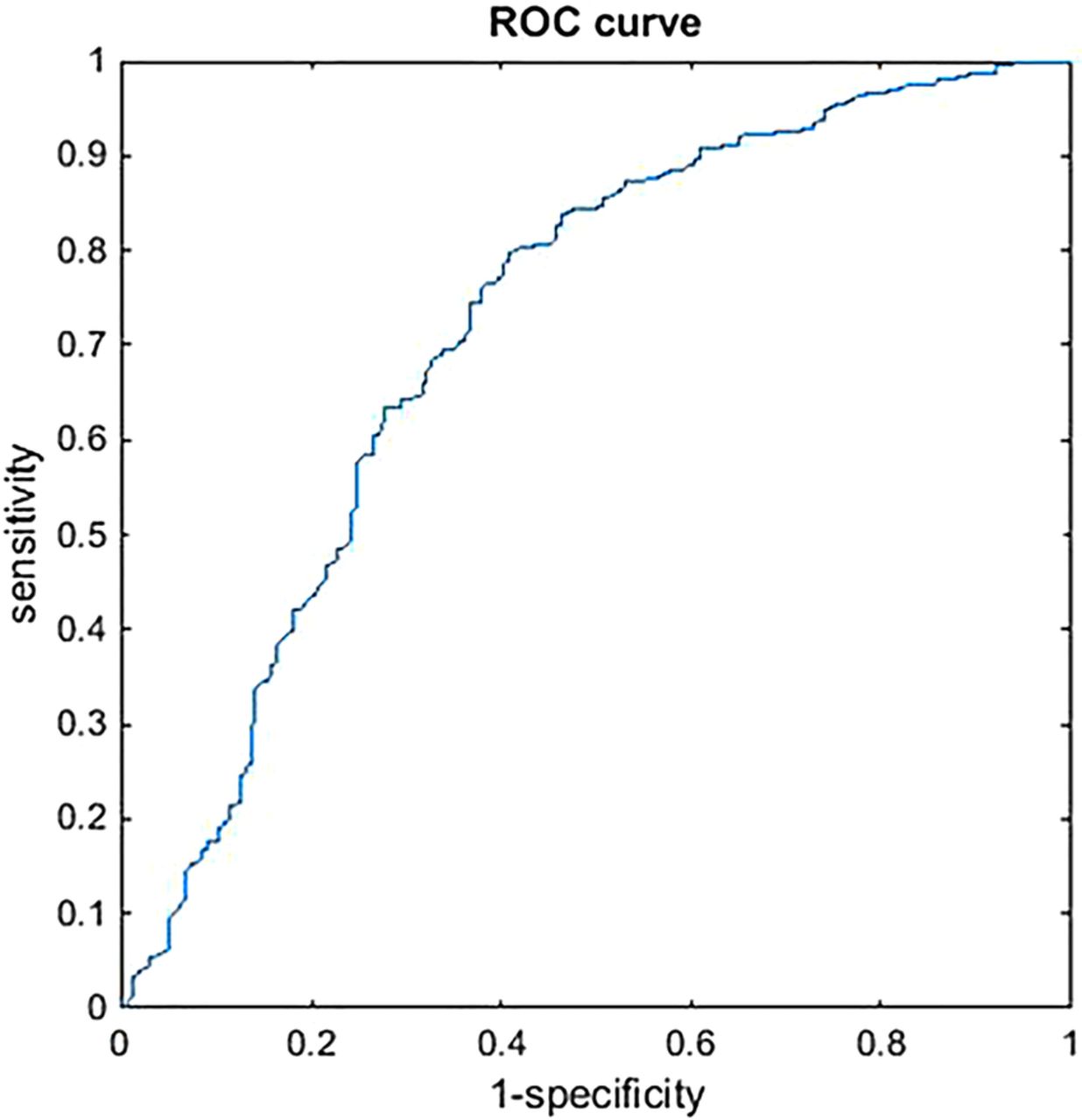
The three separate analyses sets were comparable. After adjustment for age, sex and BMI, the same structural abnormalities were observed to discriminate symptomatic OA best. The AUC for the three sets were 0.719, 0.698 and 0.693 (figure 2). Figure 3 illustrates the structural abnormalities best discriminating symptomatic knee OA.

ROC curve of one of the three analyses sets (set 1, AUC=0.7189). The ROC curves of set 2 and set 3 were comparable (AUC set 2=0.698, AUC set 3=0.693). AUC, area under the curve; ROC, receiver operating characteristic.
{kind=link}
{kind=link}
{kind=link}
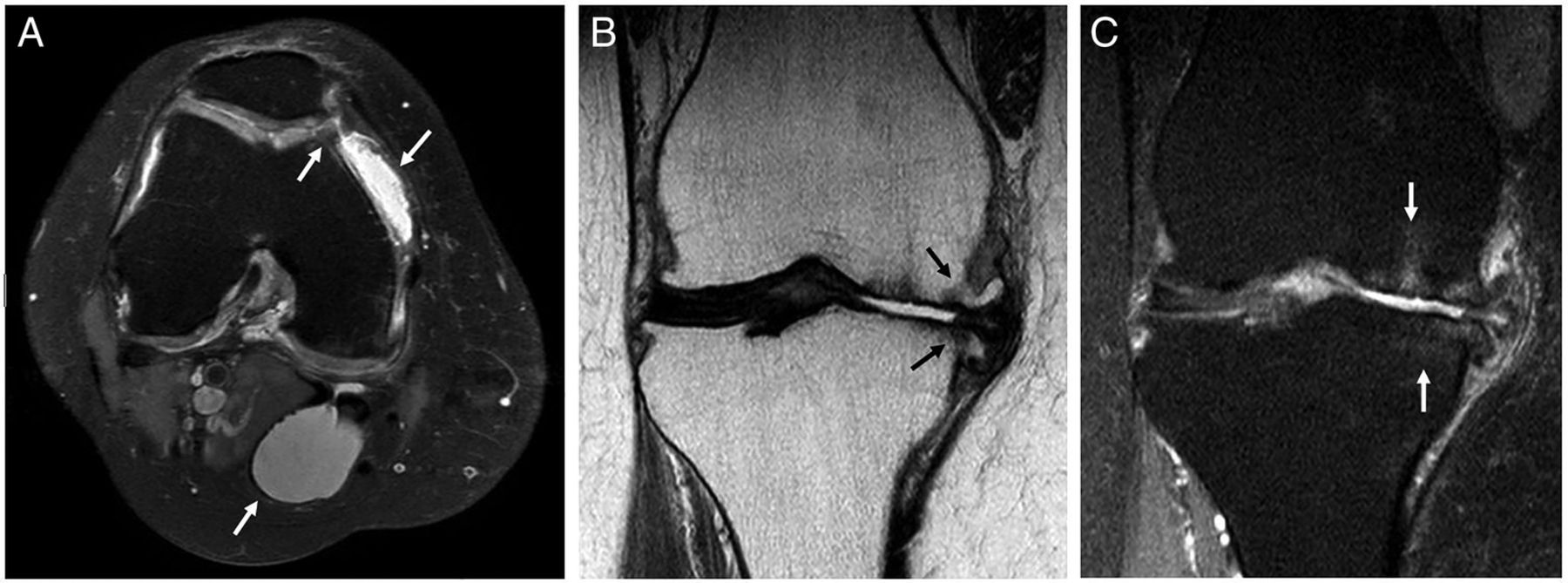
MRI in individuals with symptomatic knee osteoarthritis illustrating the structural abnormalities that discriminate symptomatic knee osteoarthritis best. (A) Axial fat suppressed proton density (PD) MRI showing a Baker's cyst, effusion and an osteophyte in the medial trochlear facet. (B) Coronal PD MRI showing osteophytes in the medial femoral condyle and medial tibial plateau. (C) Coronal fat suppressed PD MRI showing BMLs in the medial femoral condyle and medial tibial plateau. BML, bone marrow lesions.
Discussion
This large population-based study investigates which structural abnormalities as assessed on MRI discriminate symptomatic OA within the same knee best, taking co-occurrence of all structural abnormalities at different locations within the joint into account. In the entire study population, comprising individuals with and without symptomatic OA, structural abnormalities were highly frequent in the tibiofemoral and patellofemoral compartments, most prominent at the medial side. Presence of osteophytes and cartilage defects in different locations were related to each other. The structural abnormalities that discriminate best between individuals with and without symptomatic OA were general abnormalities as Baker's cysts and effusion, in addition to osteophytes and BMLs in the medial tibiofemoral compartment. In the patellofemoral joint, only osteophytes in the medial trochlear facet seemed of importance.
This is not the first study associating structural abnormalities with symptomatic knee OA or symptoms as pain, but it is the first one investigating this relationship involving structural abnormalities in all patellofemoral and tibiofemoral locations, using a model taking co-occurrence of all abnormalities into account.
Baker's cysts showed the highest regression coefficient for symptomatic OA. The relationship between Baker's cysts and OA symptoms has been assessed in a few studies that show conflicting results.11 ,19–21 Bakers’ cysts have not been studied before to discriminate symptomatic OA. Inflammation seems to play a role in development of Baker's cysts since the presence and grade of synovial inflammation has been associated with Baker's cysts.22 Although the grade of synovial inflammation has not been assessed in this study, since no contrast enhancement was used, effusion also discriminated symptomatic OA. The prevalence of grade 2 or 3 Baker's cysts was 23% in individuals with symptomatic OA compared to 9% in those without. Perhaps, treatment of knee OA has to focus on prevention of development of Baker's cysts by treatment of synovial inflammation. Studies on treatment of Baker's cysts by steroid injections showed a significant reduction of symptoms after intra-articular infiltration, and even more after direct injection into the cyst.23 ,24
As described in a systematic review on structural abnormalities in relation to symptoms in OA, the discriminative role of effusion and BMLs found in this study is in accordance with the previous literature.14 Osteophytes and cartilage defects do not show a clear relation with OA symptoms.14 This study, taking co-occurrence of structural abnormalities into account, showed osteophytes especially in the medial tibiofemoral joint to discriminate symptomatic OA. Although a high prevalence of cartilage defects was observed, they were found to discriminate symptomatic OA less well. This can be understood when looking at the network graph presented in figure 1, showing relations between structural abnormalities that co-occur frequently within the total study population. Since cartilage defects co-occur frequently with osteophytes, only one of these abnormalities will discriminate symptomatic OA when taking this co-occurrence into account.
The Baker's cyst, found to discriminate individuals with symptomatic OA best, was not present in the network graph. This is probably due to the lower prevalence of Baker's cysts. Although Baker's cysts also co-occur with other abnormalities in the knee, they especially discriminate symptomatic OA.
Although research on knee OA has been focusing increasingly on the patellofemoral compartment during past years,1 ,3 this study shows that most of the abnormalities discriminating symptomatic OA are general abnormalities (Baker's cysts and effusion) and structural abnormalities located within the medial tibiofemoral compartment. In the current literature on patellofemoral OA, it has been suggested that abnormalities in the patellofemoral compartment may represent an early stage of OA and precede tibiofemoral OA.25–27 This is in contrast with the minor role of the patellofemoral compartment in discriminating symptomatic OA found in this study.
The strengths of this study are the size of the study population and extensive assessment of structural abnormalities using MRI and analyses accounting for the co-occurrence of abnormalities at different locations within the joint. Symptoms as pain, assessed by self-report, may be influenced by unknown determinants or causes other than OA. Moreover, we lacked information on medication taken by the participants. Therefore, we used symptomatic OA defined by highly sensitive and specific criteria10 instead of only pain as the outcome measure.
Owing to the large number of individuals without symptomatic OA, the logistic ridge regression analyses were performed in three sets of data, consisting of a random one-third of individuals without symptomatic OA in addition to the individuals with symptomatic OA. Analyses of these three sets prevent loss of information due to the high proportion of individuals without OA. Furthermore, abnormalities that were found to discriminate symptomatic OA in all three sets support the importance of especially these abnormalities. The AUC of the three analyses (around 0.7) showed that assessment of all structural abnormalities results in fair discrimination of symptomatic OA.28
Although there was an oversampling of persons with overweight or obesity in our study population, obesity is not likely to influence the results since adjustment for BMI did not alter the results. Chondrocalcinosis can co-occur with OA,29 which could result in pseudogout and pain. However, on MRI, chondrocalcinosis is not assessed and could therefore not be included in our analysis.
This study suggests that Baker's cysts discriminate symptomatic knee OA best, followed by effusion and structural abnormalities as osteophytes and BMLs, especially on the medial side of the tibiofemoral joint. More research is necessary to gain more insight into the precise underlying mechanisms; longitudinal research will be of help. The role of Baker's cysts especially in symptomatic OA may provide potential targets for treatment of knee OA.
Acknowledgments
The authors express their gratitude to all the individuals who participated in the Netherlands Epidemiology in Obesity study. The authors are grateful to all participating general practitioners for inviting eligible participants. The authors furthermore thank all research nurses for collection of data and I. de Jonge, MSc for all data management of the NEO study.
References
Footnotes
Contributors AWV performed the statistical analysis, interpreted the data and drafted the manuscript. BM performed the statistical analysis, interpreted the data and revised the manuscript for important intellectual content. MR, SLC and FRR participated in the study design and revised the manuscript for important intellectual content. MR and JLB contributed to the acquisition of data and revised the manuscript for important intellectual content. MK participated in the study design, was involved in analysing and interpreting the data and in drafting and revising the manuscript. All authors read and approved the final version of the manuscript.
Funding The NEO study is supported by the Dutch Arthritis Foundation (project number 10-1-309), the participating Departments, the Division and the Board of Directors of the Leiden University Medical Center, and by the Leiden University, Research Profile Area ‘Vascular and Regenerative Medicine’.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Leiden University Medical Center.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.